Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Acides Gras Oméga-3 et Santé
Yvon A. Carpentier Laboratoire de Chirurgie Expérimentale ULB Clinique des Lipides Hôpital Erasme

2
Structure et nomenclature des acides gras
H3C COOH 18:0 Acide stéarique 9 H3C COOH 18:1n-9 Acide oléique H3C COOH 18:2n-6 Acide linoléique 6 3 H3C COOH 18:3n-3 Acide a-linolénique

3
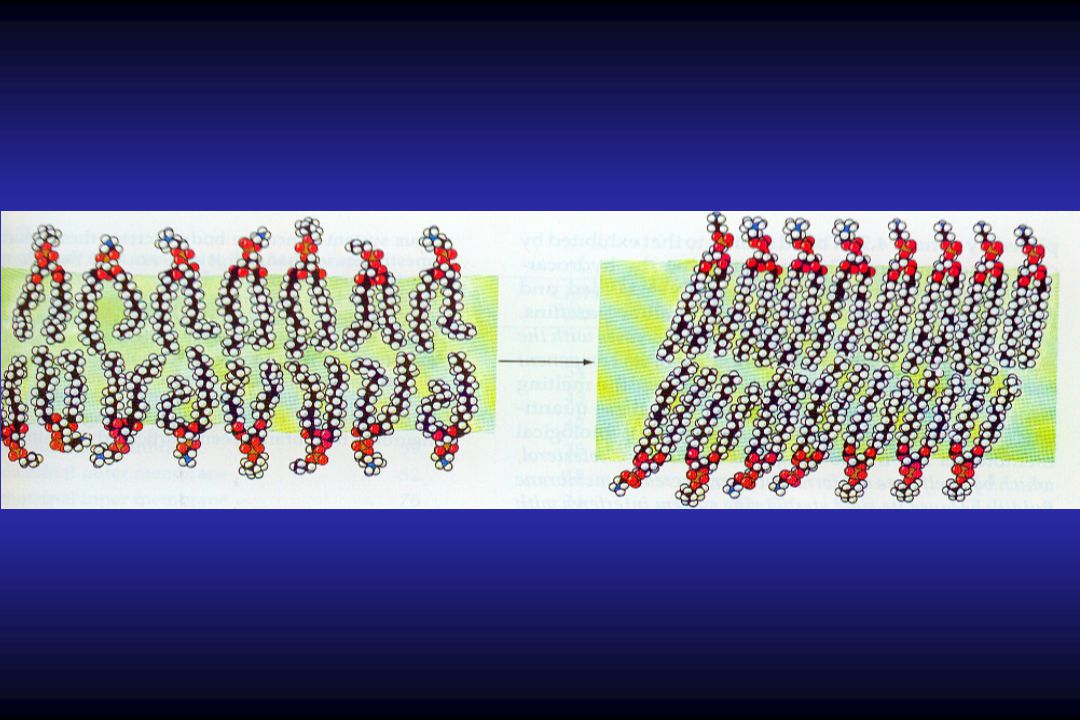
Solide à température ambiante vs. Liquide à température ambiante

5
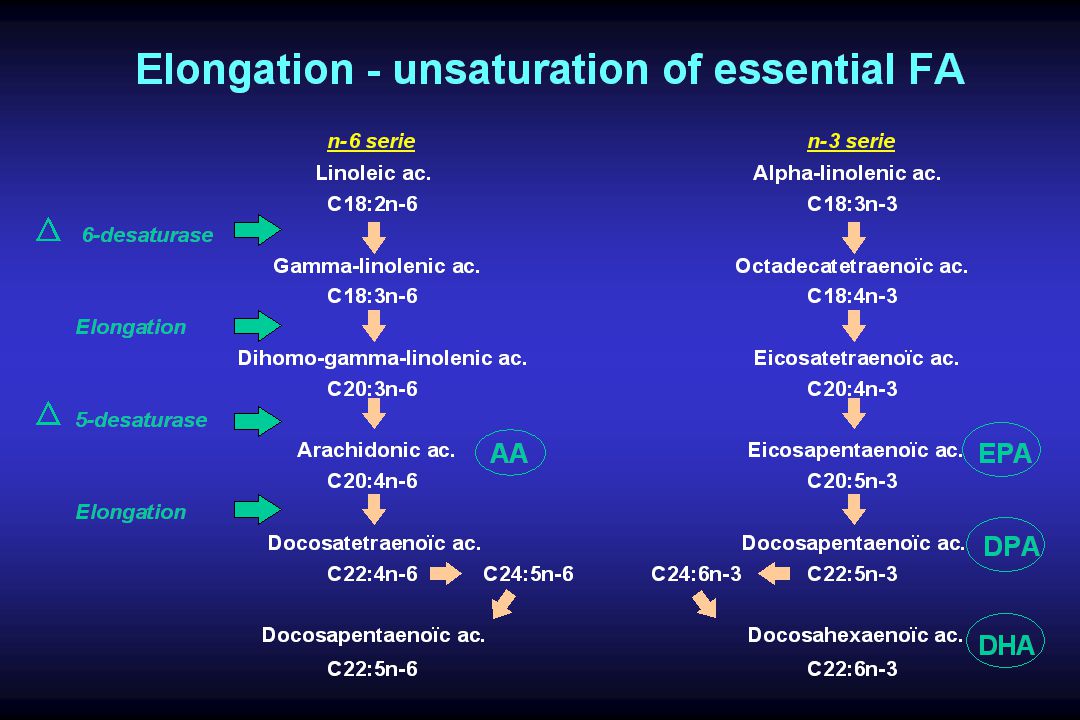
Metabolism of -linolenic acid
From Cunnane SC, J Physiol Pharmacol, 1996

6
Trends in the intake of fatty acids in the UK
% Energy PUFA to SFA ratio 1 0.8 0.6 0.4 0.2 50 40 30 20 10 Total fat SFA MUFA PUFA

7
Last 30 Years - Large Increase in the Intake of n-6 PUFAs in Industrialized Countries
Between 1972 and 1998 the n-6 fatty acids rose from 4% to 6%. Upsurge of Asthma in the UK, Australia, New Zealand and Germany might be a related phenomenon. The unexplained increase in the incidence of edema, allergic rhinitis, and regional differences of inflammatory diseases within countries may relate to increased n-6 fatty acid intake. Roberts 1991, Dept. of Health UK 1994, Black and Sharp 1997, Lewis et al. 1996, Grimble 1998 Fü-Out-13b

8
Evolution des habitudes alimentaires
Paléolithique « Western » AHA Lipides (% cal) <30 Sat (% cal) < ~ <10 P:S ~ >1.0 -3/ /1-1/ /10-1/ /1-1/5 Fibres (g/j) ~ ~ >25
 <30. Sat (% cal) <10 ~13 <10. P:S 1.4 ~0.5 >1.0. -3/ -6 1/1-1/2 1/10-1/20 1/1-1/5. Fibres (g/j) ~46 ~20 >25.")
9
DONNEES EPIDEMIOLOGIQUES
Populations consommant bcp AG n-3 faible incidence de pathologies cardiovasculaires faible incidence de pathologies inflammatoires et allergiques faible incidence de cancers (colon, sein, prostate) faible incidence de lithiases rénales faible incidence de diabète type I allongement de durée de gestation incidence accrue d’insuffisance rénale chronique CORRELATION AVEC COMPOSITION EN ACIDES GRAS DES MEMBRANES CELLULAIRES ET FORMATION EICOSANOIDES
 faible incidence de lithiases rénales. faible incidence de diabète type I. allongement de durée de gestation. incidence accrue d’insuffisance rénale chronique. CORRELATION AVEC COMPOSITION EN ACIDES GRAS DES. MEMBRANES CELLULAIRES ET FORMATION EICOSANOIDES.")
10
Rôles-clés en Santé Humaine
Acides Gras oméga-3 Rôles-clés en Santé Humaine Développement cognitif Développement vision Réponses immunes/inflammatoires Grossesses & développement foetal Maladies neurodégénératives Aspects psychologiques Maladies cardio-vasculaires

12
Modes and sites of action of n-3 PUFA’s
Formation of eicosanoids (tissue level, locally and at distance)
")
13
Membrane Pool (PL) Metabolic Pool (TG, FFA)
- isoprostanes 2 Metabolic Pool (TG, FFA) 18:2 n :3 n :3 n :4 n-6 (LA) (GLA) (DGLA) (AA) Cyclo - oxygenase Lipoxygénases PGE 1 LT HETES PGI TXA 2 PGE 4 2 2
 18:2 n-6 18:3 n-6 20:3 n-6 20:4 n-6. (LA) (GLA) (DGLA) (AA) Cyclo. - oxygenase. Lipoxygénases. PGE. 1. LT. HETES. PGI. TXA. 2. PGE")
14
A major role of arachidonic acid is as a precursor for eicosanoids
Arachidonic acid in cell membrane phospholipid Phospholipase A2 Free arachidonic acid COX LOX 12-LOX LOX PGG2 15-HPETE 12-HPETE 5-HPETE PGH2 15-HETE 12-HETE LTA4 5-HETE PGD2 LXA4 LTC4 LTB4 PGE2 PGF2a LTD4 LTE4 PGI2 TXA2

15
(ALA) (EPA) (DGLA) (DHA)
Membrane Pool (PL) F3 - and F4 - isoprostanes Metabolic Pool (TG, FFA) 18:3 n :5 n :5 n :6 n-3 (ALA) (EPA) (DGLA) (DHA) Cyclo - oxygénases Lipoxygenases TXA3 LT5 PGI3 PGE3
 F3 - and F4 - isoprostanes. Metabolic. Pool (TG, FFA) 18:3 n-3 20:5 n-3 22:5 n-3 22:6 n-3. (ALA) (EPA) (DGLA) (DHA) Cyclo. - oxygénases. Lipoxygenases. TXA3. LT5. PGI3. PGE3.")
16
Eicosanoids derived from n-3 (vs. n-6) PUFAs
Less inflammatory Less thrombogenic Less chemo-attractive Weaker protection of gastro-intestinal mucosa Retard delivery (increase pregnancy duration)
")
17
Classic view of the anti-inflammatory action of long chain w-3 PUFA
Arachidonic acid in membrane phospholipids DHA EPA Phospholipase A2 Free arachidonic acid 5-LOX COX-2 2-series PG and TX 4-series LT Inflammatory effects Inflammatory effects

18
Resolvins & related compounds
EPA DHA COX-2 (& presence of aspirin) E-series resolvins D-series resolvins, neuroprotectins etc. Anti-inflammatory; inflammation resolving
 E-series resolvins. D-series resolvins, neuroprotectins etc. Anti-inflammatory; inflammation resolving.")
20
Possible sites of action of n-3 & n-6 PUFAs
From J.A. Ross et al, Curr Opin Clin Nutr Metab Care, 1999

21
Modes and sites of action of n-3 PUFA’s
Formation of eicosanoids (tissue level, locally and at distance) Components of membrane phospholipids (membrane physical properties & interaction with membrane proteins : cell level) Second messengers in signalling pathways (molecular level) Regulators of gene expression (transcription factors : molecular level)
 Components of membrane phospholipids. (membrane physical properties & interaction with membrane proteins : cell level) Second messengers in signalling pathways. (molecular level) Regulators of gene expression. (transcription factors : molecular level)")
22
Signalisation cellulaire: voie des MAP-Kinases

23
Chemotaxis Chemoattractants Adhesion Injury Eicosanoids Cytokines Inflammation Reactive species PAF

24
Nutrition et Pathologies Cardio-vasculaires
Lipides plasmatiques Pression artérielle Tendance aux thromboses Résistance à insuline Oxydation Homocystéine Inflammation Fonction endothéliale Irritabilité ventriculaire NUTRITION MCV From WC Willett, 2004

25
Acides Gras Oméga 3 et le Coeur
triglycérides (4g/j) arythmies arrêts cardiaques réactions inflammatoires coagulation Synergie avec l’aspirine Pas d’effets secondaires Pas d’effet sur le cholestérol morbidité et mortalité des maladies coronaires
 arythmies. arrêts cardiaques. réactions inflammatoires. coagulation. Synergie avec l’aspirine. Pas d’effets secondaires. Pas d’effet sur le cholestérol. morbidité et mortalité des maladies coronaires.")
26
The New England Journal of Medicine
Volume May 9, Number 19 THE INVERSE RELATION BETWEEN FISH CONSUMPTION AND 20-YEAR MORTALITY FROM CORONARY HEART DISEASE Daan KROMHOUT, PH.D., M.P.H., EDWARD B., BOSSCHIETER, M.D., AND COR DE LEZENNE COULANER, M.SC. 1960: town of Zutphen, the Netherlands 852 middle-aged men without CHD dietary history 20 year follow-up: 78 deaths from CHD (> 50%) mortality from CHD in subjects eating > 30 g fish/day
 mortality from CHD in subjects eating > 30 g fish/day.")
27
Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction : diet and reinfarction trial (DART) M.L. Burr et al., The Lancet, 1989 2033 men having recovered from myocardial infarction (M.I.) Dietary intervention in secondary prevention of M.I. I fat intake (to 30% energy intake) and P/S ratio (to 1.0) II fatty fish intake ( g/week) III. cereal fibre intake (18g/day) 2 year follow-up : 29% REDUCTION OF MORTALITY (all causes) IN ‘‘FISH’’ GROUP II
 Dietary intervention in secondary prevention of M.I. I. fat intake (to 30% energy intake) and P/S ratio (to 1.0) II. fatty fish intake ( g/week) III. cereal fibre intake (18g/day) 2 year follow-up : 29% REDUCTION OF MORTALITY (all causes) IN ‘‘FISH’’ GROUP II.")
28
Dietary intake and cell membrane levels of long-chain n-3 Polyunsaturated Fatty Acids and the risk of primary cardiac arrest D.C. Siscovick et al. « Compared with no dietary intake of eicosapentaenoic acid (C20:5n-3) and docosahexaenoic acid (C22:6n-3), an intake of 5.5 g of n-3 fatty acids per month (... equivalent of one fatty fish meal per week) was associated with a 50% reduction in the risk of primary cardiac arrest (odds ratio [OR], 0.5; 95% confidence interval [Cl], 0.4 to 0.8), after adjustment for potential confounding factors. » JAMA, 1995
 and docosahexaenoic acid (C22:6n-3), an intake of 5.5 g of n-3 fatty acids per month (... equivalent of one fatty fish meal per week) was associated with a 50% reduction in the risk of primary cardiac arrest (odds ratio [OR], 0.5; 95% confidence interval [Cl], 0.4 to 0.8), after adjustment for potential confounding factors. » JAMA,")
29
Prevention and termination of arrhythmia by EPA
J.X. Kang & A. Leaf, Proc Natl Acad Sci USA, 1994

30
Prevention of Sudden Cardiac Death by Dietary Pure w-3 Polyunsaturated Fatty Acids in Dogs
Dog model of cardiac sudden death surgically, large myocardial infarct + inflatable cuff around left circumflex coronary art. (LCA) 1 month later: Treadmill running + LCA occlusion Ventricular fibrillation and death in all controls & soybean oil (n = 7) Survival in 5/7 dogs infused for 1h with EPA 6/8 dogs infused for 1h with DHA 6/8 dogs infused for 1h with LNA G.E. Billman et al, Circulation, 1999
 1 month later: Treadmill running + LCA occlusion. Ventricular fibrillation and death in all controls & soybean oil (n = 7) Survival in 5/7 dogs infused for 1h with EPA. 6/8 dogs infused for 1h with DHA. 6/8 dogs infused for 1h with LNA. G.E. Billman et al, Circulation,")
31
Résultats - Suppl. HP vs. 2 autres groupes:
Association of n-3 polyunsaturated fatty acids with stability of atherosclerotic plaques : a randomised controlled trial 188 patients en attente endartériectomie carotide (7-189j) Suppl. HP (1.4g EPA/DHA/j) vs. Tournesol vs. Palme/Soja Résultats - Suppl. HP vs. 2 autres groupes: EPA & DHA dans lipides de plaque ( incorporation avec temps) Plus de plaques avec couche fibreuse épaisse Moins de plaques avec couche fibreuse fine & inflammatoire Moins d’infiltration de macrophages dans plaques t/o rapide des acides gras dans lipides des plaques effet marqué de suppl. HP sur morphologie & fragilité des plaques F. Thies et al, The Lancet, 2003
 Suppl. HP (1.4g EPA/DHA/j) vs. Tournesol vs. Palme/Soja. Résultats - Suppl. HP vs. 2 autres groupes: EPA & DHA dans lipides de plaque ( incorporation avec temps) Plus de plaques avec couche fibreuse épaisse. Moins de plaques avec couche fibreuse fine & inflammatoire. Moins d’infiltration de macrophages dans plaques. t/o rapide des acides gras dans lipides des plaques. effet marqué de suppl. HP sur morphologie & fragilité des plaques. F. Thies et al, The Lancet,")
32
Dietary Fish Oil Supplementation Reduces Myocardial Infarct Size in a Canine Model of Ischemia and Reperfusion 0.06 g/kg.day EPA for 6 weeks Occlusion of left circumflex coronary art. for 90 min followed by 6h of reperfusion Infarct size: 13.3% (w 3) vs 29.7% (control) (p<0.05); no difference in regional blood flow or oxygen consumption Protective mechanisms: inhibition of TXA2 inhibition of free radical production by leucocytes? H. J. Oskarsson et al., J Am Coll Cardiol, 1993
 vs 29.7% (control) (p<0.05); no difference in regional blood flow or oxygen consumption. Protective mechanisms: inhibition of TXA2. inhibition of free radical production by leucocytes H. J. Oskarsson et al., J Am Coll Cardiol,")
33
Acides Gras -3 et Endothélium
Amélioration profil lipoprotéines Amélioration profil éicosanoïdes Effet sur membranes cellulaires (et Chol dans cavéoles) Modulation de facteurs de transcription nucléaire Amélioration défenses anti-oxidantes de cellule vasorelaxation coagulation, act plaquettes & molécules adhésion sensibilité aux cytokines & radicaux libres activation CML
 Modulation de facteurs de transcription nucléaire. Amélioration défenses anti-oxidantes de cellule. vasorelaxation. coagulation, act plaquettes & molécules adhésion. sensibilité aux cytokines & radicaux libres. activation CML.")
34
BENEFICIAL EFFECTS OF n-3 PUFA ( I )
essential for maturation of foetal CNS and retina (DHA) reduce inflammatory response anti-thrombotic effect prevent impaired cellular immunity when caused by PGE2 production decrease plasma triglyceride concentration (also post-prandial) decrease plasma free fatty acid concentration (also p-prandial)
 reduce inflammatory response. anti-thrombotic effect. prevent impaired cellular immunity when caused. by PGE2 production. decrease plasma triglyceride concentration (also post-prandial) decrease plasma free fatty acid concentration (also p-prandial)")
35
BENEFICIAL EFFECTS OF n-3 PUFA ( II )
decrease cell reactivity to various stimuli (e.g. ventricular arrhythmia’s,...) prevent / reverse cancer & inflammatory cachexia increase tolerance to organ transplantation and improve function of the graft help maintaining adequate tissue microperfusion reduce cellular accumulation of fat (e.g., liver) potential interest for supplying n-3 PUFA to « acute » patients
 prevent / reverse cancer & inflammatory cachexia. increase tolerance to organ transplantation and improve function of the graft. help maintaining adequate tissue microperfusion. reduce cellular accumulation of fat (e.g., liver) potential interest for supplying n-3 PUFA to « acute » patients.")
36
Limitations to n-3 FA supply with Fish Oils
Gastro-intestinal administration FO TG : poor substrate for pancreatic lipase slow & rather unefficient absorption Intravenous infusion FO TG : poor substrate for lipoprotein lipase slow plasma elimination ! a proportion of n-3 FA used for oxidative purposes !

38
Obésité, syndrome métabolique, et insulino-résistance
Influence du patrimoine génétique 85% des diabétiques T2 sont obèses 30% des obèses sont diabétiques (T2) prévalence Différences entre ethnies (NB: asiatiques) Influence facteurs comportementaux (nutrition, activité physique, …) Relation avec stress & inflammation
 prévalence. Différences entre ethnies (NB: asiatiques) Influence facteurs comportementaux (nutrition, activité physique, …) Relation avec stress & inflammation.")
39
Le Syndrome Métabolique
Combinaison de 3 facteurs: - obésité abdominale : tour taille > 94 cm (H) ou > 80 cm (F) - conc. triglycérides 1.7 mmol/L (150 mg/dL) ou traitt - conc. HDL-cholestérol < 1.03 mmol/L (40 mg/dL) H ou traitt < 1.28 mmol/L (50 mg/dL) F ou traitt - tension artérielle 130/85 mm Hg ou traitt - conc. glucose à jeun 5.56 mmol/L (100 mg/dL) ou traitt prévalence: 44% pour population USA > 50 ans (2003) prévalence coronaropathies (>> facteurs isolés)
 ou > 80 cm (F) - conc. triglycérides 1.7 mmol/L (150 mg/dL) ou traitt. - conc. HDL-cholestérol < 1.03 mmol/L (40 mg/dL) H ou traitt. < 1.28 mmol/L (50 mg/dL) F ou traitt. - tension artérielle 130/85 mm Hg ou traitt. - conc. glucose à jeun 5.56 mmol/L (100 mg/dL) ou traitt. prévalence: 44% pour population USA > 50 ans (2003) prévalence coronaropathies (>> facteurs isolés)")
40
FACTEURS ASSOCIES AU SYNDROME METABOLIQUE
Insulino-résistance & risque diabète T2 Dépôts ectopiques de TAG (foie, muscles, … ) Altérations lipoprotéines (sd LDL athérogènes) Composante inflammatoire Dysfonction endothéliale activité ortho-sympathique Etiologie multiple (nutrition, sédentarité, …)
 Altérations lipoprotéines (sd LDL athérogènes) Composante inflammatoire. Dysfonction endothéliale. activité ortho-sympathique. Etiologie multiple (nutrition, sédentarité, …)")
41
Serum sialic acid concentration in 263 overweight women without (0) or with 1-3 other features of metabolic syndrome : insulin resistance; dyslipidemia; hypertension L. Browning, Proc Nut Soc, 2003

42
Gene variants, insulin resistance, and dyslipidaemia
Hypotheses: primary effect of variants on insulin resistance or on dyslipidaemia M.Lakso, Curr Opin Lipidol, 2004

43
Interaction between dietary lipids and physical inactivity on insulin sensitivity and on intramyocellular lipids in healthy men 8 healthy male volunteers 60h complete bed rest + high fat or high CHO diet Hyperinsulinemic –euglycemic clamp (glucose disposal) 1H-magnetic resonance spectroscopy Bed rest + high fat : glucose disposal (- 24%) intramyocellular lipid content (+ 32%) R. Stettler et al, Diabetes Care, 2005
 1H-magnetic resonance spectroscopy. Bed rest + high fat : glucose disposal (- 24%) intramyocellular lipid content (+ 32%) R. Stettler et al, Diabetes Care,")
45
Mitochondrial dysfunction and type 2 diabetes
Maintenance of normal glucose level : insulin responsiveness of skeletal muscle & liver defect insulin resistance insulin secretion by pancreatic beta cells defect hyperglycemia both defects may be caused by mitochondrial dysfunction Lowell BB & Shulman GI, Science, 2005

46
Insulin resistance associated to obesity and type 2 diabetes
Molecular defects of insulin signaling in muscle glucose disposal and transport (role of fatty acids & metabolites) Insulin resistance in liver glucose output (overexpression of glucose-6-Pase) Visceral obesity & ectopic fat storage (e.g., muscle & liver) poor modulation of fat oxidation Non-alcoholic fatty liver disease (NAFLD) and steato-hepatitis (NASH) lipolysis, oxidative stress, cytokine induction Altered activity of desaturases 9 & 5 6 desaturase DB Savage et al, Hypertension, 2005
 Insulin resistance in liver. glucose output (overexpression of glucose-6-Pase) Visceral obesity & ectopic fat storage (e.g., muscle & liver) poor modulation of fat oxidation. Non-alcoholic fatty liver disease (NAFLD) and steato-hepatitis (NASH) lipolysis, oxidative stress, cytokine induction. Altered activity of desaturases. 9 & 5 6 desaturase. DB Savage et al, Hypertension,")
47
N-3 long chain polyunsaturated fatty acids: a nutritional tool to prevent insulin resistance associated to type 2 diabetes and obesity ? RAT STUDIES N-3 PUFAs improve molecular defects of insulin signaling in muscle IRS-1 phosphorylation PI 3’-kinase act, GLUT-4 mRNA muscle TAG content & LCFA CoA N-3 PUFAs improve insulin resistance in liver expression & activity of G-6-Pase; normalize glucose output N-3 PUFAs improve visceral obesity & ectopic fat storage (muscle & liver) fat oxid (PPAR) lipogenesis, TG formation, & fat deposition
 fat oxid (PPAR) lipogenesis, TG formation, & fat deposition.")
48
N-3 long chain polyunsaturated fatty acids: a nutritional tool to prevent insulin resistance associated to type 2 diabetes and obesity ? HUMAN STUDIES (Healthy volunteers) 3 week supplementation w FO (1.1 g EPA g DHA) Oral glucose load (after supplementation n-3 PUFA) : insulin response (- 40%) glycemic response glucose oxidation lipid oxidation glycogen storage N.B.: no effect after short-term supplementation (need for n-3 FA incorporation in cell membranes ?) J. Delarue et al, Reprod Nutr Dev, 2004
 3 week supplementation w FO (1.1 g EPA g DHA) Oral glucose load (after supplementation n-3 PUFA) : insulin response (- 40%) glycemic response. glucose oxidation. lipid oxidation. glycogen storage. N.B.: no effect after short-term supplementation (need for n-3 FA incorporation in cell membranes ) J. Delarue et al, Reprod Nutr Dev,")
49
Changes in AUC for insulin (final-baseline) after supplementation with n-3 PUFA vs. placebo in premenopausal non-diabetic subjects P < 0.05 Subjects : - age : years - BMI : kg/m2 Inflammatory status (IS) : - low IS : sialic acid < 2.00 mM - high IS : sialic acid > 2.20 mM L. Browning, Proc Nut Soc, 2003
 : - low IS : sialic acid < 2.00 mM. - high IS : sialic acid > 2.20 mM. L. Browning, Proc Nut Soc,")
50
Fish oil prevents the adrenal activation elicited by mental stress in healthy men
7 healthy volunteers 2 tests of mental stress, before & after suppl 7.2g FO/d (3wks) Before: heart rate blood pressure energy expenditure plasma cortisol plasma epinephrine plasma NEFAs After n-3 PUFA supplementation : heart rate blood pressure energy expenditure plasma cortisol plasma epinephrine plasma NEFAs blunting of sympatho-adrenal stimulation (at CNS level ?) potential role in prevention of insulin resistance J. Delarue et al, Diabetes Metab, 2003
 Before: heart rate blood pressure energy expenditure. plasma cortisol plasma epinephrine plasma NEFAs. After n-3 PUFA supplementation : heart rate blood pressure energy expenditure. plasma cortisol plasma epinephrine plasma NEFAs. blunting of sympatho-adrenal stimulation (at CNS level ) potential role in prevention of insulin resistance. J. Delarue et al, Diabetes Metab,")
51
Diabetogenic impact of long-chain omega-3 fatty acids on pancreatic beta-cell function and the regulation of endogenous glucose production Dietary saturated lipids in healthy subjects: ins resist but ins secretion glucose tolerance maintained Substitution 7% dietary lipids with n-3 PUFA (4 weeks): reverses peripheral insulin resistance (normal glucose disposal) HOWEVER: no suppression of hepatic insulin resistance no suppression glucose output no compensatory insulin secretion (+ direct impairment ?) glucose level MJ Holness et al, Endocrinology, 2003
: reverses peripheral insulin resistance (normal glucose disposal) HOWEVER: no suppression of hepatic insulin resistance. no suppression glucose output. no compensatory insulin secretion (+ direct impairment ) glucose level. MJ Holness et al, Endocrinology,")
52
Body weight modulates cholesterol metabolism in non-insulin dependent type 2 diabetics
BMI, serum insulin and/or blood glucose levels: cholesterol synthesis bile acid synthesis cholesterol excretion in bile cholesterol t/o cholesterol absorption serum cholestanol & plant sterols PP Simonen et al, Obes Res, 2002

53
Lipoprotein metabolism in the metabolic syndrome
Chylo LPL Chylo-R Visceral adipose tissue FA LPL CHO Apo B VLDL -TG VLDL TG FA FFA apoB CO2 IDL LDL Designed from PHR Barett & GF Watts, Curr Opin Lipidol, 2003

54
Visceral adipose tissue
Lipoprotein metabolism in the metabolic syndrome : Effects of n-3 PUFA supplementation Chylo LPL Chylo-R Visceral adipose tissue FA LPL CHO Apo B VLDL -TG VLDL TG FA FFA apoB CO2 IDL LDL Designed from PHR Barett & GF Watts, Curr Opin Lipidol, 2003

55
N-3 Fatty Acids and Plasma Lipoproteins
plasma triglycerides plasma VLDL-TG and VLDL-cholesterol or HDL-cholesterol, but apo A-1 LDL-cholesterol (generally slight) fraction of small dense LDL (phenotype B subjects)
 fraction of small dense LDL (phenotype B subjects)")
56
Dietary effects on postprandial triglyceride levels
SFA n-6 PUFA n-3 PUFA M. Weintraub et al, J Clin Invest, 1988

57
Differential effects of n-3 fatty acids
Mildly hyperlipidemic subjects - TAG conc. : 1.7g/d EPA+DHA > 9.5g/d ALA LDL sensitivity to oxidation with 1.7g EPA+DHA YE Finnegan et al, AJCN, 2003 - TAG conc. : comparable with 4g/d EPA and 4g/d DHA LDL size : only with 4g/d DHA forearm blood flow : only with 4g/d DHA TA Mori et al, AJCN & Circulation, 2000

58
48 obese insulin-resistant subjects
Regulatory effects of HMG CoA reductase inhibitor and Fish Oils on apolipoprotein B-100 kinetics in insulin-resistant obese male subjects with dyslipidemia 48 obese insulin-resistant subjects 6 wks Atorva 40mg vs Omacor 4g vs Atorva+Omacor EPA/DHA : plasma VLDL-apo B VLDL-apo B secretion VLDL to LDL conversion Atorva : plasma apo B lipoproteins FCR of VLDL-, IDL-, LDL-apo B Atorva + EPA/DHA : cumulative effects DC Chan, Diabetes, 2002

59
Healthy Swedish Subjects with mild hyperlipidaemia
(after 4 weeks of Mediterranean vs. Swedish diet) P < 0.05 P < 0.05 Swedish Mediterranean P < 0.05 P < 0.05 A. Ambring et al, Clin Sci, 2004
 P < P < Swedish. Mediterranean. P < P < A. Ambring et al, Clin Sci,")
60
Effect of weight loss and lifestyle changes on vascular inflammatory markers in obese women
Randomized single-blind trial ;120 premenopausal obese women (BMI ≥ 30) with no diabetes, hypertension, or hyperlipidemia Low energy mediterranean diet + physical activity vs. Healthy food + exercise K Esposito et al, JAMA, 2003
 with no diabetes, hypertension, or hyperlipidemia. Low energy mediterranean diet + physical activity vs. Healthy food + exercise. K Esposito et al, JAMA,")
61
Le Syndrome Métabolique: stratégie
Unique ? AG n-3 effet préventif, non thérapeutique, sur insulino-résistance inflammation défenses anti-oxydantes cellulaires (modérée) pression artérielle TAG HDL-chol sdLDL mais LDL-chol Globale nutrition : association avec AG saturés et AGMI (alimentation type méditerranéen) amélioration contrôle pondéral activité physique si indiquée, association à hypolipémiants
 pression artérielle. TAG HDL-chol sdLDL mais LDL-chol. Globale. nutrition : association avec AG saturés et AGMI. (alimentation type méditerranéen) amélioration contrôle pondéral. activité physique. si indiquée, association à hypolipémiants.")
62
Le syndrome métabolique : effets des fibres (FOS) chez le rat
satiété prises alimentaires absorption glucides & acides gras glycémie & triglycéridémie post-prandiales sécrétion insuline phénomènes inflammatoires (NFkB) possibilité effets complémentaires et/ou synergiques à ceux des AG w 3
 possibilité effets complémentaires et/ou synergiques à ceux des AG w 3.")
63
Delivery of DHA and EPA via alpha linolenic acid is not efficient Delivery of DHA and EPA via increased fish oil intake is very efficient Current intake of fish oil EPA and DHA in the USA is ~1/3 – 1/6 of recommended levels

64
General Conclusions and recommendations Fish and Omega-3 fatty acid intake
Clear benefits in secondary prevention Less strong evidence in primary prevention Include (fatty) fishes as part of healthy preventive diet Temporary limited intake in specific subgroups (pregnant women & children) Increased intake in other specific subgroups (high risk & hypertriglyceridaemia) Possibility to use (good quality) supplements
 fishes as part of healthy preventive diet. Temporary limited intake in specific subgroups. (pregnant women & children) Increased intake in other specific subgroups. (high risk & hypertriglyceridaemia) Possibility to use (good quality) supplements.")
65
Fish and Omega-3 fatty acid intake : The unanswered questions
Indications for primary prevention in high risk groups (renal failure, insulin-resistance, transplantation, …) ? Doses in different indications ? Effect of DHA vs. EPA ? Intake of ALA (and w3/w6 intake) ? Prevention of lipid peroxidation ? Optimising intestinal absorption & cell incorporation ?
 Doses in different indications Effect of DHA vs. EPA Intake of ALA (and w3/w6 intake) Prevention of lipid peroxidation Optimising intestinal absorption & cell incorporation")
Présentations similaires






 and associated factors in HIV-infected patients,>")











>")


 of, organic matter (OM), Neutral Detergent Fibre (NDF), Acid Detergent Fibre (ADF) and crude protein (CP) of the.>")
 et un plan horizontal (2). Les flèches indiquent les mouvements.>")