Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
b-lactamases à spectre étendu Les points clés pour le réanimateur
JR Zahar Microbiologie – Hygiène Hospitalière

2
Plan Données épidémiologiques Identification du réservoir
Proposition de gestion du risque

3
Beta lactamase à spectre étendu (BLSE) K pneumoniae
 K pneumoniae")
4
ESBL an old history Nosocomial outbreaks (1980 – 2000)
Predominantly K pneumoniae Nosocomial infections Intensive care unit Long prior hospitalisation Prior antibiotic therapy Catheters, mechanical ventilation, ….

5
How did we deal with this risk?
1990 – 2000, decreased prevalence of Kp ESBLs (+) (Paris AP/HP) from 15-20% to 2-3%
 (Paris AP/HP) from 15-20% to 2-3%")
6
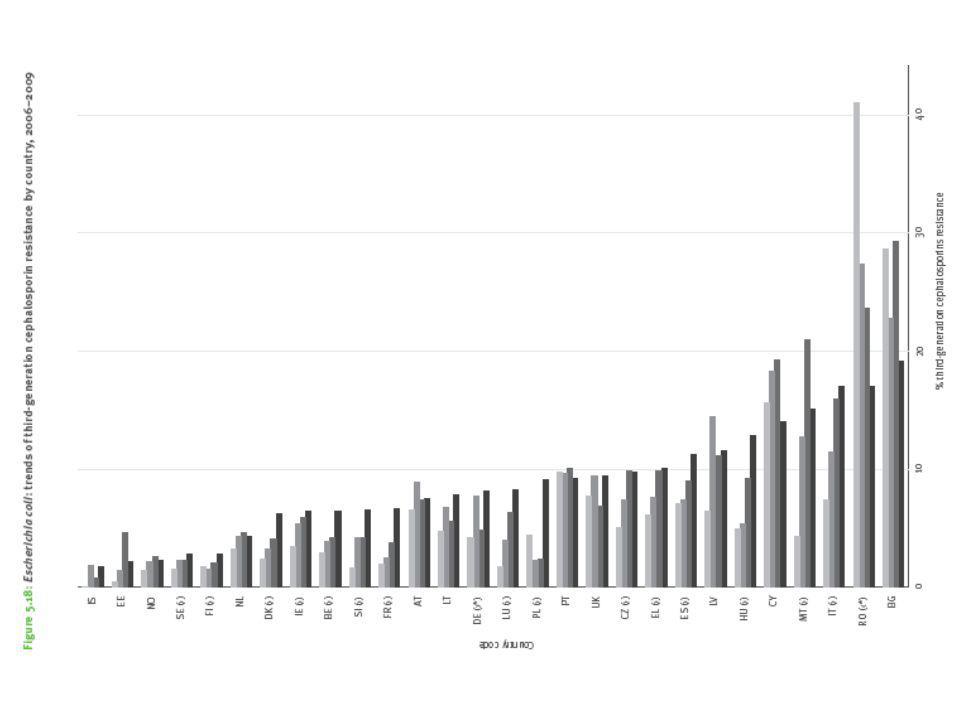
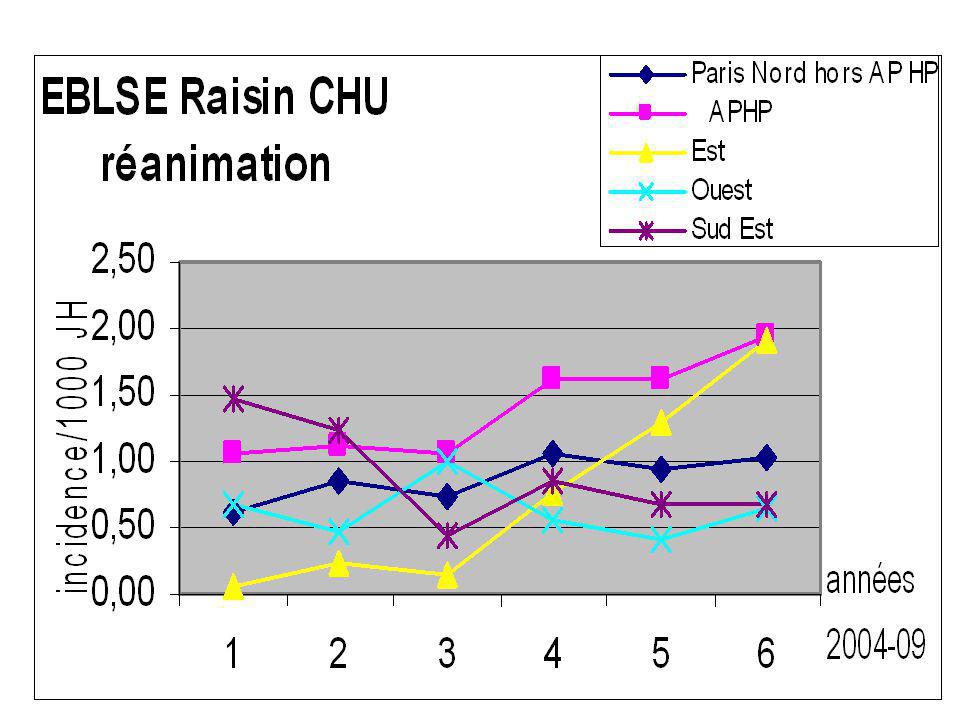
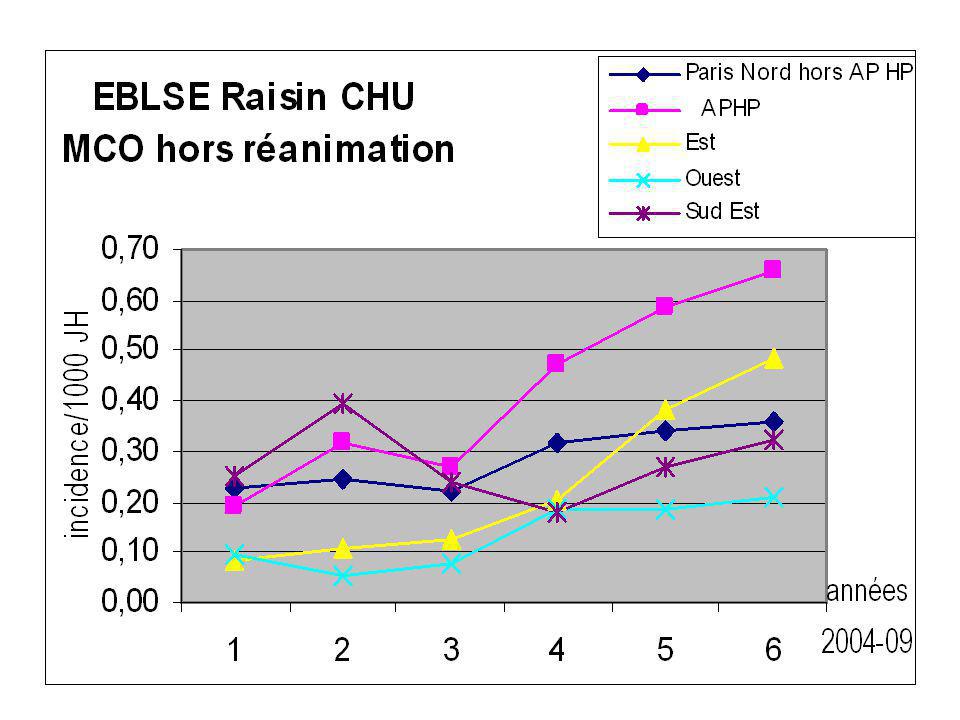
Diffusion des EBLSE

10
L’Hygiène expliquée à ma fille!
Le risque de transmission croisée augmente Pression de colonisation RESERVOIR VECTEUR PERSONNES EXPOSEES

13
En résumé Diffusion endémique des BLSE En milieu communautaire ++
Répercussion en milieu hospitalier Importance de la Pression de Colonisation

14
Can we identify carriers or infected patients?

15
Pour simplifier Deux types de porteurs/infectés Les Communautaires
Vrais Liés aux soins Les Nosocomiaux

16
Infected patients ? Risk factors asociated with bacteremia?
Case control study including 43 cases of ESBL E coli bacteremia 70% isolates with CTX-M plasmid 19% « really » community acquired Antibiotic therapy OR 6,6 ; IC 95 % (2,9 – 15) Cephalosporin III G OR 3,3 ; IC 95 % (1,2 – 9.1) Fluoroquinolones OR 6,4 ; IC 95 % (2,2 – 18,3) Rodriguez-Bano, Clin Microbiol Infect 2007
 Cephalosporin III G OR 3,3 ; IC 95 % (1,2 – 9.1) Fluoroquinolones OR 6,4 ; IC 95 % (2,2 – 18,3) Rodriguez-Bano, Clin Microbiol Infect")
17
Risk factors associated with ESBL E coli infected patients
Rodriguez-Bano et al, Clin Microbiol Infect 2007

18
Hospitalization < 3 months Antibiotic < 3 months
Infected patients ? Factors associated with community acquired (?) ESBL-PE UTI Propective study, including 128 ESBL and 183 non ESBL, UTI FDR OR IC 95% CSP II G 15.8 CSP III G 10.1 Hospitalization < 3 months 8.95 3.77 – 21.25 Fluoroquinolones 4.1 1.8 – 9.0 Penicillins 4.0 1.6 – 9.0 Antibiotic < 3 months 3.23 1.76 – 5.91 Âge>60 years 2.65 1.45 – 4.83 Diabetes 2.57 1.20 – 5.51 male 2.47 1.22 – 5.01 Klebsiella infection 2.31 4.54 Colodner, Eur J Clin Microbiol Infect Dis 2004, 23:163
 ESBL-PE UTI. Propective study, including 128 ESBL and 183 non ESBL, UTI. FDR. OR. IC 95% CSP II G CSP III G Hospitalization < 3 months – Fluoroquinolones – 9.0. Penicillins – 9.0. Antibiotic < 3 months – Âge>60 years – Diabetes – male – Klebsiella infection Colodner, Eur J Clin Microbiol Infect Dis 2004, 23:163.")
19
Calbo, J Antimicrobial Chemother 2006, 57; 780
Infected patients ? ESBL- E coli, UTI Case (19) – control (55) study 3:1 ratio to case patients according to age, sex, date of isolation and residence in a long-term care facility Univariate analysis Hospitalisation Prior UTI Urinary tract abnormality Prior antibiotic therapy with cefuroxime Multivariate analysis Antibiotic therapy (cefuroxime), OR =21,42 ; (IC 95 % 5,38 – 85,2) Calbo, J Antimicrobial Chemother 2006, 57; 780
 – control (55) study. 3:1 ratio to case patients according to age, sex, date of isolation and residence in a long-term care facility. Univariate analysis. Hospitalisation. Prior UTI. Urinary tract abnormality. Prior antibiotic therapy with cefuroxime. Multivariate analysis. Antibiotic therapy (cefuroxime), OR =21,42 ; (IC 95 % 5,38 – 85,2) Calbo, J Antimicrobial Chemother 2006, 57; 780.")
20
Risks factor associated with infection
65 patients infected by an ESBL- E coli CTX-M, compared to patients infected by an ESBL- E coli non-CTX-M 22/65 community acquired 64/65 urinary isolates Variable OR p Renal disease 8.4 0.0037 Diabetes 5.2 0.02 UTI 17.9 0.003 Community acquired 26.7 <0.0001 Surgery 7.1 0.028 Gynecological surgery 6.9 0.008 Urinary catheter 4.1 0.043 Lavigne, JCM 2007

21
Risks factors associated with infection
339 patients infected, 90,5% E coli and 65% CTX-M 34% with no recent hospital admission Variables OR p Age> 65 2.4 (1.6 – 3.6) <0.001 Recent use of antibiotic 1.8 (1.2 – 2.6) Recent hospitalisation 2.9 (1.9 – 4.4) Residence in LTF 7.5 (3.5 – 16.3) Male sex 2.5 (1.7 – 3.7) Ben Ami, Clin Inf Dis 2009
 < Recent use of antibiotic. 1.8 (1.2 – 2.6) Recent hospitalisation. 2.9 (1.9 – 4.4) Residence in LTF. 7.5 (3.5 – 16.3) Male sex. 2.5 (1.7 – 3.7) Ben Ami, Clin Inf Dis")
22
Risk factors of carriage
Prevalence study in a nursing home 119 (40,5%) with faecal samples growing with MDR E coli (49% CTX-M) 51% without recent hospital admission 13,5% « old carriers » Variable OR (95%CI) p Fluoroquinolone use 0.23 (0.04 – 1.23) 0.09 Fluoroquinolones use days 1.33 ( ) 0.02 History of UTI 2.56 (1.37 – 4.78) 0.003 Rooney, JAC 2009
 with faecal samples growing with MDR E coli (49% CTX-M) 51% without recent hospital admission. 13,5% « old carriers » Variable. OR (95%CI) p. Fluoroquinolone use (0.04 – 1.23) Fluoroquinolones use days ( ) History of UTI (1.37 – 4.78) Rooney, JAC")
23
Alors les infections sont elles si fréquentes !!!

24
My local epidemiology!! Bacteremia in 12 French hospitals
Prospective study, including all GNB bacteremia isolated within the 48 hours after admission 16% of the isolates where resistant to CSP third generation (except Ceftazidim) 3,5% ESBL Michka Shoai Tehrani , submitted
 3,5% ESBL. Michka Shoai Tehrani , submitted.")
25
Prélèvements cliniques et EBLSE
CHU Necker- Enfants Malades

26
Others risk factors …..?

27
Risk factors of carriage
Prospective study Faecal carriage in outpatients with UTI and their Household members Faecal carriage was 67,9% in outpatients with UTI 27.6% in household members 15,4% in non-household relatives 7.4% in the control group Rodriguez-Bano, JAC 2009

28
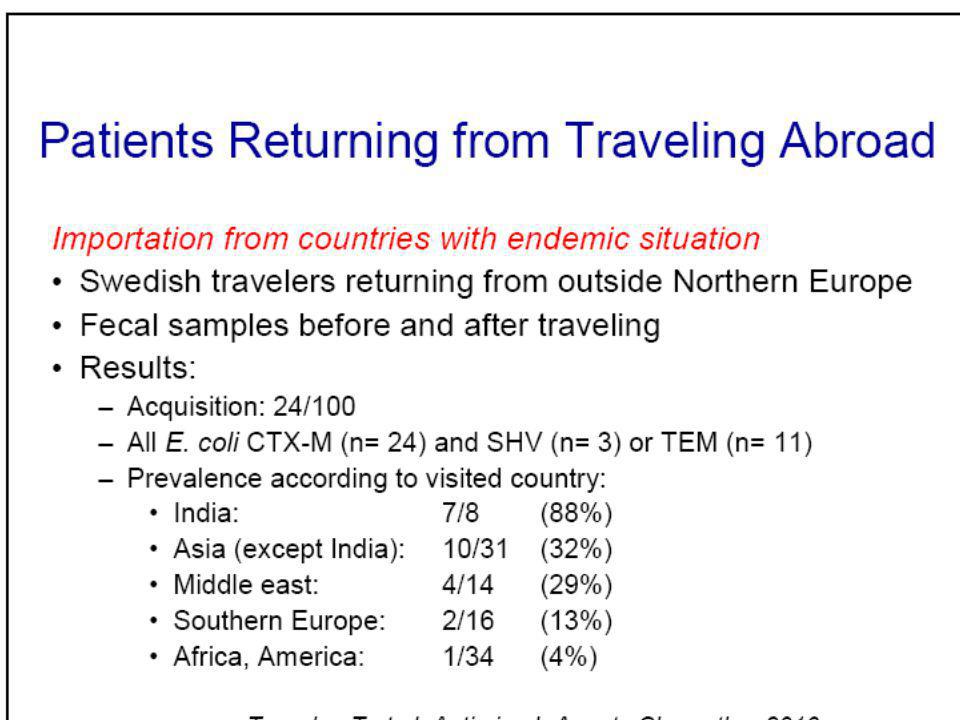
Overseas travel ? 247 infected patients with ESBL-E coli
177 community acquired , 70 health care associated 74 (73%) CTX-M Pitout, J Inf 2008
 CTX-M. Pitout, J Inf")
30
Prévalence du portage en France
?
31
En résumé Comme toute BMR Mais en plus
Facteurs liés à la charge en soin Antibiothérapie préalable Promiscuité « hospitalière » Mais en plus De vrais porteurs sans FDR habituels Promiscuité « communautaire » Environnementale?

32
Pourquoi cela nous pose un problème ?
A titre individuel Risque d’échec thérapeutique A titre collectif Risque d’amplification de la résistance

33
Be aware to co resistance

34
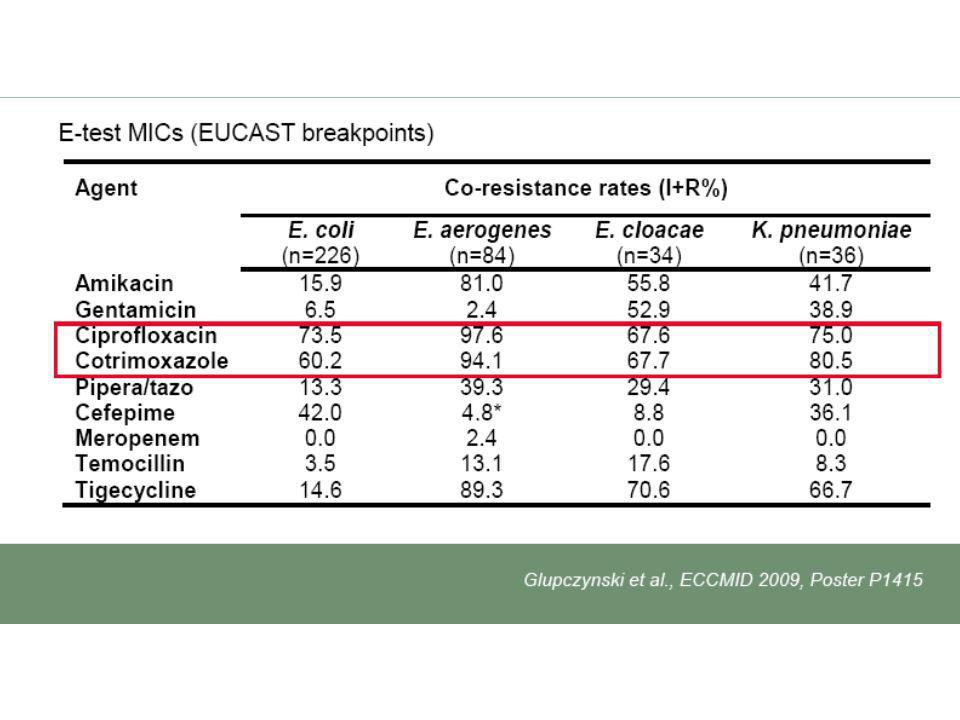
The b lactams are not the only concerned antibiotics!
Calbo, J Antimicrobial Chemother 2006, 57; 780

36
The b lactams are not the only concerned antibiotics!
MH Nicolas-Chanoine, Clin Microbiol Infect 2008

37
Do we have other antibiotics available
Do we have other antibiotics available? Are Carbapenems the only choices !!

38
Other antibiotics? Auer, AAC 2010

39
Cephamycin = Cefoxitin=Mefoxin
Little clinical expérience Can be effective Risk of selection of new resistance Impermeability !!! Different species # same risk ….. Falagas, J Hosp Inf 2009 CH Lee, JAC 2006

40
Glupczynski, Eur J Clin MIcrobiol Infect Dis 2007
Temocillin !! Glupczynski, Eur J Clin MIcrobiol Infect Dis 2007

41
Other ? Fosfomycin E coli resistant <2%
Urinary diffusion ( > 85%) Tigecycline Bacteriostatic … CMI<2 mg/l
 Tigecycline. Bacteriostatic … CMI<2 mg/l.")
42
Quelques recommandations!
Ne traiter que les infections !! Apprendre à désescalader Si l’antibiogramme le permet « Extirper » les foyers infectieux Pour obtenir une guérison plus rapide Et donc réduire les durées des traitements Utiliser les bithérapies

43
Un seul objectif LIMITER la prescription des carbapénèmes

44
CHU Necker Enfants-Malades
Consequences? Carbapenem consumption (DDD/1000 DH) CHU Necker Enfants-Malades
 CHU Necker Enfants-Malades.")
45
What are the risks? D’après J Carlet

46
How can we manage the risk?

47
Le réservoir étant difficilement identifiable
Améliorer le respect des précautions standards Eviter les acquisitions et donc les colonisations inutiles

48
Physiopathologie des infections
CLINIQUE INFECTION LATENTE COLONISATION APPARENTE COLONISATION LATENTE

49
Eviter les facteurs qui amplifient le portage!!
Chaque gramme antibiotique compte Les classes antibiotiques n’ont (probablement) pas le même poids de sélection Si vous êtes forcés, apprenez à réduire!!! Les durées comptent
 pas le même poids de sélection. Si vous êtes forcés, apprenez à réduire!!! Les durées comptent.")
50
Donskey, Antimicrobial Agents Chemotherapy 2007
CMI mg/l 1 0.25 4 Low ecological risk ? Donskey, Antimicrobial Agents Chemotherapy 2007

51
Physiopathologie des infections
CLINIQUE INFECTION LATENTE COLONISATION APPARENTE ANTIBIOTIQUE COLONISATION LATENTE

52
Eviter chez les colonisés la survenue des infections

53
Physiopathologie des infections
CLINIQUE Réduire les durées des « procédures » COLONISATION APPARENTE COLONISATION LATENTE

55
Messages Difficile de définir le réservoir
Appliquer des mesures standards Les infections communautaires Restent rares et concernent « certains » patients Apprenez a Economiser les Carbapénèmes

56
Merci de votre attention

58
Livermore JAC 2009

59
Conclusions It is difficult to define the reservoir
The most important action is : The antibiotic stewardship Carbapenems are not a homogeneous class Choose the molecules whith a favorable profile Pharmacokinetics Pharmaco Dynamics The Zero risk doesn’t exist Think about it individually Monitor your ecology

60
La résistance aux carbapénèmes, un danger immédiat ?
Enterobacteriaceae (7) La résistance aux carbapénèmes, un danger immédiat ? AmpC /BLSE + Imperméabilité Carbapénèmases de classe A Carbapénèmases de classe B Oxacillinases (classe D) Rare (pression ATB+++) Enterobacter spp., C. freundii, K. pneumoniae Chromosomiques NMC/IMI SME (<40 souches décrites) E. cloacae, S. marcescens VIM (très rares) Grèce, Corée du Sud IMP Japon, Australie OXA-23 P. mirabilis OXA-48 K. Pneumoniae (Exceptionnelles) Plasmidiques KPC (mini-épidémies Est E.-U.) K. pneumoniae+++, E. cloacae GES (GES-2,4,5,6) (très rare, description mondiale) K. pneumoniae, E. coli >98% des entérobactéries dans le Monde sensibles aux carbapénèmes
 La résistance aux carbapénèmes, un danger immédiat AmpC /BLSE + Imperméabilité. Carbapénèmases. de classe A. Carbapénèmases. de classe B. Oxacillinases. (classe D) Rare. (pression ATB+++) Enterobacter spp., C. freundii, K. pneumoniae. Chromosomiques. NMC/IMI. SME. (<40 souches décrites) E. cloacae, S. marcescens. VIM. (très rares) Grèce, Corée du Sud. IMP. Japon, Australie. OXA-23. P. mirabilis. OXA-48. K. Pneumoniae. (Exceptionnelles) Plasmidiques. KPC. (mini-épidémies Est E.-U.) K. pneumoniae+++, E. cloacae. GES (GES-2,4,5,6) (très rare, description mondiale) K. pneumoniae, E. coli. >98% des entérobactéries dans le Monde sensibles aux carbapénèmes.")
61
Source ESAC 2009

Présentations similaires










 d ’éradication du SARM en soins de longue durée>")



 Biomarqueurs IHC (n = 412) Séquençage (n = 418) 200 patients évaluables pour les facteurs pronostiques cliniques et biologiques Comparaison.>")







