Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Antibiothérapie vétérinaire et problèmes de santé publique
ECOLE NATIONALE VETERINAIRE T O U L O U S E Antibiothérapie vétérinaire et problèmes de santé publique Les facteurs de risque de l’antibiorésistance Le schéma posologique Février 2009 P.L. TOUTAIN

2
Usages des antibiotiques
Treatment & prophylaxis Veterinary medicine Human medicine Community Animal feed additives Hospital Agriculture Plant protection Environment Industry

3
"The war against infectious diseases has been won"
"One can think of the middle of the 20th century as the end of one of the most important social events in history: the virtual elimination of the infectious diseases as a significant factor in social life" Sir Mac Farland Burnett, Natural History of Infectious Disease, 1962 "The war against infectious diseases has been won" U.S. Surgeon General, 1969

4
Aujourd'hui de nombreuses maladies infectieuses qui étaient jugulées resurgissent Émergence de résistances

5
Causes de mortalité (2001)
")
6
Causes de mortalité (WHO, 2004)
Cardiovascular diseases 29.4 Infectious and parasitic diseases 19.12 Malignant neoplasms (cancers) 12.49 Respiratory diseases 6.49 Unintentional injuries 6.23 Digestive diseases 3.45 Intentional injuries (suicide, murder, war, etc.) 2.84 Neuropsychiatric disorders 1.95
 Respiratory diseases Unintentional injuries Digestive diseases Intentional injuries (suicide, murder, war, etc.) Neuropsychiatric disorders")
7
Causes de mortalité infectieuse (WHO 2004)
Code Groupe % mortalité B Infectious and parasitic diseases 19.12 B.1 Respiratory infections 6.95 B.1.1 Lower respiratory tract infections 6.81 B.1.2 Upper respiratory infections 0.13 B.2 HIV/AIDS 4.87 B.3 Diarrheal diseases 3.15 B.4 Tuberculosis 2.75 B.5 Malaria 2.23 B.6 Childhood diseases 1.97 B.6.1 Measles (rougeole) 1.07 B.6.2 Pertussis (coqueluche) 0.52 B.6.3 Tetanus 0.38 B.7 Sexually transmitted diseases 0.32 B.7.1 Syphilis 0.28 B.8 Meningitis 0.3 B.9 Tropical diseases 0.23 B.10 Hepatitis B 0.18 B.9.1 Leishmaniasis 0.09 B.9.2 Trypanosomiasis 0.08 B.11 Hepatitis C
 B.6.2. Pertussis (coqueluche) B.6.3. Tetanus B.7. Sexually transmitted diseases B.7.1. Syphilis B.8. Meningitis B.9. Tropical diseases B.10. Hepatitis B B.9.1. Leishmaniasis B.9.2. Trypanosomiasis B.11. Hepatitis C.")
8
Leading infectious killers
Measle: rougeole ARI: acute resp inf

9
Les conséquences de l'antibiorésistance
Individuelles échec du traitement Collectives perte d'activité de l'antibiotique ou d'une famille d'antibiotiques

10
Facteurs médicaux et non médicaux impliqués dans l'émergence d'antibiorésistance

11
Facteurs non médicaux impliqués dans l'émergence d'antibiorésistance
Mondialisation de l'agriculture (échanges, transports) Intensification de l'agriculture (usage vétérinaire) Usages industriels d’antibiotiques Usages phytosanitaires d’antibiotiques Surpopulation, urbanisation Fréquence et nature des contacts interindividuels Mobilité des populations Pauvreté Facteurs climatiques (température, humidité)
 Intensification de l agriculture (usage vétérinaire) Usages industriels d’antibiotiques. Usages phytosanitaires d’antibiotiques. Surpopulation, urbanisation. Fréquence et nature des contacts interindividuels. Mobilité des populations. Pauvreté. Facteurs climatiques (température, humidité)")
12
Facteurs médicaux impliqués dans l'émergence d'antibiorésistance
Accès libre aux produits de santé, automédication Les génériques ( augmentation de la consommation de vieux antibiotiques : ex: ciprofloxacine ) Techniques médicales (service d'urgence, réanimation, Schémas posologiques inadéquats Valeurs critiques des antibiogrammes à réviser Population immunodéprimée en expansion (greffés, sujets âgés, SIDA)
 Techniques médicales (service d urgence, réanimation, Schémas posologiques inadéquats. Valeurs critiques des antibiogrammes à réviser. Population immunodéprimée en expansion (greffés, sujets âgés, SIDA)")
13
In: Clinical infectious deseases 2005 41 114-117

15
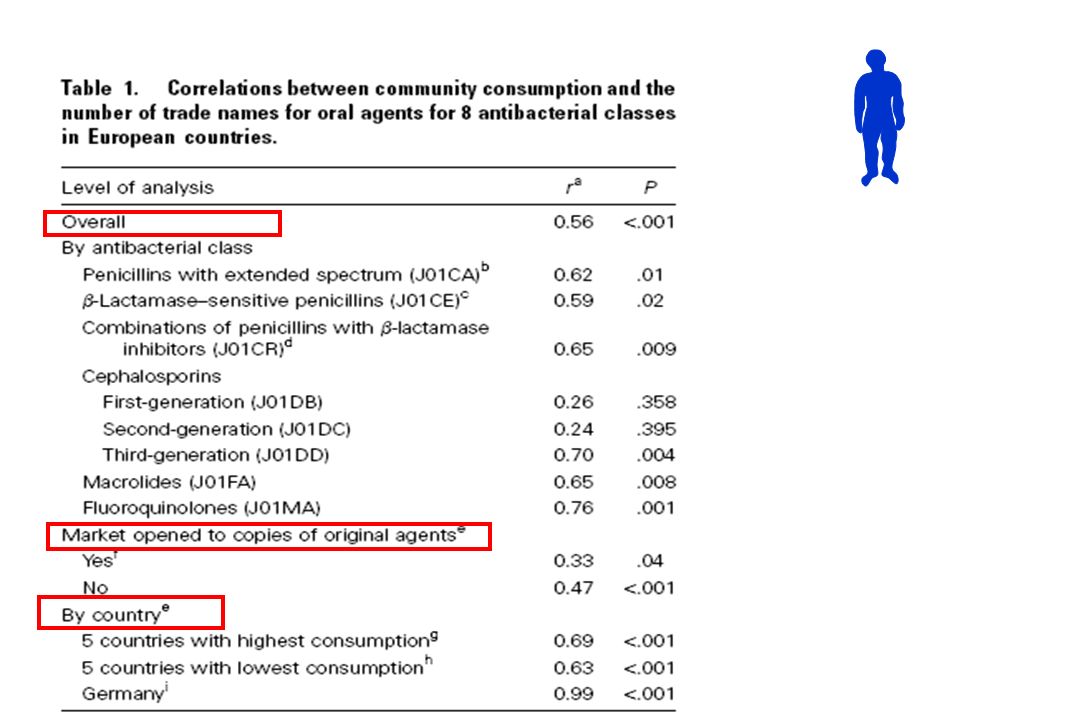
High consumption countries Low consumption countries
Correlation between community use and the number of trade names for oral-use agents for 6 antibacterial classes in EU High consumption countries Low consumption countries Nb of trade names Nb of trade names

16
Generic competition for drugs availability: Is it a good medical practice to encourage the use of old antibiotics rather new ones?

17
Is it a good practice to encourage the use of old antibiotics rather new ones?
Traditionally, from a public health perspective, doctor are encouraged not to employ newer drugs, but rather to use the older antibiotics. The recommendation whether to choose older rather than newer antibiotics was recently challenged on an epidemiological basis (Amyes et al., 2007) and shown to be flawed for quinolones, cephalosporins and carbapenems.
 and shown to be flawed for quinolones, cephalosporins and carbapenems.")
18
. For three antibiotic classes (quinolones, cephalosporins and carbapenems), it was observed that the less active drugs could be worse at hastening the spread of resistance than more active drugs in the same class. This led the authors to qualify the (WHO) stratagem of recommending the use of old antibiotics as part of microbiological folklore.
 stratagem of recommending the use of old antibiotics as part of microbiological folklore.")
19
Résistance en médecine humaine Quelle est la situation?

20
Micro-organismes pathogènes résistants majeurs en médecine humaine
Micro-organismes Origine animale ? S. Aureus Methicilline-resistant oui Mycobacterium tuberculosis Non (interdiction de traiter la tub en véto) Streptococcus pneumoniae Non Streptococcus pyogenes Non Neisseria meningitidis Non Neisseria gonorrhoea Non Campylobacter spp Possible (peu d'évidence d'échec thérap.) Salmonella spp Possible (peu d'évidence d'échec thérap.) E coli (urogen 0157) Possible (taux de résistants très faible) Vancomycin-resistant enterococci Peut-être Pseudomonas aeruginosa Non Klebsiella spp Acinetobacter spp Non Enterobacter spp Non Pneumocoque Non FEDESA
 Streptococcus pneumoniae Non. Streptococcus pyogenes Non. Neisseria meningitidis Non. Neisseria gonorrhoea Non. Campylobacter spp Possible (peu d évidence d échec thérap.) Salmonella spp Possible (peu d évidence d échec thérap.) E coli (urogen 0157) Possible (taux de résistants très faible) Vancomycin-resistant enterococci Peut-être. Pseudomonas aeruginosa Non. Klebsiella spp. Acinetobacter spp Non. Enterobacter spp Non. Pneumocoque Non. FEDESA.")
21
Bywater and Casewell JAC 2000
Evolution rapide

22
Origine des résistances en médecine humaine
La plupart des résistance en médecine humaine ne sont pas liées aux usages vétérinaires des antibiotiques On a estimé à environ « 4% » les résistances humaines d’origine animale et cela concerne en général des pathogènes peu dangereux Le cas actuel des MRSA Néanmoins, il convient de minimiser les sources animales d’antibiorésistance

23
Antibiorésistance en médecine humaine et usage vétérinaire des antibiotiques

24
Consommation mondiale d’antibiotiques pour les animaux
tonnes 99% : animaux de rente 60% 15-20% 1% 1% animaux de compagnie Barber and associates 1997

25
Consommation d'antibiotiques en Europe
L'Europe consomme 100 mg d'antibiotique par kg de viande produite

26
Production d’animaux sains pour fournir des denrées animales ou d’origine animale saines, abondante et bon marché Alimentation Santé

27
Les différents types d’usage des antibiotiques en médecine collective (porc, volaille, veau…)
Maladie Santé prophylaxie prévention Facteur de croissance Thérapeutique Métaphylaxie Animaux non malades mais présence d’un facteur de risque comme le sevrage du porcelet Présence de signes cliniques sur un % donné d’animaux Certitude de l’extension de la maladie à tout le groupe Animaux sains & usages zootechniques (interdit en UE) Animaux malades
 Animaux malades.")
28
Consommation mondiale annuelle d’antibiotiques chez l’animal (tonnes)
Oxytétracycline 5 300 Chlortétracycline 3 900 Monensine 3 500 Bacitracine 3 200 Tylosine 2 300 Salinomycine 2 100 Lasalocide 1 800 Penicilline G 900 Narasine 700 Virginiamycine 600 Il n’y a pas de comparabilité dans la nature des principes actifs utilisés en MV et MH

29
Part des utilisations vétérinaire et humaine des principaux antibiotiques
usage vétérinaire Uusage humain

30
Usages vétérinaires des antibiotiques et implications pour l’homme
Treatment & prophylaxis Veterinary medicine Human medicine Community Animal feed additives Hospital Agriculture Plant protection Environment

31
Les problèmes liés à l’usage des antibiotiques en médecine vétérinaire
Rejet d’antibiotique dans l’environnement Résidus d’antibiotique dans les aliments Diminution de la sensibilité ou résistance des pathogènes zoonotiques passant de l’animal à l’homme soit directement soit via la chaîne alimentaire Développement de résistance sur la flore commensale et passage des gènes de résistance à l’homme

32
Problème liés à l’ excrétion des antibiotiques par l’animal dans l'environnement

33
Problème de la présence des antibiotiques dans l'environnement
Certains antibiotiques sont excrétés sous leur forme active par l’animal ( fèces, urine) et persister dans les lisiers et dans l’environnement Grande stabilité de certains antibiotiques Ex:Tétracyclines : plusieurs mois dans les sols La Tiamuline reste stable dans un lisier de porc pendant plus de180 jours Le temps de demi-vie de l’érythromycine dans le lisier de porc est de 41 jours Les antibiotiques ainsi excrétés peuvent agir sur les flores environnementales (lisiers…) d’où l’analyse éco-tox réalisée lors des demandes d’AMM vétérinaires
 et persister dans les lisiers et dans l’environnement. Grande stabilité de certains antibiotiques. Ex:Tétracyclines : plusieurs mois dans les sols. La Tiamuline reste stable dans un lisier de porc pendant plus de180 jours. Le temps de demi-vie de l’érythromycine dans le lisier de porc est de 41 jours. Les antibiotiques ainsi excrétés peuvent agir sur les flores environnementales (lisiers…) d’où l’analyse éco-tox réalisée lors des demandes d’AMM vétérinaires.")
34
Résidus d’antibiotiques dans les aliments
Issus de l’animal Non respect des délais d’attente Plan de surveillance de la DGAL Contamination Glace aux antibiotiques pour les poissons

35
Les problèmes liés à l’usage des antibiotiques en médecine vétérinaire
Rejet d’antibiotique dans l’environnement Diminution de la sensibilité ou résistance des pathogènes zoonotiques passant de l’animal à l’homme soit directement soit via la chaîne alimentaire Développement de résistance sur la flore commensale et passage des gènes de résistance à l’homme

36
Quels sont les germes de l’animal susceptibles de faire de la résistance et de poser des problèmes à l’homme via l’alimentation

37
Les germes susceptibles de faire de la résistance en MV
Pathogènes animaux Zoonotiques Flore commensale Efficacité des traitements vétérinaires Efficacité homme Problème écologique global Surconsommation d'antibiotiques Eradication naturelle Risque de colonisation définitive Enjeux individuels Enjeux collectifs

38
Germes zoonotiques

39
Le cas de Staphylococcus aureus résistant à la méthicilline
Antibiorésistance : passage directe de l’animal à l’homme (risque non professionnel) Rare mais en progression immunodéprimé Le cas de Staphylococcus aureus résistant à la méthicilline
 Rare mais en progression. immunodéprimé. Le cas de Staphylococcus aureus résistant à la méthicilline.")
40
Overview of SA & MRSA in human
Staphylococcus aureus (SA) is part of normal human bacterial flora, and is found primarily in the nares SA can causes serious invasive infections including endocarditis, osteomyelitis, bacteriema, pneumonia and toxic shock syndrome.
 is part of normal human bacterial flora, and is found primarily in the nares. SA can causes serious invasive infections including endocarditis, osteomyelitis, bacteriema, pneumonia and toxic shock syndrome.")
41
MRSA (SARM) Before penicillin mortality rate from invasive Staph aureus was 90% Penicillin has a dramatic effect However resistance developed Introduction of Methicillin in 1959 to the treatment of SA resistant to penicillin MRSA identified in 1961

42
MRSA as a leading cause of nosocomial infections

43
MRSA in human: nosocomial infections
Major cause of morbidity and mortality in human Intensive Care Units (ICU) Up to 50% staphylococcal infections in human ICUs are now due to MRSA Transmission via transiently colonised hands of health care workers Hospital acquired strains commonly resistant to multiple classes of antibiotics
 Up to 50% staphylococcal infections in human ICUs are now due to MRSA. Transmission via transiently colonised hands of health care workers. Hospital acquired strains commonly resistant to multiple classes of antibiotics.")
44
S. aureus : nosocomial infections in humans
Superficial infections Wound infections Catheter infections Endocarditis Bacteraemia with sepsis Mortality of around 50%

45
MRSA: transmission Hand-to hand transmission From infected patients
From environment Floor (27% of surface in room of MRSA positive patient) Door handles Computer etc
 Door handles. Computer. etc.")
46
MRSA: treatment MRSA are sensitive to vancomycin, teicoplatin, nitrofurantoin, rifampicin, linezolid and quinopristin-dalfopristin;

47
MRSA: epidemiology

48
Overview of SA & MRSA in human epidemiological facts (US 2005)
The standardized incidence rate of invasive MRSA was 31.8 per persons year The standardized mortality rate was 6.3 per and extrapolation to a national level predicted about deaths annually associated to MRSA i.e more deaths than attributed to AIDS in that year! A meta-analysis studies found that the risk of mortality due to invasive MRSA infections was approximately twofold that seen with invasive methicillin sensitive SA

49
MRSA in animals

50
SA in animals A ubiquitous commensal with a host range that span to all vertebrates In domestic animals, SA is primarily an opportunistic pathogen associated with sporadic infections, but it is a major etiological agent of bovine mastitis An Update on Staphylococcus aureus Mastitis

51
MRSA in animals Davies P; Methicillin resistant Staphylococcus aureus: people, pigs and pets In: Am Assoc Swine Vet 2008 P15-20

52
La transmission d’homme à homme des germes zoonotiques

53
La transmission d’homme à homme des germes zoonotiques
Rare mais semble prendre de l’importance avec les MRSA Cela peut survenir chez les immunodéprimés Quand la flore bactérienne a été perturbée par un usage excessif d’antibiotique Risk assessment model (

54
MRSA: transmission between animals to man
Until recently, it was accepted that epidemiology of transmission and antimicrobial resistance of MRSA were essentially confined to the human arena, and that animals reservoir were of negligible importance Animal can act as reservoir of MRSA ( cat, dogs, horse, chicken, rabbit, pig, guinea pigs, turtle, parrot, etc.) Currently we have evidences of MRSA animal-to-human transmission (e.g from horse to human)
 Currently we have evidences of MRSA animal-to-human transmission (e.g from horse to human)")
55
MRSA in horse (Ontario Vet College 2002)
Asymptomatic nasal carriage of MRSA in 26 hospitalized horses and 16 vet personnel To read the full article

56
MRSA: An Irish survey 2005 sampling
Recovery of MRSA in animals with respiratory, urinary tract or wound infection and animal subjected to surgery following treatment in 1 vet hospital and 16 private vet clinics MRSA was recovered from 25 animals ( 14 dogs, 8 horses, 1 cat, 1 rabbit & 1 seal) and also 10 attendant vet personnel (healthy carriers)
 and also 10 attendant vet personnel (healthy carriers)")
57
sondage BVA auprès d'un échantillon de personnes et publié dans le numéro de février 2002 du mensuel Trente Millions d'amis Près de la moitié (45 %) des propriétaires de chats dorment avec leur animal.
 des propriétaires de chats dorment avec leur animal.")
58
passage directe de l’animal à l’homme (risque professionnel)
Également manipulation sans précaution des AB (porc)
")
59
A French studies has documented antimicrobial resistance of commensals in pigs and pig farmers,
In that study, 5 MRSA isolates were found in pigs, including one strain (ST 398 on multilocus sequence typing) that has since been associated with pigs in other countries. A small number of ‘pig associated’ strains were found in farmers across a wide geographic range in France, leading the authors to conclude that pig farming could be a risk factor of staphylococcal infection of farmers. To read the full article
 that has since been associated with pigs in other countries. A small number of ‘pig associated’ strains were found in farmers across a wide geographic range in France, leading the authors to conclude that pig farming could be a risk factor of staphylococcal infection of farmers. To read the full article.")
60
MRSA in swine A national Dutch survey of 540 pigs slaughtered in nine slaughterhouses, found 39% of the pigs (and 44 out of 54 groups of pigs) to be positive for MRSA in their nares. 39 All the isolates belonged to a single clonal group, MLST 398, Dutch studies estimate the prevalence of the ST398 clone in people with occupational exposure to pigs to be 760 times higher than that of the general population. investigations in other European countries (Belgium, Germany, Denmark) indicate that the occurrence of MRSA in swine is not a problem limited to the Netherlands
 to be positive for MRSA in their nares. 39 All the isolates belonged to a single clonal group, MLST 398, Dutch studies estimate the prevalence of the ST398 clone in people with occupational exposure to pigs to be 760 times higher than that of the general population. investigations in other European countries (Belgium, Germany, Denmark) indicate that the occurrence of MRSA in swine is not a problem limited to the Netherlands.")
61
MRSA: foodborne route of transmission
S aureus can frequently be isolated from pig carcasses, though generally resistant isolates have not been predominant However concerns about foodborne risk have been reinforced by the first report of a ‘life threatening’ infection with the ‘pig’ ST 398 MRSA-strain in a 63-year-old Dutch woman who was not exposed to pigs, suggesting indirect (possibly foodborne) routes of transmission.
 routes of transmission.")
62
MRSA in vets In: Clin Microbiol Infect. 2008;14 (1):29-34.
To read the full article

63
MRSA colonization is an occupational risk for veterinary professionals
MRSA was isolated from nares of 27/417 (6.5%) attendees at an international veterinary conference: 23/345 (7.0%) veterinarians, 4/34 (12.0%) technicians, and 0/38 others. To read the full article
 attendees at an. international veterinary conference: 23/345 (7.0%) veterinarians, 4/34 (12.0%) technicians, and 0/38 others. To read the full article.")
64
Resistance among coliforms isolated from fecal samples from veterinarians of different specialities
resistance Pig vet Cattle vet Poultry vet Pet vet Non pract.vet Tetracyclin Ampicillin Personal AB consumption

65
Écosystème et antibiothérapie vétérinaire : passage indirecte de l’animal à l’homme via l’alimentation

66
Bactéries zoonotiques Gène de résistance (flore commensale)
Antibiorésistance : passage indirecte de l’animal à l’homme via l’alimentation Flore digestive Oui mais gérable Bactéries zoonotiques Gène de résistance (flore commensale) Flore environnement Oui difficile à gérer
 Flore environnement. Oui difficile à gérer.")
67
Les deux dangers de santé publique liés à l’antibiorésistance
La transmission de pathogènes zoonotiques devenus résistants aux AB Salmonella Campylobacter E. coli La transmission de matériel génétique support de résistance et capable de coloniser la flore commensale digestive humaine enterococci autres enterobacteriaciae G. Morris

68
Diffusion de la résistance de l’animal à l’homme
Bactéries zoonotiques Bactéries commensales

69
Comment des bactéries rendues résistantes à cause de traitements vétérinaires ou encore des gènes de résistance d’origine vétérinaire passent-ils à l’homme?

70
Transmission à partir de l’animal des germes zoonotiques
Le traitement d'animaux porteurs de germes zoonotiques va transférer à l'homme directement ou via l'alimentation des germes zoonotiques résistants environ 100 morts aux USA imputés à cette cause

71
How people get antibiotic-resistant bacteria from chickens
1- Chicken are infected with various bacteria, including E.coli (which is lethal to chickens) and Campylobacter (which is not) 2- Flock of infected chickens is treated with fluoroquinolone antibacterial in drinking water 3- Fluoroquinolone kills E.coli 5- Chickens with fluoroquinolone-resistant Campylobacter enter human food supply 4- Resistant Campylobacter survive fluoroquinolone treatment and multiply 8- Patients fail to recover because they carry fluoroquinolone-resistance Campylobacter 6- Eating under-cooked chicken or contact with raw poultry exposes people to fluoroquinolone-resistant Campylobacter 7- People infected with fluoroquinolone- resistant Campylobacter are treated with fluoroquinolone
 and Campylobacter (which is not) 2- Flock of infected chickens is treated with fluoroquinolone antibacterial in drinking water. 3- Fluoroquinolone kills E.coli. 5- Chickens with fluoroquinolone-resistant Campylobacter enter human food supply. 4- Resistant Campylobacter survive fluoroquinolone treatment and multiply. 8- Patients fail to recover because they carry fluoroquinolone-resistance Campylobacter. 6- Eating under-cooked chicken or contact with raw poultry exposes people to fluoroquinolone-resistant Campylobacter. 7- People infected with fluoroquinolone- resistant Campylobacter are treated with fluoroquinolone.")
72
Retrait d’une AMM aux USA en 2005 pour une fluoroquinolone destinée aux volailles

73
Bactéries zoonotiques impliquées dans l'antibiorésistance
Salmonella spp 95% des cas humains (USA) soit 1.4x106 cas par an sont d'origine alimentaire Campylobacter jejuni 80% des cas humains (USA) soit 2x106 cas par an sont d'origine alimentaire
 soit 1.4x106 cas par an sont d origine alimentaire. Campylobacter jejuni. 80% des cas humains (USA) soit 2x106 cas par an sont d origine alimentaire.")
74
Prévalence des dangers microbiologiques (%) dans différentes viandes
Espèces bactériennes Porc Bovin Volaille Salmonella spp Campylobacter jejuni/coli Listeria E.coli 0157:

75
TIAC: germes identifiés

76
Causes de mortalité d’origine alimentaire
Rapport InVS/AFSSA

77
Emergence of quinolone resistance in Salmonella typhimurium DT104 in UK following licensing of fluoroquinolones for use in food animals Stöhr & Wegener, Drug resistance Updates, 2000, 3:

78
Diffusion de la résistance de l’animal à l’homme
Bactéries zoonotiques Bactéries commensales

79
Quels sont les écosystèmes de bactéries commensales posant des problèmes à l’antibiothérapie vétérinaire

80
Systèmes ouverts et large réservoir
Les écosystèmes de bactéries commensales posant des problèmes à l’antibiothérapie vétérinaire Systèmes ouverts et large réservoir Tube digestif Peau Système ouvert et faible réservoir Arbre respiratoire Système fermé et faible réservoir La mamelle

81
Le tube digestif comme réservoir de bactéries commensales
Le plus large des réservoirs Exposé aux antibiotiques administrés par voie orale et à biodisponibilité réduite comme les tétracyclines chez le porc Exposé aux antibiotiques administrés par voie générale et excrétés dans le tube digestif via la bile ou par sécrétion intestinale (fluoroquinolones) L’impact des antibiotiques sur la flore digestive est systématiquement évalué pour les nouveaux antibiotiques lors de la demande d’AMM
 L’impact des antibiotiques sur la flore digestive est systématiquement évalué pour les nouveaux antibiotiques lors de la demande d’AMM.")
82
Biophases & antibiorésistance
G.I.T Proximal Distal AB: oral route 1-F% Gut flora Zoonotic (salmonella, campylobacter commensal ( enterococcus) F% Food chain Environmental exposure Blood Man Target biophase Bug of vet interest Résistance = public health concern Résistance = lack of efficacy
 F% Food chain. Environmental exposure. Blood. Man. Target biophase. Bug of vet interest. Résistance = public health concern. Résistance = lack of efficacy.")
83
Biophases & antibiorésistance
G.I.T Proximal Distal Gut flora Zoonotic (salmonella, campylobacter commensal ( enterococcus) Intestinal secretion Bile Quinolones Macrolides Tétracyclines Food chain Environmental exposure Systemic administration Blood Man Biophase Bug of vet interest Résistance = public health concern Résistance = lack of efficacy
 Intestinal secretion. Bile. Quinolones. Macrolides. Tétracyclines. Food chain. Environmental exposure. Systemic administration. Blood. Man. Biophase. Bug of vet interest. Résistance = public health concern. Résistance = lack of efficacy.")
84
Germes commensaux et traitements antibiotiques
Hôte 1 : animal (ou homme) Mutation Antibiotique Sélection des mutants généralement non pathogènes mais pérennes (ex: coliformes) et parfois pathogènes (ex: entérocoques chez les personnes immunodéprimées) Environnement Passage à l'homme Autre homme (+++) chaîne alimentaire (+++) Hôte 2 : homme Colonisation pérenne - réserve de gènes de résistance avec possibilité de passage à des pathogènes - parfois germes deviennent pathogènes ex: enterococci résistant à vancomycine et relation avec avoparcine
 Mutation. Antibiotique. Sélection des mutants généralement non pathogènes mais pérennes (ex: coliformes) et parfois pathogènes (ex: entérocoques chez les personnes immunodéprimées) Environnement. Passage à l homme. Autre homme (+++) chaîne alimentaire (+++) Hôte 2 : homme. Colonisation pérenne. - réserve de gènes de résistance avec possibilité de passage à des pathogènes. - parfois germes deviennent pathogènes ex: enterococci résistant à vancomycine et relation avec avoparcine.")
85
Les flores commensales chez l’homme
Les bactéries commensales (à la différence des pathogènes zoonotiques) sont des bactéries résidentes et elles perdurent dans leur écosystème Les échanges interhumains sont fréquents (ce qui n’est pas le cas pour les zoonotiques) Les charges bactériennes sont élevées et associées avec un état de bonne santé Ici le risque est associé à la prévalence de l’antibiorésistance dans les flores humaines
 sont des bactéries résidentes et elles perdurent dans leur écosystème. Les échanges interhumains sont fréquents (ce qui n’est pas le cas pour les zoonotiques) Les charges bactériennes sont élevées et associées avec un état de bonne santé. Ici le risque est associé à la prévalence de l’antibiorésistance dans les flores humaines.")
86
Enteroccocus spp: chevaux de Troie pour l’antibiorésistance
Sont un réservoir de gènes de résistance aux AB Acquisition aisée de gène de résistance et de leur trasfert à d’autres espèces (Staphylococcus aureus, listeria monocytogene, bacillus spp).
.")
87
Commensal bacteria A low level of resistance in the intestinal flora of food animals should be considered as a safety and quality mark for these animals Van den Bogard, 1997

88
Les différentes bactéries surveillées
Bactéries zoonotiques Salmonella spp, Isolées dans différents écosystèmes (environnement, animaux, alimentation…) campylobacter coli and jejuni Isolés à l’abattoir pour les filières aviaire, porcine et bovine Bactéries sentinelles (Indicator bacteria) E.coli, Enterococcus faecium and faecalis Pathogènes propres aux animaux Isolés d’animaux malades (bovins, porcins, volailles)
 campylobacter coli and jejuni. Isolés à l’abattoir pour les filières aviaire, porcine et bovine. Bactéries sentinelles (Indicator bacteria) E.coli, Enterococcus faecium and faecalis. Pathogènes propres aux animaux. Isolés d’animaux malades (bovins, porcins, volailles)")
89
Réseau salmonella Réseau de 150 labo piloté par l’AFSSA
4 secteurs : environnement, animaux, alimentation humaine et animale Plus de 3000 antibiogrammes/an Antibiogramme centralisé

90
Les bactéries commensales indicatrices
L’évaluation du niveau de sensibilité aux antibiotiques dans la flore fécale permet d’apprécier la pression de sélection des AB E. coli & enterococci (Enterococcus faecium) Utilisé comme bactérie indicatrice des Gram positif Enterococcus faecalis) Utilisé comme bactérie indicatrices des Gram moins
 Utilisé comme bactérie indicatrice des Gram positif. Enterococcus faecalis) Utilisé comme bactérie indicatrices des Gram moins.")
91
Résultats de la surveillance
Farm Rapport du programme français de surveillance de l’antibiorésistance des bactéries d’origine anilale (Afssa Août 2006) Pour connaître les résultats cliquer sur: programme français de surveillance
 Pour connaître les résultats cliquer sur: programme français de surveillance.")
92
L'interdiction de l'avoparcine : un exemple de gestion des risques au niveau communautaire

93
La problématique L'avoparcine (additif alimentaire utilisé chez le porc et le poulet en tant qu'additif depuis 1976) et la vancomycine appartiennent à la même famille des glycopeptides La vancomycine est utilisée en médecine humaine contre les entérocoques et les staphylocoques résistants à la methicilline (antibiotique dit de dernier "recours")
 et la vancomycine appartiennent à la même famille des glycopeptides. La vancomycine est utilisée en médecine humaine contre les entérocoques et les staphylocoques résistants à la methicilline (antibiotique dit de dernier recours )")
94
Découverte de la résistance à la vancomycine
1986 : découverte des premières souches d'origine humaine d‘Enterococcus faecium résistantes aux glycopeptides (ERG) Le transfert de résistance aux entérocoques est obtenu in vitro et in vivo chez l'animal Étude danoise : association entre la prévalence de la résistance à la vancomycine dans des isolats de porcs et de volaille et l'usage de l'avoparcine (rien chez les bovins) avec des prévalences de : 15% : technique d'enrichissement 2% : technique classique
 Le transfert de résistance aux entérocoques est obtenu in vitro et in vivo chez l animal. Étude danoise : association entre la prévalence de la résistance à la vancomycine dans des isolats de porcs et de volaille et l usage de l avoparcine (rien chez les bovins) avec des prévalences de : 15% : technique d enrichissement. 2% : technique classique.")
95
Question sociétale posée:
Avoparcine et vancomycine appartenant à la même famille, la supplémentation en avoparcine de l'alimentation animale contribue-t-elle à la présence de souches ERG chez l'homme ? La réponse n’a pas été univoque mais les additifs ont été interdits au nom du principe de précaution (gestion du danger et non du risque)
")
96
Trend in antibacterial usage and resistance in Enterococcus faecium in Denmark : Avoparcin
80 30 000 60 20 000 % resistant isolates 40 Kg active compound used 10 000 20 94 95 96 97 98 99 Swine broilers Avoparcin Stöhr & Wegener, Drug resistance Updates, 2000, 3:

97
Les facteurs et pratiques à risque en médecine humaine

98
Facteurs de risques en médecine humaine: Surconsommation d’antibiotiques

99
Antimicrob Chemother 2006;doi: 10.1093/jac/dkl188
European Surveillance of Antimicrobial Consumption Outpatient antibiotic use in Europe Ferech M, Coenen S, Malhotra-Kumar S, Dvorakova K, Hendrickx E, Suetens C, on behalf of the ESAC Project Group. Antimicrob Chemother 2006;doi: /jac/dkl188

100
Outpatient antibiotic in 25 European countries in 2003*
* For Iceland total data are use; for Poland 2002 data are used.

101
Outpatient use of cephalosporins in 27 European countries in 2004*
dark green = lowest to DID; light green = to DID; yellow = to DID; red = DID to highest; grey = ESAC participant for which no data are available. * expressed in DDD per thousand inhabitants per day (DID); for Iceland total data are used, for Poland 2002, and for Estonia and Italy 2003 data;
; for Iceland total data are used, for Poland 2002, and for Estonia and Italy 2003 data;")
102
Outpatient Antibiotic Use in Europe and Association with Resistance.
The LANCET Volume 365, Number February 2005 Outpatient Antibiotic Use in Europe and Association with Resistance. Herman Goossens, M.D., Ph.D., Matus Ferech, Pharm.D., Robert Vander Stichele, M.D., , Monique Elseviers, Ph.D, and the ESAC Project Group. From the ESAC Management Team, Department of Microbiology, University of Antwerp, Universiteitsplein 1, B-2610 Antwerp, Belgium

103
Usage de l'érythromycine et conséquence sur le pourcentage de résistance sur les streptocoques de type A Resistance to erythromycin (%) Erythromycin consumption (doses/1000/day)
 Erythromycin consumption (doses/1000/day)")
104
Facteurs de risques en médecine humaine: mouvements de population et résistance à Streptococcus pyogenes en suède Tetracycline resistance (%) Kronoberg county, Sweden 1989 (>400 strains / year) 50 40 Two consecutive contingents of refugees (sept 92-oct93) 30 20 10 89 90 91 92 93 94 95 96 97 98 99 Year G. Kahimeter
 Kronoberg county, Sweden (>400 strains / year) Two consecutive contingents of refugees (sept 92-oct93) Year. G. Kahimeter.")
105
Usure des antibiotiques et le non renouvellement des antibiotiques

106
Introductions of new antibiotic classes
TMP 1970 Oxazolidinones 2000 Quinolones 1962 Streptogramins 1962 Glycopeptides 1958 Macrolides 1952 Aminoglycosides 1950 Chloramphenicol 1949 Tetracyclines 1949 Penicillins 1940 Sulfas 1936

107
Economie du développement d'un antibiotique
Coût : 400 à Euros Rentabilité ? Si très efficace, sera réservé aux hôpitaux

108
Facteurs de risques en médecine humaine
Areas associated with inadequate antimicrobial resistance intensive care units oncology bone marrow transplantation wards dialysis Kollef, Clin.Inf. Dis., 2000,4:131

109
Facteurs de risques en médecine humaine
Previous use of antibiotic is an important risk factor for nosocomial infections Prolonged stay in hospital patients become colonized by resistant bacteria Presence of invasive device endotracheal tubes, IV catheters, urinary catheters

110
Facteurs de risques en médecine humaine: les schémas posologiques

111
Dosage regimen and prevention of resistance
the most important risk factor is repeated exposure to suboptimal antibiotic concentrations dosage regimen should minimize the likelihood of exposing pathogens to sublethal drug levels

112
Effect on Penicillin resistance in pneumococcus isolates (n=465) of duration of b-lactam use, 6 months before swab collection Nb of days of b-lactam use 1-7 8-14 >14 Odd ratios 0.86 1.5 2.5 95% CI Nasrin et al. BMJ, 2002

113
Schéma posologique et antibiorésistance
Odds ratio confidence interval Oral blactams in past 30 days Dose lower than clinically recommended Treatment >5 days 16 children carrying penicillin-resistant pneumococcal

114
Dosage regimen and antibioresistance
To design appropriate dosage regimen may be the single most important contribution of clinical pharmacology to the resistance problem over the next years which we are certain to be without significant advance for new antibiotics

115
Comment les antibiotiques favorisent-ils l’antibiorésistance

116
Resistance: mécanismes
Emergence spontanée Selection Transfer between patient Transfer from one country to another one Antibiotique

117
Schéma posologiques et prévention des résistances: le cas des quinolones

118
Traditional explanation for enrichment of mutants
Concentration MIC Placing MIC near the lower boundary of the selection window contradicts traditional medical teaching in which resistant mutants are thought to be selected primarily when drug concentrations are below MIC (shown in a figure taken from a book published in 2002 (2)). This distinction is important because traditional dosing recommendations to exceed MIC are likely to place drug concentrations inside the selection window where they will enrich resistant mutant subpopulations. While low drug concentrations do not enrich resistant mutants, they do allow pathogen population expansion; consequently, low drug doses indirectly foster the generation of new mutants that will be enriched by subsequent antimicrobial challenge. Selective Pressure Time plt
). This distinction is important because traditional dosing recommendations to exceed MIC are likely to place drug concentrations inside the selection window where they will enrich resistant mutant subpopulations. While low drug concentrations do not enrich resistant mutants, they do allow pathogen population expansion; consequently, low drug doses indirectly foster the generation of new mutants that will be enriched by subsequent antimicrobial challenge. Selective Pressure. Time. plt.")
119
Notion de concentration préventive de mutants (CMP) : le cas des quinolones
 : le cas des quinolones")
120
Without antibiotics With antibiotics
Blocking Growth of Single Mutants Forces Cells to Have a Double Mutation to Overcome Drug Without antibiotics 10-4 single mutant population 10-8 Wild pop With antibiotics 10-8 single mutant population Wild population éradication plt sensible single mutant Double mutant

121
Quinolone resistance: Spontaneous mutations
Chromosomal mutation affecting drug permeation (alteration of efflux pump) Probability: 10-5 Point mutation: (gyrase, totpoisomerase) Probability: 10-8
 Probability: Point mutation: (gyrase, totpoisomerase) Probability:")
122
Fréquence de mutation et CMI pour la ciprofloxacine
5*MIC 10*MIC P. aeruginosa S. aureus

123
The selection window hypothesis
Mutant prevention concentration (MPC) (to inhibit growth of the least susceptible, single step mutant) MIC Selective concentration (SC) to block wild-type bacteria Mutant Selection window Plasma concentrations All bacteria inhibited Growth of only the most resistant subpopulation Growth of all bacteria plt
 (to inhibit growth of the least susceptible, single step mutant) MIC. Selective concentration (SC) to block wild-type bacteria. Mutant Selection window. Plasma concentrations. All bacteria inhibited. Growth of only the most resistant subpopulation. Growth of all bacteria. plt.")
124
Mutants are not selected at concentrations below MIC or above the MPC
For emphasis we restate that as a rule mutants are not selectively enriched at drug concentrations below MIC. As an aside, we note some selective pressure exists at concentrations below the standard MIC because it measures inhibition of growth of a large number of cells (100,000). Indeed, some enrichment of mutants does occur upon repeated serial passage of a strain (6). These data stress that the bottom boundary of the window can be fuzzy. That is why we define it to be MIC(99), the minimal concentration that blocks growth of 99% of the cells in a culture. MIC(50) would be a more precise lower boundary, but it is more difficult to determine experimentally. plt
. Indeed, some enrichment of mutants does occur upon repeated serial passage of a strain (6). These data stress that the bottom boundary of the window can be fuzzy. That is why we define it to be MIC(99), the minimal concentration that blocks growth of 99% of the cells in a culture. MIC(50) would be a more precise lower boundary, but it is more difficult to determine experimentally. plt.")
125
Emergence of mutational resistance
Resistance is a function of the product of original inoculum, rate of reproduction and the mutation rate, divided by the negative growth rate (reduction in susceptibles) If high inoculum size resistance If no starting mutants, best S killer resistance If starting R mutants, best S killer resistance Lipsitite and Levin ARC 1997
 If high inoculum size resistance. If no starting mutants, best S killer resistance. If starting R mutants, best S killer resistance. Lipsitite and Levin ARC")
126
Strategies for Restricting the Development of Resistance
plt

127
Strategies for Restricting the Development of Resistance
Three possible strategies for restricting the development of antimicrobial resistance. To keep concentrations above the MPC To narrow the selection window. To use combination therapy in which pharmacokinetic mismatch is avoided. plt

128
Aminoglycosides: achieve a peak of 8x the MIC at least
What is the concentration needed to prevent mutation and/or selection of bacteria with reduced susceptibility? Beta-lactams: we do not know but most likely stay always above the MIC… Aminoglycosides: achieve a peak of 8x the MIC at least Fluoroquinolones: AUC/MIC > 100 h and peak/MIC > 8

129
The role of antibiotics is to eradicate the causative organisms from the site of infection
Jacobs. Istambul, 2001

130
EMEA "Points to consider" July 2000
Inadequate dosing of antibiotics is probably an important reason for misuse and subsequent risk of resistance A recommendation on proper dosing regimens for different infections would be an important part of comprehensive strategy The possibility to produce such a dose recommendation based on pharmacokinetic and pharmacodynamic considerations will be further investigated in one of the CPMP working parties...

131
Comment déterminer un schéma posologique pour un antibiotique
Essais cliniques Dose titration PK/PD

132
Clinical trials

133
Spontaneous cure vs. antibiotic treatment
100 Spontaneous clinical cure Cure with antibiotic treatment 50 % patients D1 D2 Time

134
Clinical trials Poor diagnostic tools Poor endpoint in clinical trials
Poor knowledge about which patients really benefit from antibiotic treatment

135
Les essais cliniques Clinical trials of efficacy are presently almost entirely funded by the pharmaceutical industry and have objectives confined to satisfying regulatory authorities thus, trials which seek to optimize the dose, dose interval and duration of treatment are rarely done Opinion of the Scientific Steering Committee on Antimicrobial Resistance, 28 may 1999

136
Bacteriological vs. clinical success: the Pollyanna phenomenon

137
The Pollyanna phenomenon
The clinical efficacy does not always indicate bacteriological efficacy making it difficult to distinguish between antimicrobials on clinical outcomes only or why are statistical differences between 2 antibiotics in clinical outcome rarely seen.

138
L'effet Pollyanna Otite moyenne
Discordance des résultats bactériologiques et cliniques Otite moyenne Efficacité (%)
")
139
The Pollyanna phenomenon
Merchant et al. J. Pediatrics, 1992, Otitis media bacteriological cure high (100%) clinical success = 89% other cases = non bacterial aetiology Bacteriological cure low (27%) clinical success = 74% Conclusion : discrimination between "good" and "bad" antimicrobial on clinical outcomes alone would require extremely large clinical trials
 clinical success = 89% other cases = non bacterial aetiology. Bacteriological cure low (27%) clinical success = 74% Conclusion : discrimination between good and bad antimicrobial on clinical outcomes alone would require extremely large clinical trials.")
140
The Pollyanna phenomenon
If efficacy is measured by symptomatic response, drugs with excellent antibacterial activity will appear less efficacious than they really are and drugs with poor antibacterial activity will appear more efficacious than they really are.

141
Essais cliniques Ne sont pas des outils appropriés pour définir un schéma posologique Doivent vérifier (valider) que le schéma posologique sélectionné par d'autres approches est efficace (essai de confirmation)
 que le schéma posologique sélectionné par d autres approches est efficace (essai de confirmation)")
142
Les indicateurs PK/PD d'efficacité
Inaptitude des critères cliniques à trouver les bons schémas posologiques PK/PD

143
Les indicateurs PK/PD d'efficacité
Principe contrôle l'exposition à l'antibiotique car la "forme" de l'exposition contrôle l’effet (in vitro) et l'efficacité (in vivo)
 et l efficacité (in vivo)")
144
La vitesse de bactericidie

145
La bactéricidie • Evalue la décroissance de l'inoculum bactérien en fonction du temps et des concentrations en antibiotique Log C.F.U. / ml latence phase de bactéricidie phase de recroissance 2 6 temps (h)
")
146
Concentration dépendant
La bactéricidie Concentration dépendant Temps dépendant Bactéries survivantes Bactéries survivantes 6 h 6 h Temps Temps Pente dose- dépendante Pente indépendante de la dose

147
Propriétés des antibiotiques " Dose et temps dépendants "
" Dose dépendants " - Effet bactéricide rapide - Effet fonction de la dose, effet "pic" - Peu d'importance des concentrations minimales - Peu d'importance de la durée d'exposition - Effet post-antibiotique dose dépendant " Temps dépendants " - Effet bactéricide lent - Effet indépendant de la dose et de Cmax - Importance des concentrations minimales

148
La bactéricidie La reconnaissance de deux grands types d'antibiotiques a conduit à explorer des indicateurs in vivo de l'efficacité des antibiotiques prenant en compte la concentration et le temps.

149
D'où viennent les indices PK/PD
Modèles animaux validations cliniques (analyses rétrospectives)
")
150
In vivo model Murine thigh infection (neutropenic) Pneumoniae in rat
 Pneumoniae in rat")
151
Correlation of pharmacodynamic parameters with efficacy
Use neutropenic murine thigh-and lung-infection models Evaluate different dosing regimens (5 different total doses given at 4-6 different dosing intervals) Measure efficacy from change in Log10 CFU per thigh or lung at the end of 24 h of therapy Correlate efficacy with various pharmacodynamic parameters (time above MIC, peak/MIC, 24h AUC/MIC)
 Measure efficacy from change in Log10 CFU per thigh or lung at the end of 24 h of therapy. Correlate efficacy with various pharmacodynamic parameters (time above MIC, peak/MIC, 24h AUC/MIC)")
152
Relationship between PK/PD parameters and efficacy for cefotaxime against Klebsiella pneumoniae in a pneumonia model 10 10 10 R² = 94% 9 9 9 8 8 8 Log10 CFU per lung at 24 h 7 7 7 6 6 6 5 5 5 01 1 10 100 1000 10000 3 10 30 100 300 1000 3000 20 40 60 80 100 24 h AUC/MIC ratio Peak MIC ratio Time above MIC (%) Craig CID, 1998
 Craig CID,")
153
Relationship between 24h AUC/MIC and mortality for Fluoroquinolones against gram negative bacilli in immunocompromised animal models 100 80 60 % Mortality 40 20 3 10 30 100 300 1000 24 h AUC/MIC

154
Relationship Between T>MIC and Efficacy for Carbapenems (Red), Penicillins (Aqua) and Cephalosporins (Yellow) plt

155
PK/PD indices as indicator of antibiotic efficacy

156
Quantitative indices of antimicrobial PK/PD
Should be mixed (hybrid) indices considering microbiological (MIC) and PK criteria together Able to predict outcome of therapy Able to allow dual individualization (PK and PD) of the dosage regimen
 indices considering microbiological (MIC) and PK criteria together. Able to predict outcome of therapy. Able to allow dual individualization (PK and PD) of the dosage regimen.")
157
Les critères PK/PD AUIC (ou AUC/CMI) : quinolones, tétracyclines
Cmax/CMI : aminoglycosides T>CMI : pénicillines, cephalosporines, macrolides Cmax Concentrations CMI Temps 24h T>CMI

158
AUIC : definition AUC (t1-t2) AUIC = AUC(t1-t2) / MIC Unit = time (h)
Established on a 24 h period (in steady state conditions) Concentrations MIC t1 t2 24 Time (h) Time considered for computing
 Concentrations. MIC. t1. t Time (h) Time considered for computing.")
159
Pourquoi ces indices sont-ils dits PK et PD
AUC CMI Dose / Clearance CMI50(90) AUIC # = PD adaptation posologique mixte PK et PD (dual)
 AUIC # = PD. adaptation posologique mixte PK et PD (dual)")
160
Cmax / MIC The inhibitory ratio
PK at steady state Bioavailability (%) clearance rate constant of absorption rate constant of elimination (clearance , VD) accumulation factor for multiple dosing (half-life) Cmax MIC90 IR = good predictor of clinical outcome for concentration dependent antibiotic a high Cmax/MIC avoids resistance the "best" index for aminoglycoside PD
 clearance. rate constant of absorption. rate constant of elimination (clearance , VD) accumulation factor for multiple dosing (half-life) Cmax. MIC90. IR = good predictor of clinical outcome for concentration dependent antibiotic. a high Cmax/MIC avoids resistance. the best index for aminoglycoside. PD.")
161
T > MIC Time for which drug concentration exceeds MIC
T>MIC between t2 - t1 PK determinant : complex clearance, half-life Usually given as a percentage of the dosage interval at steady state Application: Betalactam Half-life concentrations MIC Time (h) 24 t1 t2
 24. t1. t2.")
162
The validation of efficacy index clinical data

163
Validation of efficacy index : which is the optimum one in terms of accuracy, reproducibility, clinical relevance in silico simulation in vitro dynamic model animal model clinical trial

164
PK/PD and clinical trials
Retrospective analysis clinical PK/PD Prospective validation PK/PD clinical trials

165
Efficacy index: clinical validation
Bacteriological cure versus time above MIC in otitis media (from Craig and Andes 1996) 100 S. pneumoniae Penicillin cephalosporins 50 Bacteriologic cure (%) H. influenzae Penicillin cephalosporins 50 100 Time above MIC (%) Free serum concentration need to exceed the MIC of the pathogen for 40-50% of the dosing interval to obtain bacteriological cure in 80% of patients
 100. S. pneumoniae. Penicillin. cephalosporins. 50. Bacteriologic cure (%) H. influenzae. Penicillin. cephalosporins Time above MIC (%) Free serum concentration need to exceed the MIC of the pathogen for 40-50% of the dosing interval to obtain bacteriological cure in 80% of patients.")
166
Efficacy index: clinical validation
Relationship between the maximal peak plasma level to MIC ratio and the rate of clinical response in 236 patients with Gram-negative bacterial infections treated with aminoglycosides (gentamicin, tobramycin, amikacin) 100 80 Response rate (%) 60 2 4 6 8 10 12 Maximum peak/MIC ratio Moor et al J. Infect. Dis.
 Response rate (%) Maximum peak/MIC ratio. Moor et al J. Infect. Dis.")
167
AUIC and bacterial eradication
Nosocomial pneumonia treated with IV ciprofloxacin AUIC was highly predictive of time to bacterial eradication If AUIC >250 h/day : eradication of organism on day 1 of therapy good target for nosocomial pneumonia and compromised host defense 100 AUIC < 125 % patients remaining culture positive 50 AUIC AUIC > 250 4 8 12 Days after start of therapy Schentag Symposium, 1999

168
AUIC and bacterial resistance
Ciprofloxacin AUIC predicts bacterial resistance in nosocomial pneumoniae 100 Resistance for AUIC < 100 day % 4 50 20 93 simulation AUC/MIC > 101 75 50 Probability of remaining susceptible AUC/MIC< 100 25 5 10 15 20 No.Days after start of therapy AUIC < 100 = suboptimal Schentag-Symposium 1999

169
PK/PD vs. dose-titration trial
PK/PD Dose titration Subjects healthy infectious model volunteers patient Endpoints surrogate clinical or correlated bacteriological to clinical cure cure

170
Valeurs à atteindre pour les indices PK/PD
AUIC : 125 h (5 x CMI) Cmax / CMI : 10-12 T>CMI : 50 à 100%
 Cmax / CMI : T>CMI : 50 à 100%")
171
Calcul de la dose (PK/PD)
Approche populationnelle PK/PD Dose = x x Clairance (24h) Objectif thérapeutique PD (mesuré) Pop PK AUIC 24h CMI fu x F% Fraction libre biodisponibilité
 Objectif thérapeutique. PD (mesuré) Pop. PK. AUIC. 24h. CMI. fu x F% Fraction libre. biodisponibilité.")
172
Les indices PK/PD sont basés sur des concentrations plasmatiques libres et non tissulaires pourquoi?

173
Where are located the bacteria
ECF Most bacteria of clinical interest - respiratory infection - wound infection - digestive tract inf. Cell (in phagocytic cell most often) Legionnella spp mycoplasma (some) chlamydiae Brucella Cryptosporidiosis Listeria monocytogene Salmonella Mycobacteria Meningococci
 Legionnella spp. mycoplasma (some) chlamydiae. Brucella. Cryptosporidiosis. Listeria monocytogene. Salmonella. Mycobacteria. Meningococci.")
174
(S. aureus, Brucella, Salmonella)
Barrier, efflux pump Porous capillaries Plasma Interstitial fluid Brain, retina, prostate Surrogate marker (T>MIC, AUIC, Cmax/MIC) Biophase for most bacteria of veterinary therapeutical interest Tissular barrier B Mannhemia, Pasteurella Haemophilus, Streptococcus, Staphylococcus, Coli, Klebsiella Bound F Bound F B lipophilicity F Efflux pump Total concentration Biophase for facultative and obligatory intracellular pathogens Bound Cytosol (Listeria, Shigella) B F Phagosome (Chlamydiae) Cell membrane Cell Bound B F B B Obligatory or facultative bacteria Phagolysosome (S. aureus, Brucella, Salmonella) plt
 Biophase for most bacteria of veterinary therapeutical interest. Tissular barrier. B. Mannhemia, Pasteurella Haemophilus, Streptococcus, Staphylococcus, Coli, Klebsiella. Bound. F. Bound. F. B. lipophilicity. F. Efflux pump. Total concentration. Biophase for facultative and obligatory intracellular pathogens. Bound. Cytosol. (Listeria, Shigella) B. F. Phagosome. (Chlamydiae) Cell membrane. Cell. Bound. B. F. B. B. Obligatory or facultative bacteria. Phagolysosome. (S. aureus, Brucella, Salmonella) plt.")
175
Le site d'infection Germes extracellulaires
La plupart des germes pathogènes sont des parasites extracellulaires Ils se multiplient en dehors des cellules c'est à dire dans les espaces intercellulaires (substances fondamentales) en contact avec l'eau extracellulaire Ces germes peuvent être phagocytés par les PNN et détruits la phagocytose est la clé de la guérison elle est inhibée par les facteurs de virulence
 en contact avec l eau extracellulaire. Ces germes peuvent être phagocytés par les PNN et détruits. la phagocytose est la clé de la guérison. elle est inhibée par les facteurs de virulence.")
176
Le site d'infection (2) Les trois types de bactéries
Intracellulaires obligées Chlamydiae Rickettsia Brucella Lawsonia intracellularis (enterite proliferative du porc) Rhodococcus equi Extracellulaires S. pneumoniae E. coli Klebsiella Mannhemia pasteurella Actinobacillius pleuropneumoniae Mycoplasma hyopneumoniae Bordetala bronchoseptia Intracellulaires facultatives S. aureus S. typhi Listeria Mycobacterium tubercolosis Streptococcus suis
 Rhodococcus equi. Extracellulaires. S. pneumoniae. E. coli. Klebsiella. Mannhemia pasteurella. Actinobacillius pleuropneumoniae. Mycoplasma hyopneumoniae. Bordetala bronchoseptia. Intracellulaires facultatives. S. aureus. S. typhi. Listeria. Mycobacterium tubercolosis. Streptococcus suis.")
177
Intracellular location of bacteria
Fusion B Lysosome 3 pH=7.4 Phagosome Phagolysosome B 4 B 1 B S.aureaus Brucella Salmonella Coxiella burneti pH=5.0 B B B 2 Chlamydiae B No fusion with lysosome Listeria

178
Tissue concentrations
According to EMEA "unreliable information is generated from assays of drug concentrations in whole tissues (e.g. homogenates)" EMEA 2000
 EMEA")
179
En France : la qualité est privilégiée
En général, quel type de poulet achetez-vous ? Les 61 ans et plus, cadres, ménages à haut revenu et les couples privilégient le Label Rouge Dans 75% des cas, les français achètent le poulet en grande surface Source : TRUST

180
Habitudes d’achats : le poulet surgelé est très peu diffusé en France contrairement à l’Allemagne
Achetez-vous du poulet frais, … du poulet surgelé ? Source : TRUST

181
Des risques réels qui n’augmentent pas accompagnés de nombreux évènements médiatisés …
Les crises alimentaires Fièvre aphteuse 2001 Crise du poulet 1999 Présence de verre dans les bouteilles de Coca-Cola Vache folle 1996 Listériose (brie de Meaux) 1995 Salmonelle dans du jambon Marks & Spencer 1994 Présence de verre dans les bières Bavaria/Heineken 1993 Épidémie de listériose (langue de porc en gelée, rillettes, fromage et charcuterie à la coupe) Benzène dans l’eau Perrier 1990 Éclats de verre dans les petits pots pour bébés 1989 Veau aux hormones 1988 Listéria dans le vacherin suisse 1987 Colorants et additifs 1980 Huiles de colza 1978 Évènements Dates Des risques réels qui n’augmentent pas Une mortalité liée à l’alimentation qui a fortement diminuée depuis le début du XXème siècle ( à / 100 par an de nos jours) Un taux de mortalité qui est stable depuis 1980
 Salmonelle dans du jambon Marks & Spencer Présence de verre dans les bières Bavaria/Heineken Épidémie de listériose (langue de porc en gelée, rillettes, fromage et charcuterie à la coupe) Benzène dans l’eau Perrier Éclats de verre dans les petits pots pour bébés Veau aux hormones Listéria dans le vacherin suisse Colorants et additifs Huiles de colza Évènements. Dates. Des risques réels qui n’augmentent pas. Une mortalité liée à l’alimentation qui a fortement diminuée depuis le début du XXème siècle ( à / 100 par an de nos jours) Un taux de mortalité qui est stable depuis")
182
… conduisant à de fortes retombées sur la consommation
Évolution des dépenses en viandes de volailles en millions de francs courants 1999 Crise de la dioxine Viande de volaille Viande de bœuf 1996 Crise de la vache folle Source : CREDOC à partir de l’INSEE

183
Pour les français, le premier critère d ’achat reste le goût
Pour vos achats alimentaires, quelle importance accordez-vous aux critères suivants ? (Items 7 et 6) % Source : TRUST
 % Source : TRUST.")
184
Les OGM et les plats préparés : deux produits les plus risqués
Que pensez-vous du risque pour la santé des aliments suivants ? (France) Source : TRUST
 Source : TRUST.")
Présentations similaires




![[number 1-100] There is no rule to the way to remember the names for the numbers 1 to 10 in French so we recommend that you simply practice!](/1/172873/big_thumb.jpg "[number 1-100] There is no rule to the way to remember the names for the numbers 1 to 10 in French so we recommend that you simply practice!>")














