Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
DESC REANIMATION MEDICALE
Affections aortiques aigue traumatiques Sanfiorenzo céline CHU NICE

2
TRAUMATISME THORACIQUE FERME
Polytraumatisme

3
Accident de la voie publique 70%
Traumatisme thoracique Polytraumatisme 70-80% RTA isolée 5%1 Contexte Violent Homme jeune, OH Défaillance respiratoire/hémodynamique RTA 70-90%DCi 2 30% 6h, 50% 24h 90% 4 mois

4
Contusions cardiaques 3
Surtout Oreillette et Ventricule droit. Arythmie - trouble de la conduction. IDM sur dissection coronaire, thrombose ou rupture de plaque. Hémopéricarde pneumopéricarde tamponnade. Valvulopathie aortique traumatique.

5
Contusions cardiaques
Lésions associées Contusions cardiaques 76%3 Contusion pulmonaire Pneumothorax Hémothorax 53%4 Fractures côtes Sternum 69%4 Fractures autres 43%4 Trauma crânien 68%4 Contusion hépatique 65%4

7
DISSECTION AORTIQUE TRAUMATIQUE

8
Etiologies Accidents de la voie publique à grande vitesse chocs frontaux, latéraux. Accidents d’avion. Chutes/défenestration.

9
4 théories mécanistiques
Décélération brutale avec torsion/compression : force de cisaillement5. F cisaillement + F compressive (APG-BSG)5. P intraluminale brutale «Water Hammer Effect»5. Pincement osseux (manubrium clavicule 1ère côte) / rotation post-inf à gde E avec impact sur la colonne vertébrale et l’aorte proximal descendante6.
5. P intraluminale brutale «Water Hammer Effect»5. Pincement osseux (manubrium clavicule 1ère côte) / rotation post-inf à gde E avec impact sur la colonne vertébrale et l’aorte proximal descendante6.")
10
water hammer effect Forces, stress isthme

11
Pincement osseux

12
Mécanismes Traumatismes internes : Iatrogène
Artériographie/Coronarographie Contre pulsion aortique Clampage aortique per opératoire

13
Physiopathologie Classification de Parmley 7 1 hémorragie de l’intima
2 hémorragie intimale avec lacération 3 lacération de la média 4 lacération complète de l’aorte 5 faux anévrysme 6 hémorragie périaortique

14
Artère élastique, 3 tuniques

15
Anatomie Déchirure pariétale transversale et linéaire, trait de refend longitudinal, circonférentielle rare. Dissection-rupture. Isthme 90-98% (ligamentum artériosum). Aorte thoracique descendante 7-12%. Aorte ascendante 5%8. Unique 95% - multiples.
. Aorte thoracique descendante 7-12%. Aorte ascendante 5%8. Unique 95% - multiples.")
16
DIAGNOSTIC

17
Clinique - De 50% ont des symptômes spécifiques 9 Contexte
Douleur thoracique intense migrante - Dyspnée HTA /différentielle MS/MI 40% Souffle diastolique 30% Hémothorax gauche Signes ischémiques (neuro, membre, rein) Paraplégie - Syndrome de pseudo-coarctation Défaillance respiratoire/hémodynamique
 Paraplégie - Syndrome de pseudo-coarctation. Défaillance respiratoire/hémodynamique.")
18
EXAMENS COMPLEMENTAIRES

19
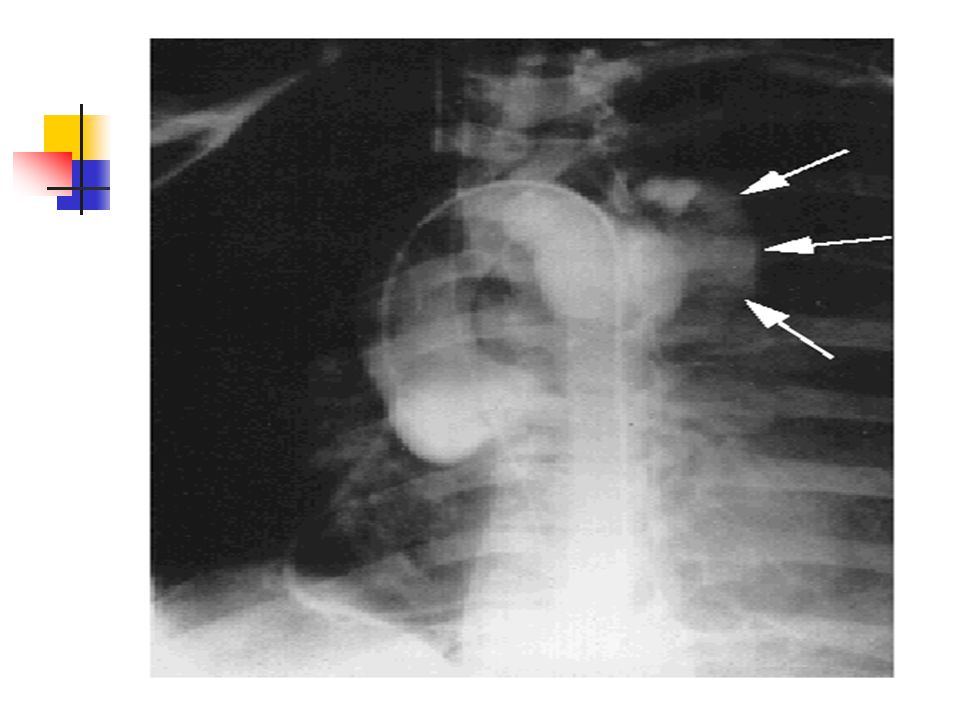
Radiographie thoracique 10
Nle 11 Hématome dôme pleural fracture 1ère côte : 4-19% Elargissement médiastin sup.>8cm 67-85% 12 Hémothorax gauche : 7-19% Effacement du bouton aortique 21-24% Épaississement paratrachéal droit, comblement de la fenêtre aorto-pulmonaire Déviation trachée SNG vers la droite 3-12% Bilan lésionnel Abaissement bronche souche G (faux anévrisme) 4-5%
 4-5%")
20
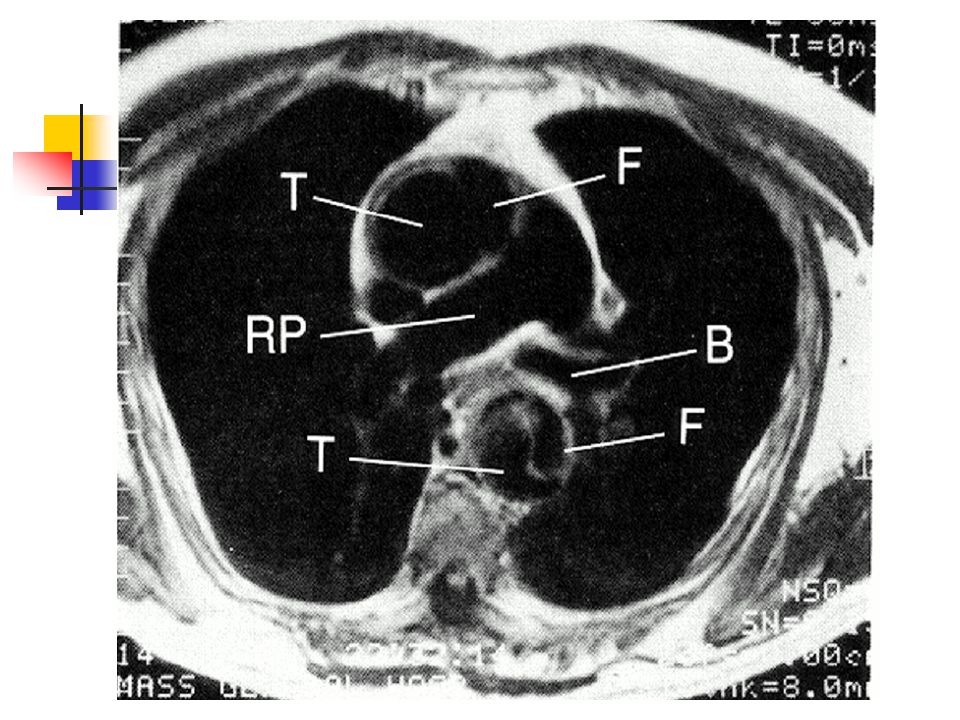
Traumatisme thoracique AVP gde vitesse Diminution du MV à droite
Rupture isthmique

22
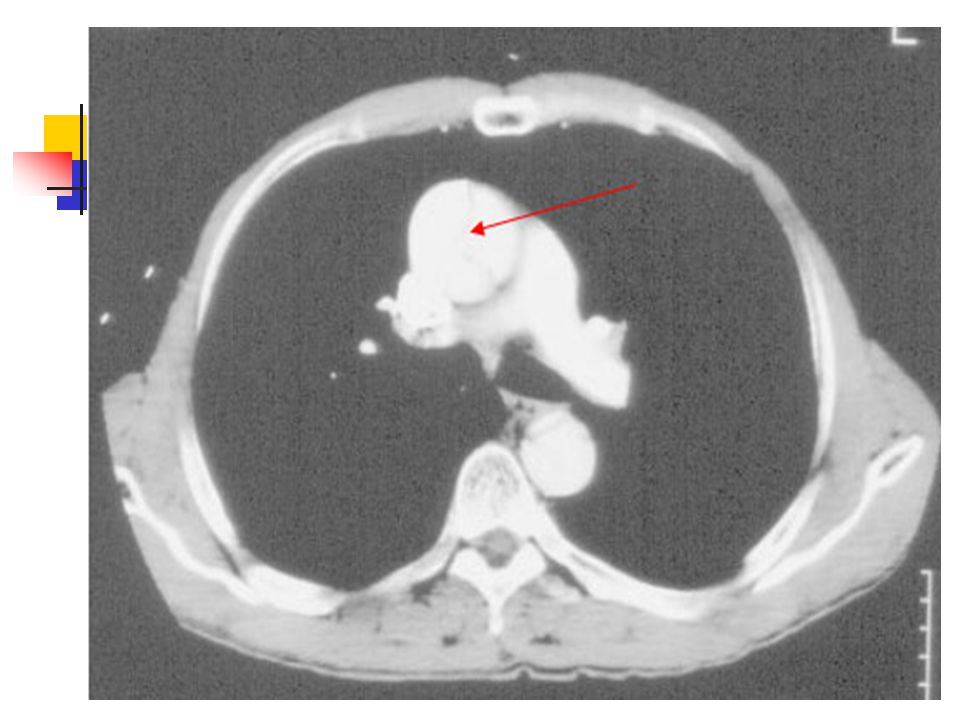
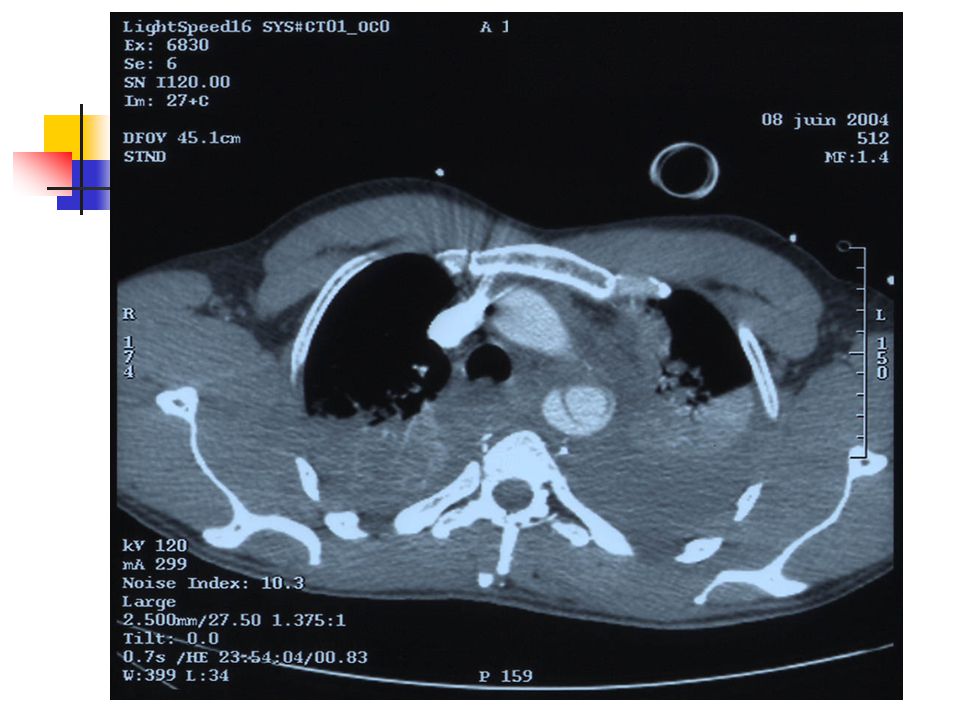
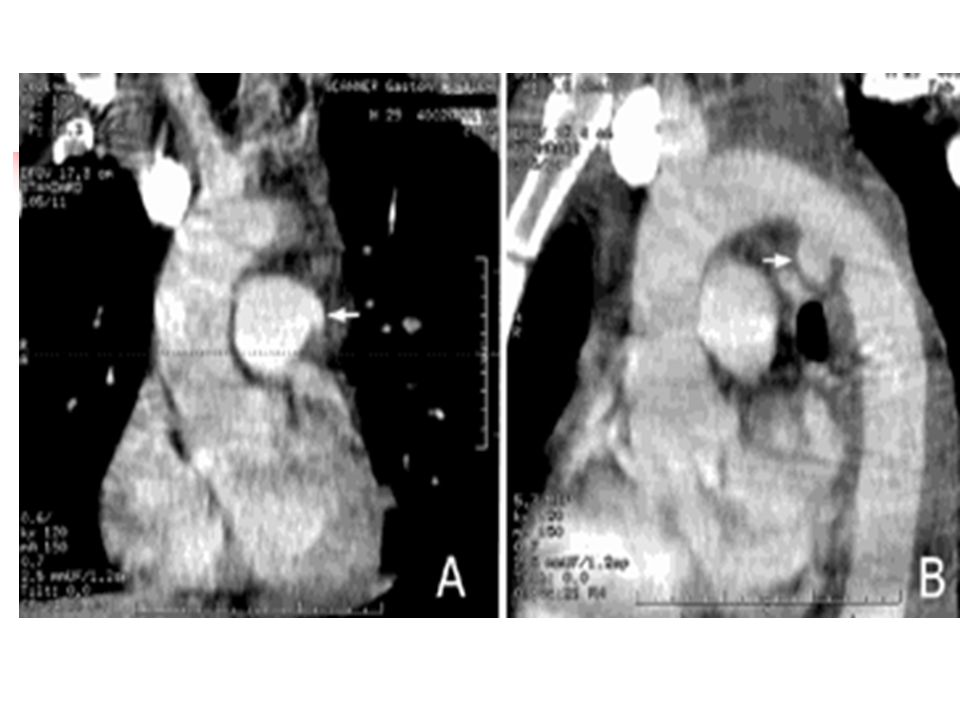
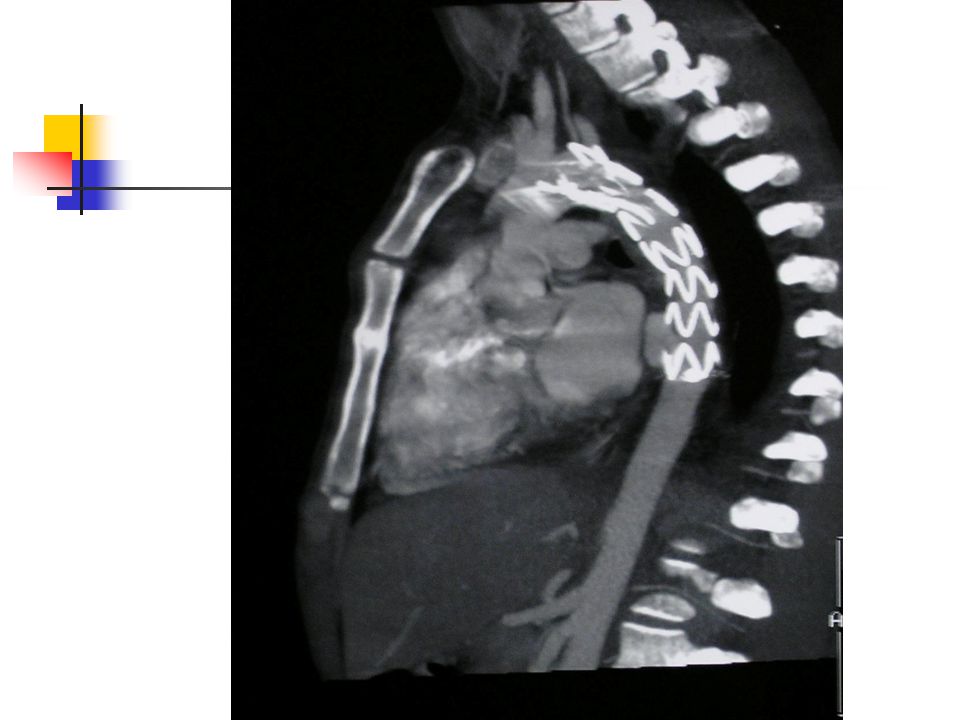
Angioscanner 13 porte d’entrée Reconstruction sagittale-coronale
Sensibilité 100%, spécificité 83-95% 14 VPP 89%,VPN 100% non invasif accès rapide Signes directs faux chenal Flap intimal calibre aorte anévrisme épaississement/irrégularité paroi lacunes intraluminales hématome périaortique Bilan lésionnel vx supra-aortiques suffusion hémorragique Signes indirects hémomédiastin localisé-diffus déviation trachéale/SNG

27
IRM Mais Sensibilité et spécificité Difficile en urgence 100%
Patient stable Avantages Déroule la crosse aortique Pas d’irradiation ni injection d’iode Suivi

28
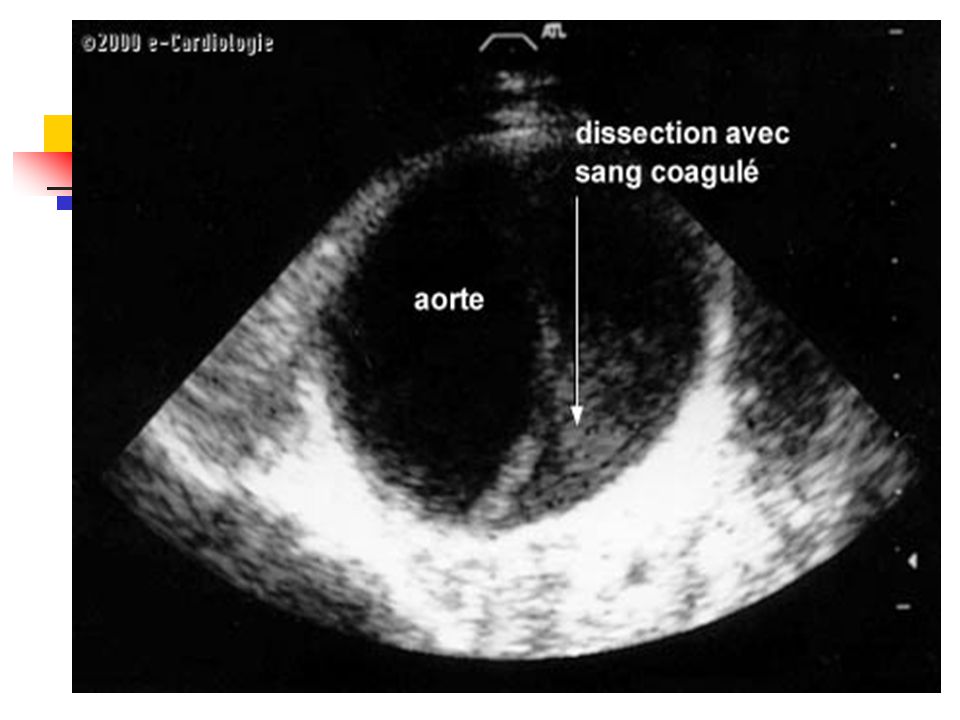
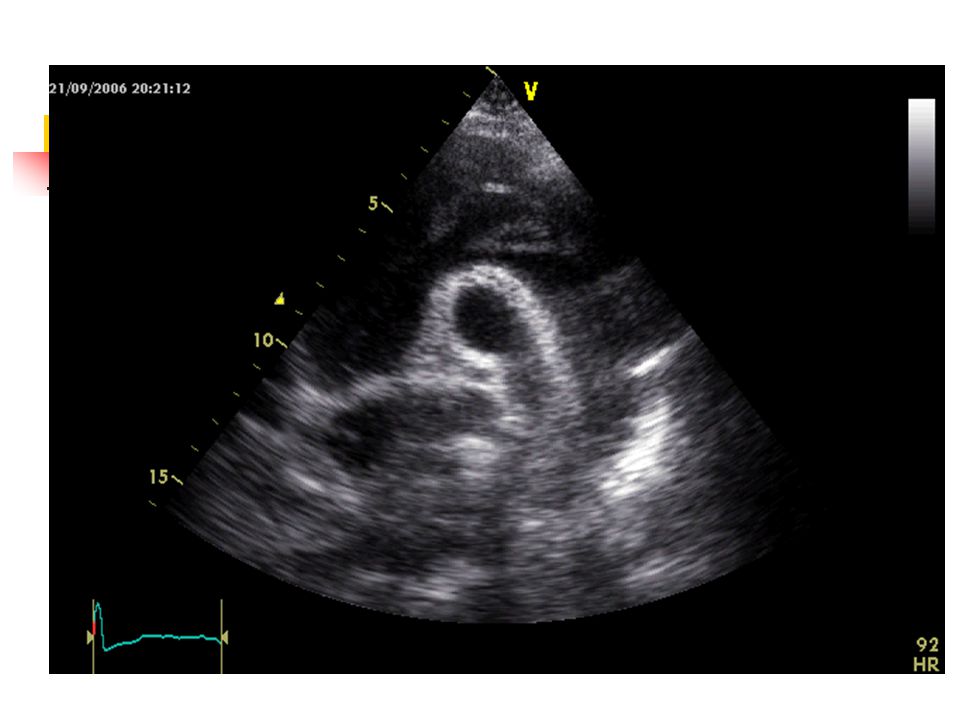
Échographie transoesophagienne
Signes directs flap médial, intimal faux anévrisme dilatation fusiforme hématome pariétal occlusion aortique vrai ou faux chenal Examen de référence se 57%, spé 91%15 Au lit, intubés, ventilés porte d’entrée sans Φ aortique Signes indirects anomalies flux doppler thrombus flottant hémomédiastin Hémodynamique Suivi

29
Limites Opérateur-dépendant Artéfacts Zone aveugle
jonction aorte ascendante-horizontale (pied du tronc artériel brachio-céphalique) CI lésions instables du rachis, délabrement facial
 CI. lésions instables du rachis, délabrement facial.")
32
A stade 3 avec faux anévrisme B stade 2 avec Flap intimal
C stade 2 avec petit Flap D stade 1 avec hématome intramural

35
Aortographie Risques Pintimale injection d’iode Sensibilité 89%
: rupture secondaire Invasif, long, Difficile si patient instable Sensibilité 89% Spécificité 100%15 Voie fémorale rétrograde prudente humérale droite plus sûre16 Interprétation difficile 17 Variantes anatomiques congénitales Ulcérations Porte d’entrée faux anévrisme irrégularité de la paroi Exploration des troncs supra-aortiques Doute au TDM

36
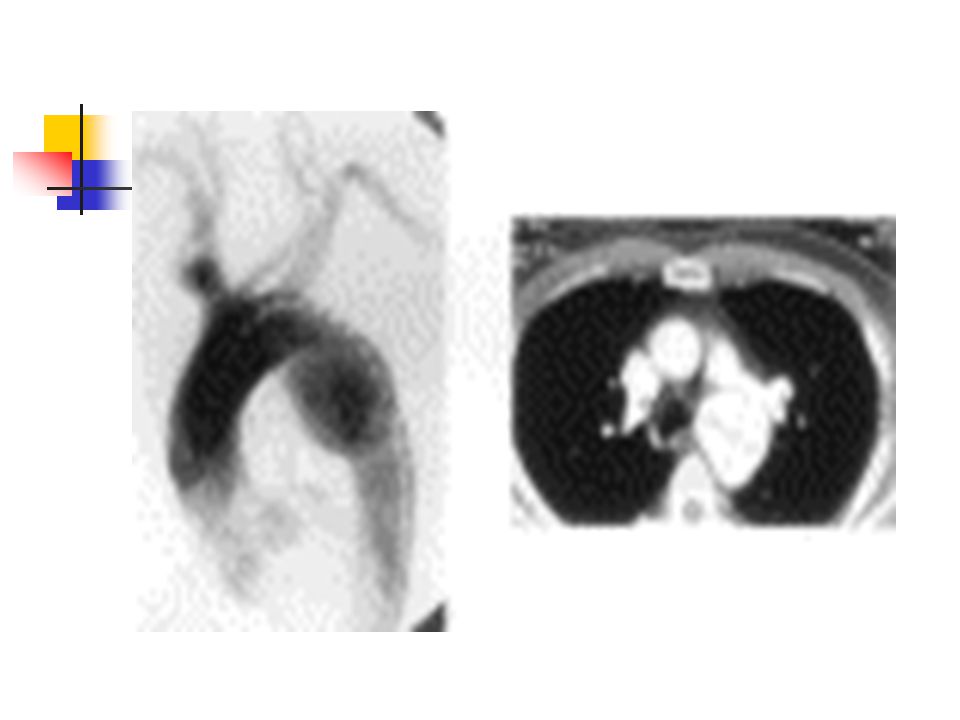
Anévrysme arc aortique inf.
AVP H 48 Anévrysme arc aortique inf.

39
COMPLICATIONS

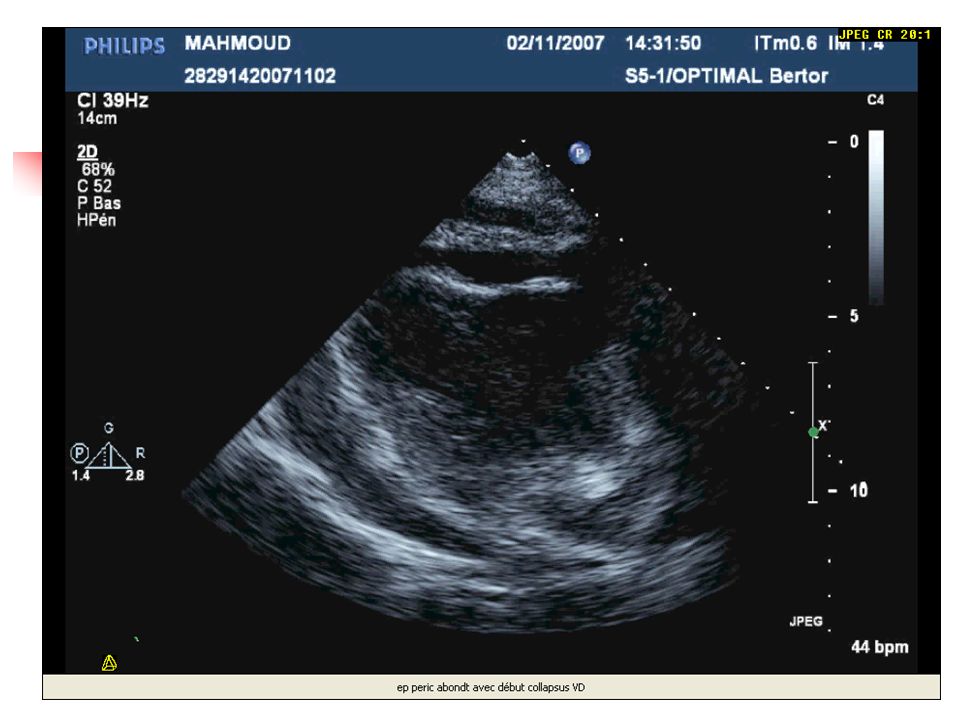
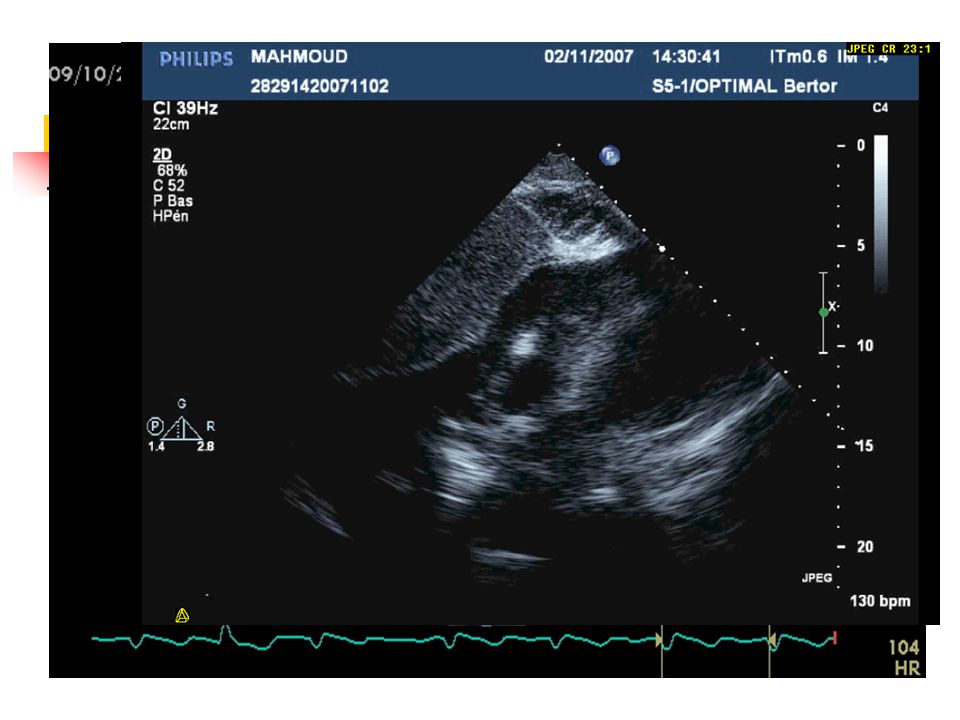
40
Aigues Extension : signes neurologiques, MI, IR Rupture aortique : péricarde, médiastin, plèvre, péritoine, aorte Rupture valve aortique Déchirure artère coronaire IDM Hémopéricarde tamponnade 5 Décés Chronique Anévrysme

43
TRAITEMENT

44
Conditionnement

45
MEDICAL

46
BUT 18 ↓ Psystolique intra-aortique : PAM 60-80 19
Β-bloquant, vasodilatateur, antalgique Stabilité hémodynamique En attente de la chirurgie Groupe à risque 20 Cardiaque : hypokinésie écho, angine, CI BB Neurologique : hémorragie, oedéme, PIC Pulmonaire : contusion + PaO2/FIO2< 300, PEEP>7,5 Coagulopathie

47
CHIRURGIE

48
Techniques Lourde mortalité 8 à 15%23.
Intervention première sur l’aorte sauf si urgence pour craniotomie ou laparotomie. Thoracotomie de sauvetage. Clampage-suture simple : rapide, Φ héparinisation. CEC : ↓ paraplégie, IR. Intérêt d’une technique moins invasive chez les patients à haut risque chirurgical du fait de lésions associées.

49
Circulation de support 19,2% à 2,3%22
Complications Paraplégie clampage sup. 30 min 21 Circulation de support 19,2% à 2,3%22 Insuffisance rénale

50
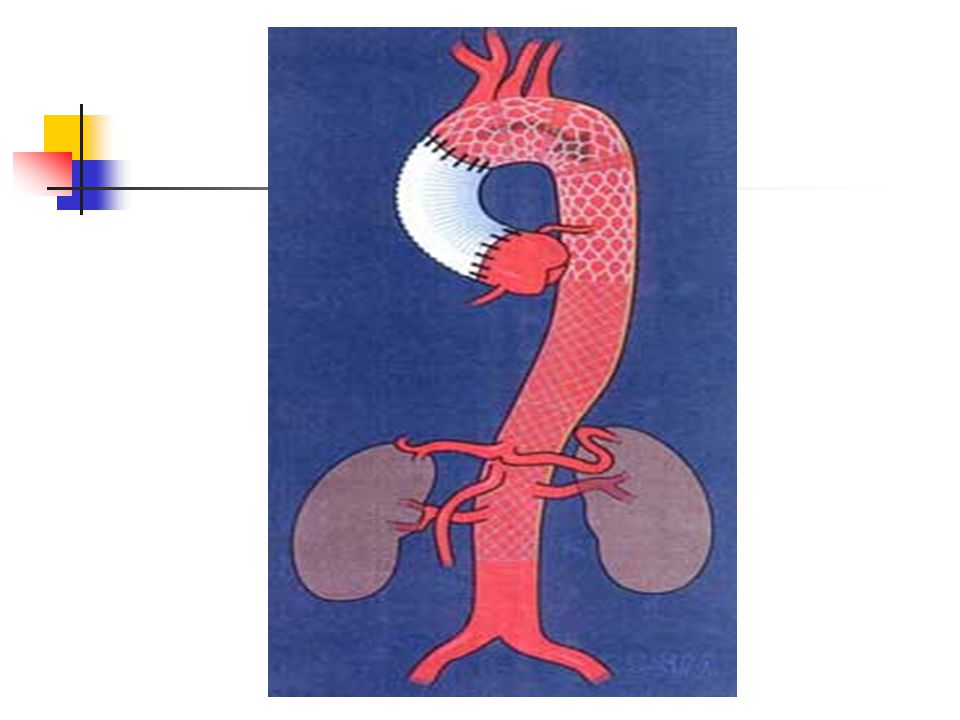
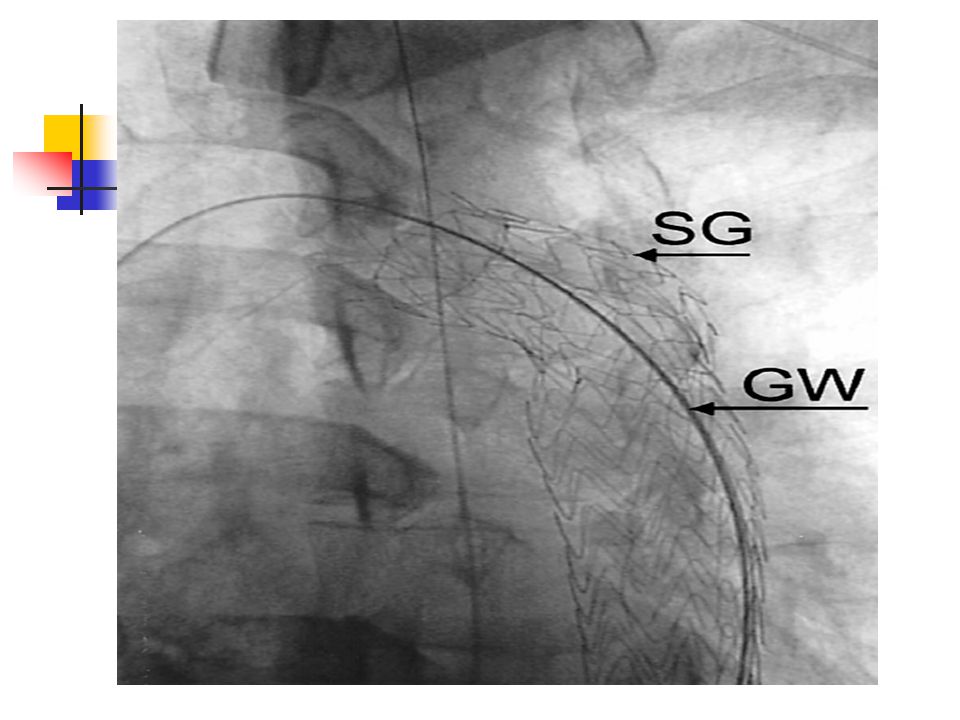
Ttt endovasculaire percutané

51
Stents Grafts Abord fémorale, iliaque ou abdominale
En regard de la porte d’entrée exclusion/thrombose du faux chenal, ↓P, reperfusion viscerale et MI Gpe à risque Faisable et sure 24 Moins invasif Facilement en aigue Pas d’héparinisation Taille fct du TDM CI Trajet tortueux Sténose Thrombose 25 Critères Rupture en distalité de l’ar sous clavière G Φ aorte max 36 mm Absence de thrombus 25

52
Limites Matériel. Opérateur-dépendant.
Topographie, pls portes d’entrée. Complications : dissection aortique rétrograde aigue, pseudo-anévrisme, couverture TSAO, fuite, collapsus, infection, thrombose. A long terme?

54
Stenting de l’ostium carotidien gauche

60
Conclusion Le + fqt : lésion de l’isthme aortique.
Contexte : polytraumatisme. Bilan lésionnel. Mortalité impte. Ttt : stabilité hémodynamique puis fct du patient / des disponibilités locales. Suivi : ETO ou IRM mois puis tous les ans.

61
Bibliographie 1. S. Kodali, W.R.E. Jamieson, M. Leia-Stephens, R.T. Miyagishima, M.T. Janusz and G.F.O. Tyers, Traumatic rupture of the thoracic aorta. A 20-year review : Circulation 84 (1991), pp. 40–46. 2. Fabian TC, Richardson JD, Croce MA, Smith JS Jr, Rodman G Jr, Kearney PA, et al. Prospective study of blunt aortic injury: Multicenter Trial of the American association for the surgery of Trauma. J Trauma 1997;42: 3. Shanmuganathan K, Mirvis SE. Imaging diagnosis of nonaortic thoracic injury. Radiol Clin North Am 1999;37(3):533/51. 4. Burkhart HM,Gomez GA, Jacobson LE, Pless JE, Broadie TA. Fatal blunt aortic injuries:A review of 242 autopsy cases. 5. Creasy JD,Chiles C, Routh WD,Dyer RB.Overview of traumatic injury to the thoracic aorta. RadioGraphics 1997; 17(1):27-45. 6. Esterra A,Mattox KL,Wall MJ.Thoracic aortic injury. Semin Vasc Surg 2000;13: 7. Parmley LF, Mattingly TW, Mariom WC, Jahnke EJ. Nonpenetrating traumatic injury of the aorta. Circulation 1958;17: 1086–1101. 8. Groskin SA. Selected topics in chest trauma. Radiology 1992;183: 9. Gleason TG, Bavaria JE. Trauma to great vessels. In: Cohn LH, Edmunds LH Jr, eds. Cardiac surgery in the adult. New York:McGraw-Hill; 2003: 10. P. Starck, Progress in clinical radiology. In: Radiology of thoracic traumaInvestigative Radiology 25 (1990), pp. 1265–1275.
, pp. 40– Fabian TC, Richardson JD, Croce MA, Smith JS Jr, Rodman G Jr, Kearney PA, et al. Prospective study of blunt aortic injury: Multicenter Trial of the American association. for the surgery of Trauma. J Trauma 1997;42: Shanmuganathan K, Mirvis SE. Imaging diagnosis of nonaortic thoracic injury. Radiol Clin North Am 1999;37(3):533/ Burkhart HM,Gomez GA, Jacobson LE, Pless JE, Broadie TA. Fatal blunt aortic injuries:A review of 242 autopsy cases. 5. Creasy JD,Chiles C, Routh WD,Dyer RB.Overview of traumatic injury to the thoracic aorta. RadioGraphics 1997; 17(1): Esterra A,Mattox KL,Wall MJ.Thoracic aortic injury. Semin Vasc Surg 2000;13: Parmley LF, Mattingly TW, Mariom WC, Jahnke EJ. Nonpenetrating. traumatic injury of the aorta. Circulation 1958;17: 1086– Groskin SA. Selected topics in chest trauma. Radiology 1992;183: Gleason TG, Bavaria JE. Trauma to great vessels. In: Cohn LH, Edmunds LH Jr, eds. Cardiac surgery in the adult. New York:McGraw-Hill; 2003: P. Starck, Progress in clinical radiology. In: Radiology of thoracic traumaInvestigative Radiology 25 (1990), pp. 1265–1275.")
62
11. Mattox KL. Fact and fiction about management of aortic transection
11. Mattox KL. Fact and fiction about management of aortic transection. Ann Thorac Surg 1989;48:1-2. 12. Katyal D,McLellan BA, Brenneman FD, Boulanger BR, Sharkey PW,Waddell JP. Lateral impact motor vehicle collisions: Significant cause of blunt traumatic rupture of the thoracic aorta. J Trauma 1997;42: 13. Dyer DS, Moore EE, Ilke DN, McIntyre RC, Bernstein SM, Durham JD, Mestek MF,Heinig MJ, Russ PD, Symonds DL, Honigman B, Kumpe DA, Roe EJ, Eule J Jr. Thoracic aortic injury: how predictive is mechanism and is chest computed tomography a reliable screening tool? A prospective study of 1,561 patients. J Trauma Apr;48(4):673-82; discussion 14. Fabian TC, Devis KA, Gavant ML, Croce MA, Melton SM, Patton JH et al. Prospective study of blunt aortic injury. Helical CT is diagnostic and antihypertensive therapy reduces rupture. Ann Surg 1998;227:666– Raptopolous V, Sheiman RG. 15. Minard G, Schurr MJ, Croce MA, Gavant ML, Kudsk KA, Taylor MJ et al. A prospective analysis of transesophageal echocardiography in the diagnosis of traumatic disruption of the aorta. J Trauma Injury Infect Crit Care 1996;40:225–230. 16. Lacombe P., Schnyder P, Mesurolle B, Mulot R, Barré O, Chagnon S (1993). Traumatisme fermé des vaisseaux du médiastin et du cœur. Feuillets de Radiologie, 33 (4) :
:673-82; discussion Fabian TC, Devis KA, Gavant ML, Croce MA, Melton SM, Patton JH et al. Prospective study of blunt aortic injury. Helical CT is diagnostic and antihypertensive therapy reduces rupture. Ann Surg 1998;227:666– Raptopolous V, Sheiman RG. 15. Minard G, Schurr MJ, Croce MA, Gavant ML, Kudsk KA, Taylor MJ et al. A prospective analysis of transesophageal echocardiography in the diagnosis of traumatic disruption of the. aorta. J Trauma Injury Infect Crit Care 1996;40:225– Lacombe P., Schnyder P, Mesurolle B, Mulot R, Barré O, Chagnon S (1993). Traumatisme fermé des vaisseaux du médiastin et du cœur. Feuillets de Radiologie, 33 (4) :")
63
reduces rupture. Ann Surg 1998;227:666-677.
17. Fisher RG, Sanchez-Torres M, Whigham CJ, Thomas JW. Lumps and bumps that mimic acute aortic injury and brachiocephalic vessel injury. RadioGraphics 1997;17(4):825/34. 18. Fabian TC,Davis KA, Gavant ML, Croce MA,Melton SM, Patton JH Jr, et al. Prospective study of blunt aortic injury: Helical CT is diagnostic and antihypertensive therapy reduces rupture. Ann Surg 1998;227: 19. Leanne R. Pérez, RN, MS, ACNP,1 and Garrett K. Chan, RN, PhD, CNS, NP2 Clinical Decision Making and Management of Blunt Traumatic Thoracic Aortic Injuries. 20. Camp PC, Shackford SR, The Western Trauma AssociationMulticentre Study Group. Outcome after blunt traumatic thoracic aortic laceration: identification of a high-risk cohort. J Trauma Injury Infect Crit Care 1997;43:413–422. 21. Fabian TC, Richardson DJ, Croce MA, Smith SJ, Rodman G, Kearney PA et al. Prospective study of blunt aortic injury: multicentre trial of the American Association for the Surgery of Trauma. J Trauma Injury Infect Crit Care 1997;42:374–383. 22. Von Oppell UO, Dunne TT, DeGroot MK, Zilla P. Traumatic aortic rupture: twenty-year meta analysis of mortality and risk of paraplegia. Ann Thorac Surg 1994;58:585–593. 23. Jahromi AS, Kazemi K, Safar HA, Doobay B, Cinà CS. Traumatic rupture of the thoracic aorta: cohort study and systematic review. J Vasc Surg Dec;34(6): 24. Pacini D, Angeli E, Fattori R, Lovato L, Rocchi G, Di Marco L et al. Traumatic rupture of the thoracic aorta: ten years of delayed management. J Thorac Cardiavasc Surg 2005;129:880–884
:825/ Fabian TC,Davis KA, Gavant ML, Croce MA,Melton SM, Patton JH Jr, et al. Prospective. study of blunt aortic injury: Helical CT is diagnostic and antihypertensive therapy. reduces rupture. Ann Surg 1998;227: Leanne R. Pérez, RN, MS, ACNP,1 and Garrett K. Chan, RN, PhD, CNS, NP2 Clinical Decision Making and Management of Blunt Traumatic Thoracic Aortic Injuries. 20. Camp PC, Shackford SR, The Western Trauma AssociationMulticentre Study Group. Outcome after blunt traumatic thoracic aortic laceration: identification of a high-risk cohort. J Trauma Injury Infect Crit Care 1997;43:413– Fabian TC, Richardson DJ, Croce MA, Smith SJ, Rodman G, Kearney PA et al. Prospective study of blunt aortic injury: multicentre trial of the American Association for the Surgery of Trauma. J Trauma Injury Infect Crit Care 1997;42:374– Von Oppell UO, Dunne TT, DeGroot MK, Zilla P. Traumatic aortic rupture: twenty-year meta analysis of mortality and risk of paraplegia. Ann Thorac Surg 1994;58:585– Jahromi AS, Kazemi K, Safar HA, Doobay B, Cinà CS. Traumatic rupture of the thoracic aorta: cohort study and systematic review. J Vasc Surg Dec;34(6): Pacini D, Angeli E, Fattori R, Lovato L, Rocchi G, Di Marco L et al. Traumatic rupture of the thoracic aorta: ten years of delayed management. J Thorac Cardiavasc Surg 2005;129:880–884.")
64
25.Buth J, Laheij RJ. Early complications and endoleaks after endovascular abdominal aortic aneurysm repair: report of a multicenter study. J Vasc Surg 2000;31:134–146. 26. Stoica L, Chocron S, Falcoz P, Etievent J. Endovascular stent grafting for contained rupture of the descending thoracic aorta. Eur J Cardiothorac Surg 2003;23:1068–1070.

Présentations similaires