Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez


1
Herpès génital Actualités épidémiologiques et thérapeutiques
Dr. Jean-Elie Malkin Centre Médical de l’Institut Pasteur Esther

2
Primo infection Asymptomatique Symptomatique Latence Réponse immunitaire Stimuli endo/exogènes cellulaire et humorale Réactivation Asymptomatique Subclinique Symptomatique

11
Diagnostic Direct Indirect Culture Détection des antigènes PCR
mise en évidence du virus par prélèvement du liquide contenu dans les vésicules ou érosions fraîches < 3 jours Culture Détection des antigènes PCR Indirect détection des anticorps dirigés contre le virus par prise de sang Sérologie

12
la culture Diagnostic direct : C’est la technique de référence
Résultats en 1 à 5 jours Spécificité +++

13
Diagnostic indirect : La sérologie
Renseigne sur l’état d’immunité du sujet vis-à-vis de l ’HSV De nombreux tests sont disponibles (Elisa ++) Possibilité de tests spécifiques de type (trousses) Est utile principalement pour les études épidémiologiques Grand progrès dans la sensibilité mais encore des faux négatifs (près de 5 %) Dans le diagnostic intérêt pour documenter une primo-infection
 Possibilité de tests spécifiques de type (trousses) Est utile principalement pour les études épidémiologiques. Grand progrès dans la sensibilité mais encore des faux. négatifs (près de 5 %) Dans le diagnostic intérêt pour documenter une. primo-infection.")
14
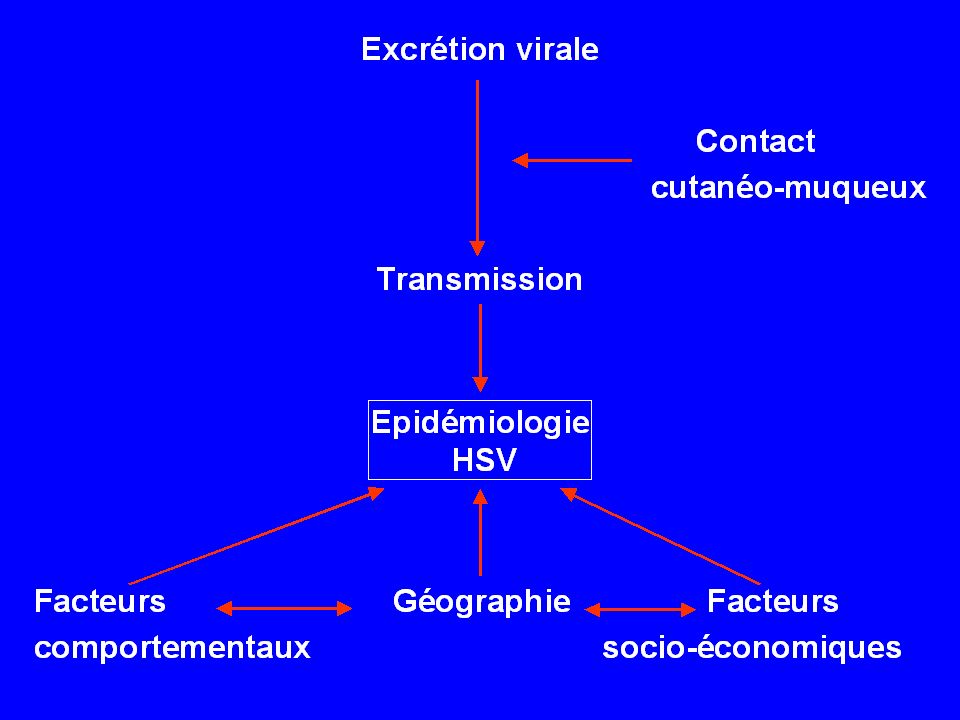
Epidémiologie de l ’infection à HSV2

15
CoreyL. Sex Transm Dis. 1994

16
Données séro épidémiologiques
Grande variabilité géographique Europe de l ’Ouest : % U.S.A. : % Afrique : %

17
U.S.A. France Augmentation de la séroprévalence de 30%
NHANES II % NHANES III % Augmentation de la séroprévalence de 30% France HERPIMAX 4412 sérums recueillis en 1996, population générale femmes > 35 ans, hommes > 45 ans femmes 17.9% Séroprévalence globale 17.2% hommes 13.7% Johnson RE New Engl J Med. 1989 Fleming DT. New Engl J Med. 1997 Malkin JE. 39th Iccac San Francisco. 1999

18
Epidémiologie de l’infection à HSV-2 en Afrique subsaharienne
Etudes séro-épidémiologiques Devenues possibles gâce à la sérologie spécifique de type Ouganda, Tanzanie, Zimbabwe, Afrique du Sud Forte prévalence chez les jeunes : Moins de 20 ans : 20-30% Adultes jeunes : 60-80% Femmes plus infectées que les hommes Etiologies des ulcérations génitales (2001) HSV-2 > Chancre mou > Syphilis Excrétion génitale asymptomatique Très peu de données Femmes enceintes VIH+ au Kenya : 17% de portage cervical (Mostad et al. J Infect Dis 2000;181:58-63)
 HSV-2 > Chancre mou > Syphilis. Excrétion génitale asymptomatique. Très peu de données. Femmes enceintes VIH+ au Kenya : 17% de portage cervical. (Mostad et al. J Infect Dis 2000;181:58-63)")
19
Yaounde HIV-1: 7% W, 3.6% M HSV-2: 51% W, 27% M Cotonou HIV-1: 2.8% W, 2.8% M HSV-2: 30% W, 12% M Kisumu HIV-1: 29% W, 18% M HSV-2: 68% W 35% M Ndola HIV-1: 32% W, 24% M HSV-2: 55% W, 36% M

20
Facteurs de risques Age Sexe féminin Facteurs ajustés sur l ’âge
Nombre de partenaires sexuels Age du premier rapport sexuel Antécédents de MST Niveau socio-économique faible Malkin JE. 38th ICCAC San Diego. 1998 Fleming DT. New Engl J Med. 1997 Wald A. Sex Transm Dis. 1997

21
Transmission 144 couples sérodifférents HSV2
Taux annuel de transmission : 10% 70% des cas de transmission survenus alors que le sujet source était asymptomatique Différence liée au sexe femme homme : 4.5% homme femme : 19% Suivi d ’une cohorte de 7046 femmes enceintes Taux d ’acquisition de 33% pour HSV2 (4% pour HSV1) Mertz GJ. Ann Intern Med. 1992 Brown ZA. N Engl J Med. 1997
 Mertz GJ. Ann Intern Med Brown ZA. N Engl J Med")
22
Transmission of Herpes Simplex Virus type 2 among factory workers in Ethiopa
Yenew Kebede et al. J of Infect Dis. 2004;190:

23
Retrospective study 1612 subjects (including 133 heterosexual couples) HSV2 seroprevalence at enrollment : 40.9% (female : 59.5 – male: 34.6) ; 43.4% y
 ; 43.4% y.")
24
41 monogamous HSV2 serodiscordant couples
12 with man HSV2 + 29 with woman HSV2 + HSV2 seroincidence was: 20.7 seroconversions /100 PY in women 4.9 seroconversions /100 PY in men

25
Majority of HSV2 + subjects did not report any episode of genital ulcer (>90%)
symptoms are unnoticed and/or underreported probable reason of the widespread dissemination of HSV2 infection

26
Increasing relative prevalence of HSV2 infection among men with genital ulcers from a mining community in South Africa Lai W et al. Sex Transm Infect. 2003;79:

27
HSV2 as a cause of GUD increased from 17
HSV2 as a cause of GUD increased from 17.2% to 36% between 1994 and 1998

28
Etiology of GUD in South Africa (1986-98)
Chen CY, Ballard RC et al. Sex Transm Dis. 2000;27:21-29

29
Herpès génital chez des malades africains souffrant d’ulcération génitale : Evolution 1980-1999
Pourcentage de HSV-2 isolé D’après O’Farrell STI 1999

30
Genital shedding of herpes simplex virus type 2 in childbearing-age and pregnant women living in Gabon Ozouaki F et al. Int J of STD & AIDS,2005

31
355 subjects recruited blood and cervicovaginal samples collected HSV2 seroprevalence : 65.9% increasing with age (peak within the range y) Prevalence of HSV2 DNA genital shedding was 13.8% on a single sampling episode

32
This high prevalence of HSV 2 shedding may be associated with high risk of HSV 2 vertical transmission to neonates Which in Africa may be higher than that observed in developed world due to : high incidence of HSV2 infection high fertility rates in African high HIV prevalence young women

33
Treatment of genital herpes old trends revisited and new directions

34
Treatment of primary genital herpes (primo-infection or primo-manifestation) ACV
> 10 RCTs vs PBO: Viral shedding: 7 days Pain: 1-5 days Healing: 3-10 days Dosage 200 mg x 5 per day or 5 mg/kg/8hrs, 7-10 days Similar efficacy of oral and IV ACV (valaciclovir 500 mg or 1000 mg bid could also be used if oral therapy is appropriate)
")
35
Episodic treatment of recurrent genital herpes oral ACV
6 RCTs vs PBO: mild effect-size Viral shedding: 1-2 days Pain: no effect Healing: 1-2 days Other limitations To be administered as early as possible (should be patient-initiated as for the other antiviral drugs) Dosage: 5 times per day for 5 days
 Dosage: 5 times per day for 5 days.")
36
Episodic treatment of recurrent genital herpes
VACV 500 mg bid is equivalent to ACV 200 mg 5 times daily, 5 days FCV 125 mg bid is equivalent to ACV 200 mg 5 times daily, 5 days ACV 800 mg tid, 2 days, may be used A 3-day course of VACV 500 mg bid is equivalent to the 5-day course of VACV Bodsworth N et al. Genitourin Med 1997;73:110-6 Chosidow O et al. BJD 2001;144:818-24 Wald A et al. CID 2004;34:944-8 Leone PA et al. CID 2004;34:958-62

37
Suppressive treatment of recurrent genital herpes
Daily use of an antiviral drug in order to suppress or delay time to recurrence In patients with at least 6 recurrences/year

38
Suppressive treatment of recurrent genital herpes A meta-analysis (Lebrun-Vignes B, Bouzamoundo A, Dupuy A, Guillaume JC, Lechat Ph, Chosidow O) Immunocompetent patients, suppressive treatment of recurrent genital herpes, RCTs vs PBO 14 RCTs (6158 patients)
")
39
Global analysis

40
Once-daily VACV to reduce the risk of transmission of genital herpes (Corey L et al. NEJM 2004;350:11-20) . IC, heterosexual, monogamous couples: one with clinically symptomatic genital HSV-2 and one susceptible (n =1484) . Partner HSV-2 + randomly assigned to VACV 500 mg OD or PBO for 8 months . Acquisition of HSV-2: HR = 0.52 (95%CI = ) (decrease in clinically symptomatic HSV-2 infection) . Decrease in viral shedding (33%)
 . Partner HSV-2 + randomly assigned to VACV 500 mg OD or PBO for 8 months. . Acquisition of HSV-2: HR = 0.52 (95%CI = ) (decrease in clinically symptomatic HSV-2 infection) . Decrease in viral shedding (33%)")
41
“The herpetic connection”
Interactions HSV2 / HIV “The herpetic connection”

42
Genital Herpes: Early AIDS-associated Opportunistic Infection

44
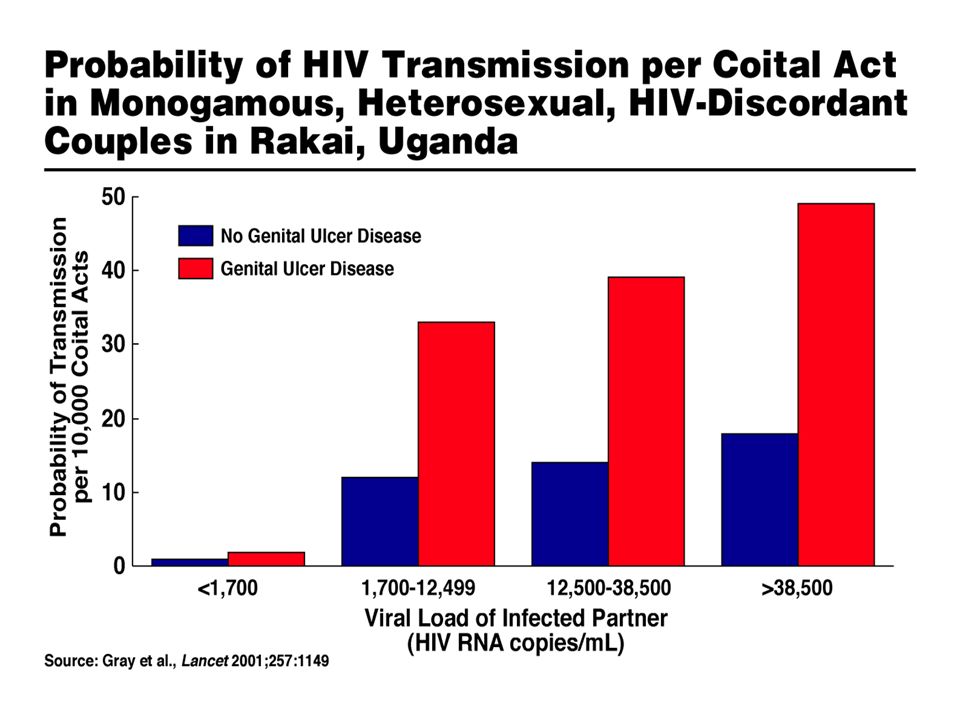
acquisition du HIV HSV2 transmission du HIV Mécanismes
Rupture de la barrière épithéliale Afflux de cellules cibles au niveau de la lésion

45
HSV2 cofacteur de transmission en cas de UG
Nairobi : cohorte de prostituées présentant une UG 34% PCR (+) HIV DNA Sur 31 prélèvements PCR (+) HSV2 DNA : 22% PCR (+) HIV DNA U.S.A. : 12 homosexuels HSV2 (+) HIV (+) 25 poussées/26 PCR (+) HIV DNA Kreiss JK. J Infect Dis. 1989 Schacker T. JAMA. 1998
 HIV DNA. Sur 31 prélèvements PCR (+) HSV2 DNA : 22% PCR (+) HIV DNA. U.S.A. : 12 homosexuels HSV2 (+) HIV (+) 25 poussées/26 PCR (+) HIV DNA. Kreiss JK. J Infect Dis Schacker T. JAMA")
47
HSV2 cofacteur de transmission en cas d ’excrétion asymptomatique
Bangui : étude cas-témoins chez des femmes coinfectées HSV2-HIV Corrélation significative entre HSV2 DNA et HIV DNA au niveau des sécrétions cervico-vaginales en dehors de toute poussée Mbopi-KéouFX. J Infect Dis. 2000

48
HSV-2 and HIV acquisition meta-analysis:
Risk of HIV infection in HSV-2 infected persons: A: 9 Longitudinal & nested case-control studies: RR=2.1 ( ) B: 22 Case-control & cross sectional studies: OR=3.9 ( ) Wald A. JID: 2002;185:45-52
 B: 22 Case-control & cross sectional studies: OR=3.9 ( ) Wald A. JID: 2002;185:")
49
The Impact of Incident and Prevalent Herpes Simplex Virus-2 Infection on the incidence of HIV-1 Infection Among Commercial Sex Workers in South Africa Ramjee G. et al. J Acquir Immune Defic Syndr. 2005:39(3)
")
50
416 women screened : 50% HIV + 84% HSV2 +

51
187 HIV negative women followed up monthly (median duration 2.2 years)
When HSV2 seroconversion was analysed as a time-dependant covariate, the RR for HIV seroconversion was 6.0 times greater among women with incident that among women with prevalent HSV2 infection

52
2 types d’essais d’intervention thérapeutique en cours
1 : Effet d’un traitement antiherpétique (épisodique et suppressif) chez les coinfectés HSV2/HIV sur la baisse de l’infectivité 2 : Effet d’un traitement suppressif chez les sujets HSV2 + sur l’incidence de l’infection HIV
 chez les coinfectés HSV2/HIV sur la baisse de l’infectivité. 2 : Effet d’un traitement suppressif chez les sujets HSV2 + sur l’incidence de l’infection HIV.")
53
ESSAI ANRS 12-12 (Ghana et République Centrafricaine)
WAPTCAS, Ghana CNRMST & FACSS, RCA Inserm U430, HEGP, Paris, FRANCE LSHTM, London, UK University of Sherbrooke, Canada Sponsors: ANRS (France,) Groupe de travail AC 12 “Microbicides et Prévention de la Transmission Sexuelle du VIH” Paris, le 4 mars 2005
 Groupe de travail AC 12 Microbicides et Prévention de la Transmission Sexuelle du VIH Paris, le 4 mars")
55
Study Design * LeGoff J et al,
Multicentre, randomised, double-blind placebo-controlled trial Syndromic Mx + Placebo Ciprofloxacin + Benzathine penicillin 2.4 MU D2 D4 D7 D14 D28 Randomisation Syndromic Mx + Acyclovir ACV 400 mg x 3/d - 5 days D0 Outcomes* HIV-1 RNA Lesional, genital and plasma HSV-2 DNA Lesional and genital Ulcer aetiologies Ulcer healing Acrra/Kumasi Bangui * LeGoff J et al, J Clin Microbiol 2006;44: 24/05/06 - AC12 Paris

56
Results at Baseline 24/05/06 - AC12 Paris

57
Population characteristics
441 women randomized HIV-1 seropositive % Median CD4+=270; IQR= HSV-2 seropositive % HIV-1/ HSV-2 sero % HSV-2 prevalence HIV-1 prevalence 96% 100 P<0.01 P<0.001 80 64% 57% 60 40 20 10% HIV+ HIV- HSV2+ HSV2- 24/05/06 - AC12 Paris

58
Ulcer aetiologies (N=422/441)
HSV-2 in 211 = 50.0% 1 co-infected with H. ducreyi and 3 with C trachomatis (not LGV strains) H. ducreyi alone in 2 samples = 0.5% 209 unknown aetiologies = 49.5% Ulcer swabs were found also positive CMV alone in 4 samples = 1.0% EBV alone in 24 samples = 4.5% CMV+EBV in 5 samples = 1.2% 24/05/06 - AC12 Paris
 H. ducreyi alone in 2 samples = 0.5% 209 unknown aetiologies = 49.5% Ulcer swabs were found also positive. CMV alone in 4 samples = 1.0% EBV alone in 24 samples = 4.5% CMV+EBV in 5 samples = 1.2% 24/05/06 - AC12 Paris.")
59
occured more frequently among HIV-1 + women
Genital HSV-2 shedding 388/407 CVL without semen contamination Genital HSV-2 DNA Ulcer +/- CVL= (Ulcer = 188; Ulcer + CVL = 131; CVL only = 14) Primary Genital Herpes (HSV-2 seroneg) = 24 Freq HSV-2 shedding Mean CVL HSV-2 DNA % 100 1 2 3 4 5 6 NS 80 P<0.001 60 log10 copies/ml 40 3.85 4.13 54% 20 23% HIV+ HIV- HIV+ HIV- N=184 N=204 N=98 N=47 Genital HSV-2 shedding occured more frequently among HIV-1 + women 24/05/06 - AC12 Paris
 Primary Genital Herpes (HSV-2 seroneg) = 24. Freq HSV-2 shedding. Mean CVL HSV-2 DNA. % NS. 80. P< log10 copies/ml % % HIV+ HIV- HIV+ HIV- N=184. N=204. N=98. N=47. Genital HSV-2 shedding. occured more frequently among HIV-1 + women. 24/05/06 - AC12 Paris.")
60
Genital HIV-1 shedding in HIV-1/HSV-2 co-infected women
% HIV-1 RNA in CVL Median CV HIV-1 RNA (log10 copies/mL) 100 6 P=0.001 P=0.003 80 5 4 60 3 40 2 68% 42% 3.14 2.1 20 1 HSV-2 DNA Positive Negative Positive Negative N=109 N=71 Genital HIV-1 shedding among women shedding HSV-2: Occured more frequently Associated with higher viral loads 1 log10 CV HSV-2 DNA 2-fold CV HIV-1 RNA 24/05/06 - AC12 Paris
 P= P= % 42% HSV-2 DNA. Positive. Negative. Positive. Negative. N=109. N=71. Genital HIV-1 shedding among women shedding HSV-2: Occured more frequently. Associated with higher viral loads. 1 log10 CV HSV-2 DNA 2-fold CV HIV-1 RNA. 24/05/06 - AC12 Paris.")
61
Results Impact Study 24/05/06 - AC12 Paris

62
Enrolment, follow-up, compliance
490 women presented Mean compliance rate (pill count) = 99% in both arms Side effects = 8/441 (2%, severity 1 or 2) 449 eligible 441 randomized 220 Placebo arm 221 ACV arm 54 HIV+ with HSV2 ulcer 52 analysed on day 7 (81%) 42 analysed on day 7 (78%) 64 HIV+ with HSV2 ulcer Primary analysis group: 118 HIV+ women with HSV-2 ulcer 24/05/06 - AC12 Paris
 = 99% in both arms. Side effects = 8/441 (2%, severity 1 or 2) 449 eligible. 441 randomized. 220 Placebo arm. 221 ACV arm. 54 HIV+ with HSV2 ulcer. 52 analysed on day 7 (81%) 42 analysed on day 7 (78%) 64 HIV+ with HSV2 ulcer. Primary analysis group: 118 HIV+ women with HSV-2 ulcer. 24/05/06 - AC12 Paris.")
63
Participants characteristics in primary analysis group (HIV+ women with HSV-2 ulcers) (N=118)
4.76 ( ) 4.63 ( ) Mean plasma HIV-1 RNA (CI) 6% 5% NG/CT/TV 11% 8% Taking HAART 47% 42% Experienced GUD last year 3% Serological syphilis TPHA/RPR+ 194 (92-548) 188 (72-519) Median CD4 count (/µL) (IQR) 30.8 31.4 Mean age in years SM+ACV (n=54) SM+Placebo (n=64) 24/05/06 - AC12 Paris
 4.63 ( ) Mean plasma HIV-1 RNA (CI) 6% 5% NG/CT/TV. 11% 8% Taking HAART. 47% 42% Experienced GUD last year. 3% Serological syphilis TPHA/RPR+ 194 (92-548) 188 (72-519) Median CD4 count (/µL) (IQR) Mean age in years. SM+ACV. (n=54) SM+Placebo. (n=64) 24/05/06 - AC12 Paris.")
64
Impact of ACV on HIV-1 RNA at day 7
Cervico-vaginal detection RR*=0.97 ( ) % * Adjusted for baseline CV HIV-1 RNA Cervico-vaginal and plasma HIV-1 RNA loads No impact on mean cervico-vaginal HIV-1 RNA at day 7 among shedders (-0.06 log10 copies/mL, P=0.69) No impact on mean plasma HIV-1 RNA at day 14 (0.02 log10 copies/mL, P=0.89) 24/05/06 - AC12 Paris
 % * Adjusted for baseline. CV HIV-1 RNA. Cervico-vaginal and plasma HIV-1 RNA loads. No impact on mean cervico-vaginal HIV-1 RNA at day 7 among shedders (-0.06 log10 copies/mL, P=0.69) No impact on mean plasma HIV-1 RNA at day 14 (0.02 log10 copies/mL, P=0.89) 24/05/06 - AC12 Paris.")
65
Impact of ACV on HSV-2 shedding at day 7
Reduction from: 81% at D0 to 26% at day 7 in acyclovir arm, 81% at D0 to 35% at day 7 in placebo arm => RR=0.74 (P=0.35) Mean quantity HSV-2 DNA was 1.12 log10 copies/mL lower in acyclovir arm than placebo arm (P=0.005) 24/05/06 - AC12 Paris
 Mean quantity HSV-2 DNA was 1.12 log10 copies/mL lower in acyclovir arm than placebo arm (P=0.005) 24/05/06 - AC12 Paris.")
66
Impact on ulcer healing at day 7 in HIV+ women with HSV-2 ulcers
0.03 RR=1.60 58% 42% 0% 10% % with ulcers <10 mm2 0.25 P- value RR=1.26 % ulcers with >90% size reduction* 55% 44% ACV Plac. D7 D0 Magnitude * Excluding ulcers size <10 mm2 at baseline 24/05/06 - AC12 Paris

67
ANRS1212: Conclusions First results from a large cohort of women with symptomatic genital herpes in Africa HSV-2 the dominant GUD aetiology Large % of primary genital herpes HSV-2 genital infectiousness of HIV-1 CV HIV-1 RNA plasma HIV-1 RNA (as Mole JID 1997; Schacker JID 2002) Importance of HIV testing to be offered to GUD patients x 2.5 > x 10 Asymptomatic Shedding Genital Ulcer (Baeten JID 2004) 24/05/06 - AC12 Paris
 Importance of HIV testing to be offered to GUD patients. x 2.5. > x 10. Asymptomatic. Shedding. Genital Ulcer. (Baeten JID 2004) 24/05/06 - AC12 Paris.")
68
ANRS1212: Conclusions Despite some impact on HSV-2, episodic treatment with ACV has no measurable impact on HIV-1 replication Too little/too short (5 days)? Too late? (median 7 days after ulcer first noticed by woman) Advanced HIV disease in many women Delayed impact? Inadequate outcome (D7?), sample size, etc? Await results of other trials in Malawi and South Africa Prevention of HSV-2 reactivations perhaps more effective in controlling HSV and HIV transmissibility 24/05/06 - AC12 Paris
 Too late (median 7 days after ulcer first noticed by woman) Advanced HIV disease in many women. Delayed impact Inadequate outcome (D7 ), sample size, etc Await results of other trials in Malawi and South Africa. Prevention of HSV-2 reactivations perhaps more effective in controlling HSV and HIV transmissibility. 24/05/06 - AC12 Paris.")
69
Acknowledgements CNRMST, Bangui WAPCAS, Ghana
Gerard Gresenguet, Jean-de- Dieu Longo WAPCAS, Ghana Thomas Agyarko-Poku, Comfort Asamoah-Adu, Agnes Dzokoto, Khonde Nzambi Sherbrooke University, Canada Sylvie Deslandes, Eric Frost, Jacques Pepin HPA, London David Brown, John Parry Institut Pasteur, Paris Jean-Elie Malkin INSERM U743, Paris Laurent Belec, Jerome LeGoff, Hicham Bouhlal, Cecile Chemin, Maxime Lecerf, Ali Si-Mohamed LSHTM, London Richard Hayes, David Mabey, Philippe Mayaud, Helen Weiss Scientific Advisors Yaw Adu-Sarkodie, Francis Ndowa (WHO), Jamie Robinson (GSK R&D), Simon Cousens, Mike Kenward, David Dunn, Andrew Nunn, Jean-Marie Huraux DSMB Peter Smith (Chair, LSHTM), Tim Clayton (LSHTM), Anne Johnson (Royal Free) 24/05/06 - AC12 Paris
, Jamie Robinson (GSK R&D), Simon Cousens, Mike Kenward, David Dunn, Andrew Nunn, Jean-Marie Huraux. DSMB. Peter Smith (Chair, LSHTM), Tim Clayton (LSHTM), Anne Johnson (Royal Free) 24/05/06 - AC12 Paris.")
70
Prospective sites for Gates HSV-HIV transmission trial
Nairobi, Eldoret, Kisumu, Kenya Kitwe and Ndola, Zambia Kampala, Uganda Moshi, Tanzania Gabarone, Botswana Johannesburg, Durban RSA

71
HSV-2 suppressive therapy to prevent HIV transmission
3646 HIV- discordant couples HSV-2 serology & CD4 testing of HIV+ partner Randomize HIV+/HSV2 + persons w/ CD4 > 250 Aciclovir 400 mg bid x 1 yr Placebo x 1 yr 1° endpoint: HIV infection in HIV-negative partners at 1 yr

72
1800 high-risk, HIV-/ HSV2+ MSM
Proof-of-concept trial of HSV-2 suppressive therapy to prevent HIV acquisition 1800 HIV-/ HSV2+ heterosexual women and 1800 high-risk, HIV-/ HSV2+ MSM Harare, Zimbabwe Lusaka, Zambia Johannesburg, SA Lima, Peru Seattle, USA San Francisco, USA New York, USA Randomize Aciclovir 400 mg bid x 1 yr Placebo x 1 yr 1° endpoint: HIV infection (estimated to be 3.5%/yr in placebo arm)
")
73
Glycoprotein-D-adjuvant vaccine to prevent genital herpes (Stanberry LR et al. NEJM 2002;347: ) Two double blind, randomized, placebo-controlled trials Study 1 (57 centers) randomized 847 both HSV-1 and HSV-2 seronegative partners of HSV-2 infected persons (clinically confirmed genital herpes) Study 2 (60 centers) randomized 1867 HSV-2 seronegative partners of HSV-2 infected persons (clinically confirmed genital herpes) Vaccinations: 0, 1, and 6 months – I.m. administration Follow-up period: 19 months Primary efficacy endpoint: Acquisition of genital herpes disease
 randomized 847 both HSV-1 and HSV-2 seronegative partners of HSV-2 infected persons (clinically confirmed genital herpes) Study 2 (60 centers) randomized 1867 HSV-2 seronegative partners of HSV-2 infected persons (clinically confirmed genital herpes) Vaccinations: 0, 1, and 6 months – I.m. administration. Follow-up period: 19 months. Primary efficacy endpoint: Acquisition of genital herpes disease.")
74
Genital Herpes Disease
STUDY 1- HSV-2 VACCINE Genital Herpes Disease HSV 1-/2- Subjects Men Women 85 90 95 100 Vaccine Placebo 20 10 30 Vaccine Placebo 85 90 95 100 Percentage without GHD 20 10 30 Observation period [months] Observation period [months]

75
Genital Herpes Disease
STUDY 2- HSV-2 VACCINE Genital Herpes Disease HSV 1-/2- Subjects Men Women 20 10 30 85 90 95 100 Placebo Vaccine 20 10 30 85 90 95 100 Placebo Vaccine Percentage without GHD Observation period [months] Observation period [months]

76
Genital Herpes Disease
STUDY 2- HSV-2 VACCINE Genital Herpes Disease HSV 1+/2- Subjects Men Women Placebo Vaccine 20 10 30 85 90 95 100 Placebo Vaccine 20 10 30 85 90 95 100 Percentage without GHD Observation period [months] Observation period [months]

Présentations similaires















 and associated factors in HIV-infected patients,>")













