Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Radiotherapeutical options to avoid Mucositis and Xerostomia
Salivary Gland Tumors : Radiotherapeutical options to avoid Mucositis and Xerostomia René-Jean Bensadoun Head of Radiotherapy Department, Centre Antoine-Lacassagne, 06189-NICE Cedex 2 (France).
.")
2
Salivary Gland tumors are considered as Radioresistant
and Chemoresistant lesions. For these tumors, the role of new radiation modalities, (i.e. IMRT, heavy ions therapy, neutrontherapy) is emphasized. I will shortly present the radiotherapeutical options to avoid Mucositis and Xerostomia in Salivary Gland Tumors.
 is emphasized. I will shortly present the radiotherapeutical options. to avoid Mucositis and Xerostomia in Salivary Gland. Tumors.")
3
RT Parotids (3DCRT) Photons + e-
 Photons + e-")
4
RT Sub-mandibular Glands
Photons + e-

5
Problem : Radioresistant (and chemoresistant) lesions
-> Limited effect of classical photontherapy on bulky disease (unresectable cases or macroscopical residual tumor after surgery)
")
6
+ French Network for Rare French National Guidelines (SOR)
Head and Neck Tumors (REFCOR) French National Guidelines (SOR)
 French National Guidelines (SOR)")
7
Arbre 3 : Prise en charge thérapeutique du patient atteint d’une tumeur des glandes salivaires de stade II (T1b-T2b-T3a N0 M0) de bas grade Stade II (T1b-T2b-T3a N0 M0) de bas grade Standard : Chirurgie tumorale et ganglionnaire. oui Résection macroscopiquement OU microscopiquement incomplète OU présence de ganglions envahis non Standards : Radiothérapie postopératoire tumorale et ganglionnaire. Pas de chimiothérapie. Standards : Pas de radiothérapie postopératoire. Pas de chimiothérapie. Modalités des thérapeutiques Exérèse chirurgicale tumorale Standards : Exérèse chirurgicale complète si tumeur localisée aux GSP. Exérèse chirurgicale élargie si tumeur localisée aux GSA. Option : Chirurgie élargie mutilante si tumeur étendue aux éléments nobles (nerf VII, fosse infra temporale, mandibule, base du crâne). Curage ganglionnaire Standard : Prophylactique modifié de type 3 et sélectif (groupes I, II, III) et bilatéral si lésions médianes. Radiothérapie postopératoire tumorale et ganglionnaire * Standard : Unilatérale sauf si lésions médianes ou bilatérale. Standards de dose : Sur le site tumoral : dose totale équivalente de 65 Gy si exérèse incomplète. Sur les aires ganglionnaires : dose totale équivalente de 50 Gy. Options : Hadronthérapie (ions carbone ou neutrons) si réalisable en cas de reliquat tumoral macroscopiquement volumineux. Photonthérapie de haute énergie (RC3D). * La neutronthérapie n'est plus disponible en France depuis la fermeture récente de l'Unité de Neutronthérapie d'Orléans mais l’émergence de nouvelles techniques telles que la radiothérapie conformationnelle en 3 dimensions (RC3D) ou la radiothérapie conformationnelle avec modulation d'intensité (RCMI), permet d’apporter d’autres options de même que les projets français d’hadronthérapie.
 de bas grade. Standard : Chirurgie tumorale et ganglionnaire. oui. Résection macroscopiquement. OU microscopiquement incomplète. OU présence de ganglions envahis. non. Standards : Radiothérapie postopératoire tumorale et ganglionnaire. Pas de chimiothérapie. Standards : Pas de radiothérapie postopératoire. Pas de chimiothérapie. Modalités des thérapeutiques. Exérèse chirurgicale tumorale. Standards : Exérèse chirurgicale complète si tumeur localisée aux GSP. Exérèse chirurgicale élargie si tumeur localisée aux GSA. Option : Chirurgie élargie mutilante si tumeur étendue aux éléments nobles (nerf VII, fosse infra temporale, mandibule, base du crâne). Curage ganglionnaire. Standard : Prophylactique modifié de type 3 et sélectif (groupes I, II, III) et bilatéral si lésions médianes. Radiothérapie postopératoire tumorale et ganglionnaire * Standard : Unilatérale sauf si lésions médianes ou bilatérale. Standards de dose : Sur le site tumoral : dose totale équivalente de 65 Gy si exérèse incomplète. Sur les aires ganglionnaires : dose totale équivalente de 50 Gy. Options : Hadronthérapie (ions carbone ou neutrons) si réalisable en cas de reliquat tumoral macroscopiquement volumineux. Photonthérapie de haute énergie (RC3D). * La neutronthérapie n est plus disponible en France depuis la fermeture récente de l Unité de Neutronthérapie d Orléans mais l’émergence de nouvelles techniques telles que la radiothérapie conformationnelle en 3 dimensions (RC3D) ou la radiothérapie conformationnelle avec modulation d intensité (RCMI), permet d’apporter d’autres options de même que les projets français d’hadronthérapie.")
8
de stade III (T3b-T4a N0 M0, tout T (sauf T4b) N1 M0) de bas grade
Arbre 4 : Prise en charge thérapeutique d’un patient atteint d’une tumeur des glandes salivaires de stade II (T1b-T2b-T3a N0 M0) de haut grade ou de stade III (T3b-T4a N0 M0, tout T (sauf T4b) N1 M0) de bas grade Stade II (T1b-T2b-T3a N0 M0) de haut grade ou Stade III (T3b-T4a N0 M0, tout T (sauf T4b) N1 M0) de bas grade Standard : Chirurgie tumorale et ganglionnaire. oui Résection macroscopiquement OU microscopiquement incomplète OU présence de ganglions envahis ? non Standards : Radiothérapie postopératoire tumorale et ganglionnaire. Pas de chimiothérapie. Standard : Pas de chimiothérapie. Option : Radiothérapie postopératoire tumorale (photons, 50 Gy) Modalités des thérapeutiques : Exérèse chirurgicale tumorale Standards : Exérèse chirurgicale complète si tumeur localisée aux GSP. Exérèse chirurgicale élargie si tumeur localisée aux GSA. Option : Chirurgie élargie mutilante si tumeur étendue aux éléments nobles (nerf VII, fosse infra temporale, mandibule, base du crâne). Curage ganglionnaire Standard : pas d’attitude standard. Options : Bilatéral si lésions médianes. Complet homolatéral conservateur. Curage ganglionnaire Standards : Bilatéral si lésions médianes. Complet, conservateur ou non conservateur, homolatéral à l’adénopathie cliniquement envahie en cas de lésion N1. Radiothérapie postopératoire tumorale ou ganglionnaire * Standard : Unilatérale sauf si lésions médianes ou bilatérale. Standards de dose : Sur le site tumoral : dose totale équivalente de 65 Gy si exérèse incomplète. Sur les aires ganglionnaires : dose totale équivalente de 50 Gy. Options : Hadronthérapie (ions carbone ou neutrons) si réalisable en cas de reliquat tumoral macroscopiquement volumineux. Photonthérapie de haute énergie (RC3D ou RCMI). * La neutronthérapie n'est plus disponible en France depuis la fermeture récente de l'Unité de Neutronthérapie d'Orléans mais l’émergence de nouvelles techniques telles que la radiothérapie conformationnelle en 3 dimensions (RC3D) ou la radiothérapie conformationnelle avec modulation d'intensité (RCMI), permet d’apporter d’autres options de même que les projets français d’hadronthérapie.
 de haut grade ou. de stade III (T3b-T4a N0 M0, tout T (sauf T4b) N1 M0) de bas grade. Stade II (T1b-T2b-T3a N0 M0) de haut grade ou. Stade III (T3b-T4a N0 M0, tout T (sauf T4b) N1 M0) de bas grade. Standard : Chirurgie tumorale et ganglionnaire. oui. Résection macroscopiquement. OU microscopiquement incomplète. OU présence de ganglions envahis non. Standards : Radiothérapie postopératoire tumorale et ganglionnaire. Pas de chimiothérapie. Standard : Pas de chimiothérapie. Option : Radiothérapie postopératoire tumorale (photons, 50 Gy) Modalités des thérapeutiques : Exérèse chirurgicale tumorale. Standards : Exérèse chirurgicale complète si tumeur localisée aux GSP. Exérèse chirurgicale élargie si tumeur localisée aux GSA. Option : Chirurgie élargie mutilante si tumeur étendue aux éléments nobles (nerf VII, fosse infra temporale, mandibule, base du crâne). Curage ganglionnaire. Standard : pas d’attitude standard. Options : Bilatéral si lésions médianes. Complet homolatéral conservateur. Curage ganglionnaire. Standards : Bilatéral si lésions médianes. Complet, conservateur ou non conservateur, homolatéral à l’adénopathie cliniquement envahie en cas de lésion N1. Radiothérapie postopératoire tumorale ou ganglionnaire * Standard : Unilatérale sauf si lésions médianes ou bilatérale. Standards de dose : Sur le site tumoral : dose totale équivalente de 65 Gy si exérèse incomplète. Sur les aires ganglionnaires : dose totale équivalente de 50 Gy. Options : Hadronthérapie (ions carbone ou neutrons) si réalisable en cas de reliquat tumoral macroscopiquement volumineux. Photonthérapie de haute énergie (RC3D ou RCMI). * La neutronthérapie n est plus disponible en France depuis la fermeture récente de l Unité de Neutronthérapie d Orléans mais l’émergence de nouvelles techniques telles que la radiothérapie conformationnelle en 3 dimensions (RC3D) ou la radiothérapie conformationnelle avec modulation d intensité (RCMI), permet d’apporter d’autres options de même que les projets français d’hadronthérapie.")
9
Heavy ions therapy Neutrontherapy

11
* Radiotherapy Department, Centre Antoine-Lacassagne,
Parotid Gland Sparing with Step-and-Shoot IMRT in Oropharyngeal and Nasopharyngeal Tumors. 5 years Experience at the Centre Antoine-Lacassagne, NICE (France). René-Jean Bensadoun *, Serge Marcié *, Cécile Ortholan*, Benjamin Serrano *, Elisabeth Charpiot*, Jean-Pierre Gérard *. * Radiotherapy Department, Centre Antoine-Lacassagne, 06189-NICE Cedex 2 (France).
. René-Jean Bensadoun *, Serge Marcié *, Cécile Ortholan*, Benjamin Serrano *, Elisabeth Charpiot*, Jean-Pierre Gérard *. * Radiotherapy Department, Centre Antoine-Lacassagne, NICE Cedex 2 (France).")
12
PRIMUS linear accelerator
pharynx IMRT Methods Linear Accelerator PRIMUS (Siemens) 1997 #003 Simtec, Primeview Lantis network RX 6 MV, 300 UM/min «step and shoot» IMRT technique Inverse treatment planning TMS 6.0 (Helax – MDS NORDION) ONCENTRA MasterPlan (Nucletron) "pencil beam" "collapsed cone" PRIMUS linear accelerator
 1997 #003. Simtec, Primeview. Lantis network. RX 6 MV, 300 UM/min. «step and shoot» IMRT technique Inverse treatment planning. TMS 6.0 (Helax – MDS NORDION) ONCENTRA MasterPlan (Nucletron) pencil beam collapsed cone PRIMUS linear accelerator.")
13
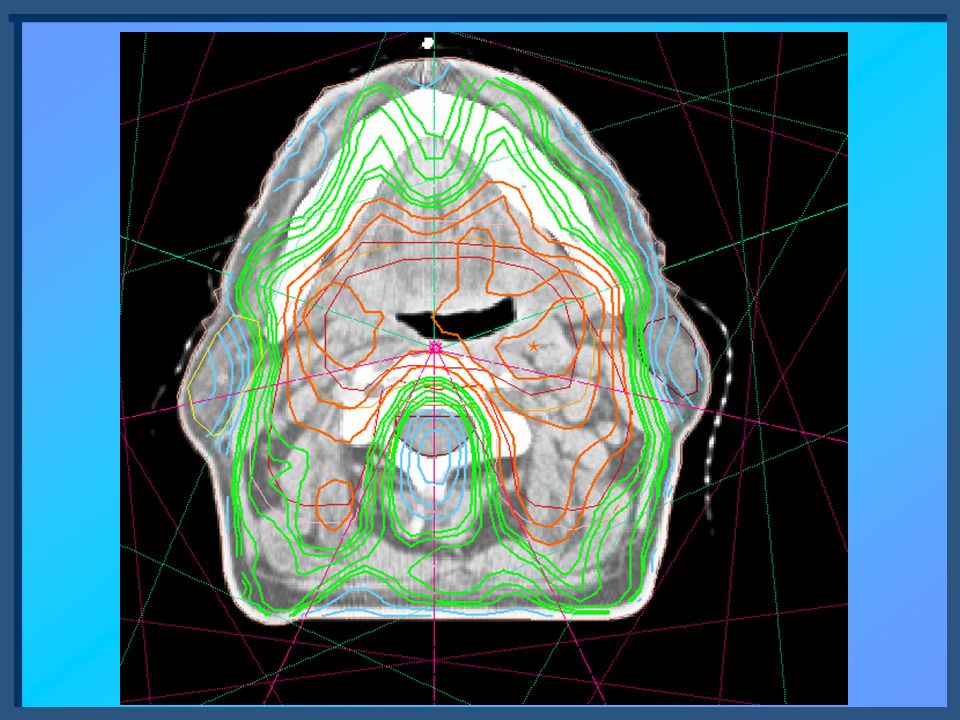
Figure 1: Comparison of IMRT, 3D conformal and traditional parallel opposed field plans for the treatment of primary nasopharynx tumors IMRT D CONFORMAL 2D TRADITIONAL Gy PTV BRAINSTEM/SPINAL CORD 13

14
Conformal radiotherapy and IMRT
in Head and Neck Tumors IMRT Process : Courtesy of V. Gregoire

15
CT Scan MRI (T1) 18F-FDG PET
 18F-FDG PET")
17
Examples of fluence matrix

18
Quality Assurance Program
Validation of Treatment Plan OUR PROCESS : 1) « In vitro » control
 « In vitro » control.")
19
Comparison Calculated dose distribution Matrix
Optical densities distribution Measured dose distribution Film

20
2) Control of the patient position
 Control of the patient position")
21
Anterior DRR Anterior DRR for daily verification of patient position.

22
Lateral DRR Case 2 : 49 yrs old man. Undifferentiated carcinoma of nasopharynx T2N1. Radiation treatment only, 70 Gy on nasopharynx, 50 Gy on bilateral cervical nodes, 56 Gy on level 1 and level 2 left cervical nodes.

23
X-Ray control of one segment (oblique field at 85°)
")
24
3) « In vivo » control
 « In vivo » control")
25
During treatment, daily in vivo dosimetry was performed, using low diameter Mosfet dosimeters (implemented in patient’s mouth thanks to a customized plastic mould).
.")
26
Customized plastic mould

27
MOSFET detectors The diagram shows a cross-section through a Metal Oxide Semiconductor Field Effect Transistor (MOSFET) structure. The layers shown are a) Metal Gate electrode, b) SiO2 Oxide layer, c) Si substrate. A current can only pass through the MOSFET from Source to Drain contacts only if a negative voltage exists on the Gate electrode. In this condition the MOSFET is “ON”. If there is no voltage on the Gate, the MOSFET is “OFF”. The voltage required to switch the MOSFET ON is called the “Threshold Voltage”, designated Vt. The MOSFET acts as a gate-controlled switch and this is how it is normally used in electronic circuits (e.g. computer logic chips). If ionizing radiation passes through the SiO2 layer, electron-hole pairs are formed (c.f. TLD). The holes (+ ve charge) are trapped at the Si/SiO2 interface. This trapped charge acts to screen the Gate potential and a higher value of Vt is required to switch the MOSFET “ON”. The MOSFET dosimeter uses the above principles as follows: 1. Vt is measured before irradiation (by Reader instrument). 2. MOSFET is irradiated with a + ve bias on the Gate (using Bias Supply) to drive holes into the traps and increase sensitivity. 3. Vt is re-measured after irradiation and the difference between pre- and post- Vt values is proportional to absorbed dose. (Vt changes with dose are ~ 1 to 3 mV/cGy, depending on Gate bias used)
 structure. The layers shown are a) Metal Gate electrode, b) SiO2 Oxide layer, c) Si substrate. A current can only pass through the MOSFET from Source to Drain contacts only if a negative voltage exists on the Gate electrode. In this condition the MOSFET is ON . If there is no voltage on the Gate, the MOSFET is OFF . The voltage required to switch the MOSFET ON is called the Threshold Voltage , designated Vt. The MOSFET acts as a gate-controlled switch and this is how it is normally used in electronic circuits (e.g. computer logic chips). If ionizing radiation passes through the SiO2 layer, electron-hole pairs are formed (c.f. TLD). The holes (+ ve charge) are trapped at the Si/SiO2 interface. This trapped charge acts to screen the Gate potential and a higher value of Vt is required to switch the MOSFET ON . The MOSFET dosimeter uses the above principles as follows: 1. Vt is measured before irradiation (by Reader instrument). 2. MOSFET is irradiated with a + ve bias on the Gate (using Bias Supply) to drive holes into the traps and increase sensitivity. 3. Vt is re-measured after irradiation and the difference between pre- and post- Vt values is proportional to absorbed dose. (Vt changes with dose are ~ 1 to 3 mV/cGy, depending on Gate bias used)")
28
This anterior view allows localization of Mosfet detector

29
This lateral view allows localization of Mosfet detector

30
Salivary Flow measurement
-> To confirm the clinical impact of parotid gland sparing with IMRT, measurement of salivary flow, before and after 5 minute stimulation (with Parafilm) was performed at D0, at the end of treatment, at 3 months, and will be performed every 6 months during 2 yrs.
 was performed at D0, at the end of treatment, at 3 months, and will be performed every 6 months during 2 yrs.")
31
To verify the clinical impact of this technique, a measurement of salivary flow (before and after stimulation with Parafilm*) is performed, as I said before, at D0, at 3 months, at 6 months, and will be performed every 6 months during 2 yrs.
 is performed, as I said before, at D0, at 3 months, at 6 months, and will be performed every 6 months during 2 yrs.")
32
RESULTS

33
Dose Prescribed Oropharynx (30 patients) :
Prophylactic dose (CTV1) : Gy Curative dose (CTV2) : Gy Nasopharynx (14 patients) : Prophylactic dose (nodes only) (CTV1) : Gy
 : Gy. Curative dose (CTV2) : Gy. Nasopharynx (14 patients) : Prophylactic dose (nodes only) (CTV1) : Gy.")
34
Dosimetric Comparisons
For those patients, we performed 2 types of Radiotherapy plans, and we made dosimetric comparisons regarding dose distribution in PTVs, Spinal Canal and Parotid glands (superficial and deep lobes).
.")
35
Mean Dose to the contralateral parotid
RESULTS: Dosimetric Comparison Mean Dose to the contralateral parotid IMRT : Mean: 28.1 Gy (range 5.5 Gy-44.1 Gy) Median: Gy RC3D : Mean: 47.4 Gy (range 25.7 Gy-64.1 Gy) Median: Gy
 Median: 29.4 Gy. RC3D : Mean: 47.4 Gy. (range 25.7 Gy-64.1 Gy) Median: 48.2 Gy.")
36
Mean Dose to Contralateral Parotid Gland

37
Mean dose to the Parotids :
Step and shoot IMRT in our experience leads to : 21 % decrease in mean dose for the ipsilateral gland 41 % decrease in mean dose for the controlateral gland +++

38
Evolution of Measured Salivary Flow

39
RCMI (Evolution du flux salivaire pour chaque patient)
Avec stimulation par Parafilm

40
RC3D (Evolution du flux salivaire pour chaque patient) Avec stimulation par Parafilm
 Avec stimulation par Parafilm")
41
Evolution of Stimulated salivary Flow after Radiation (IMRT vs RC3D)
3 mois p=0,004 12 mois p=0,05 18 mois p=0,04

42
Slight mucositis 18 days after the end of radiation

43
Radiation-Induced Mucositis(G3) Chemo-Induced Mucositis(G3)
 Chemo-Induced Mucositis(G3)")
45
Slobodan - Nice

46
Thank You for your Attention
Thank You for your Attention ! Hope to welcome you soon on the French Riviera !! 46

Présentations similaires


















 / Information about the study trip to Strasbourg (29th-31st March 2009) Château de.>")


