Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Simplification Thérapeutique
Dr Jean Luc Meynard , Dr Pierre de Truchis

2
Simplificaction Thérapeutique
Ce que l’on souhaite discuter avec VOUS Monothérapie Bithérapie Réduction posologique Traitements séquentiels STR Déboost

3
Cas N 1 Mr M 59 ans Infection par le VIH depuis 92 Jamais d’IO
Nadir CD4 100 A reçu successivement monothérapie d’AZT , puis AZT+ 3TC ( non indétectable) Mis sous Zerit Epivir Crixivan/r depuis 1996 Toujours indétectable Sauf au moment d’un switch par TRIZIVIR ( CV copies/ml) Génotype a cette époque M41L, D67N, K70R, L210W, T215A, M184V Résistance ABC, AZT, 3TC, D4T, resistance possible TDF
 Mis sous Zerit Epivir Crixivan/r depuis Toujours indétectable. Sauf au moment d’un switch par TRIZIVIR ( CV copies/ml) Génotype a cette époque. M41L, D67N, K70R, L210W, T215A, M184V. Résistance ABC, AZT, 3TC, D4T, resistance possible TDF.")
4
Cas N 1 Actuellement Très lipo atrophique CD4 500/mm3 CV < 20 cp/ml
Sous metformine depuis 2 ans avec HbA1C à 6,5% Sous tt anti HTA depuis 2ans (protéinurie a 0,5 g/l) Sous crestor depuis 3 ans ( paramètres lipidique OK) Clearance créat à 60ml/mn Le médecin qui l a repris en charge vous sollicite pour un avis
 Sous crestor depuis 3 ans ( paramètres lipidique OK) Clearance créat à 60ml/mn. Le médecin qui l a repris en charge vous sollicite pour un avis.")
5
Que propoez vous ? 2 INTI + IP/r 2 INTI + INNTI 2 INTI + INI
Monotherapie IP Bitherapie IP + INNTI Bithérapie IP + INI Autres options thérapeutiques

6
Cas N 1 Ce qui a été fait Monothérapie par Prézista/r (800/100)
Correction lipoatrophie Poursuite statine

7
Quelle réponse chez quels patients ?
MONARK[1] Initiation M03-613[2] Induction/Maintenance OK04[3] Simplification 100 80 60 Patients (%) LPV, lopinavir; RTV, ritonavir. One of the concerns about boosted PI monotherapy is whether patients have continuing low-level viremia. This slide compares the proportion of patients with low-level viremia in lopinavir/ritonavir monotherapy trials in each of the 3 settings: initial therapy, induction-maintenance, and simplification. The green areas show the proportion of patients with HIV-1 RNA < 50 copies/mL; it is clear that the best results are obtained with the simplification strategy. The blue areas represent patients who develop HIV-1 RNA of copies/mL and again the best results are with the simplification strategy; compared with patients using the induction-maintenance strategy, the green area (suppression) was smaller and the blue area (low-level viremia) was larger. (We should reemphasize that some patients being treated with the induction-maintenance strategy had been undetectable for only 2 months whereas in the simplification strategy trials, patients were virologically suppressed for at least 6 months.) If we now turn our attention to the orange area (HIV-1 RNA > 400 copies/mL), few patients in the simplification trial had residual viremia at this level. This may be attributed to the trial strategy in which these patients were adherent to and successful with combination therapy for at least 6 months before simplifying therapy. 40 20 16 32 48 16 32 48 64 80 96 12 24 36 48 Wk Wk Wk Ré-intensification HIV-1 RNA HIV-1 RNA > 400 HIV-1 RNA < 50 1. Delfraissy JF, et al. AIDS. 2008;22: Cameron DW, et al. J Infect Dis. 2008;198: Published by University of Chicago. 3. Arribas J, et al. J Acquir Immune Defic Syndr. 2005;40:
 LPV, lopinavir; RTV, ritonavir. One of the concerns about boosted PI monotherapy is whether patients have continuing low-level viremia. This slide compares the proportion of patients with low-level viremia in lopinavir/ritonavir monotherapy trials in each of the 3 settings: initial therapy, induction-maintenance, and simplification. The green areas show the proportion of patients with HIV-1 RNA < 50 copies/mL; it is clear that the best results are obtained with the simplification strategy. The blue areas represent patients who develop HIV-1 RNA of copies/mL and again the best results are with the simplification strategy; compared with patients using the induction-maintenance strategy, the green area (suppression) was smaller and the blue area (low-level viremia) was larger. (We should reemphasize that some patients being treated with the induction-maintenance strategy had been undetectable for only 2 months whereas in the simplification strategy trials, patients were virologically suppressed for at least 6 months.) If we now turn our attention to the orange area (HIV-1 RNA > 400 copies/mL), few patients in the simplification trial had residual viremia at this level. This may be attributed to the trial strategy in which these patients were adherent to and successful with combination therapy for at least 6 months before simplifying therapy Wk. Wk. Wk. Ré-intensification. HIV-1 RNA HIV-1 RNA > 400. HIV-1 RNA < Delfraissy JF, et al. AIDS. 2008;22: Cameron DW, et al. J Infect Dis. 2008;198: Published by University of Chicago. 3. Arribas J, et al. J Acquir Immune Defic Syndr. 2005;40:")
8
MONET & MONOI 99 100 100 94.1 82 80 78 80 60 60 40 40 Non infériorité
MONOI 48 Wks[2] MONET 96 Wks[1] PP Analysis TLOVR, S = F 99 100 100 94.1 82 80 78 = -5.8% (-16.0% to +4.4%) 80 Lower limit of 90% CI: 60 60 Patients Meeting Primary Endpoint /%) 40 40 Non infériorité Non démontrée Non infériorité 20 20 127 129 112 113 DRV/RTV Mono DRV/RTV + 2 NRTIs DRV/RTV Mono DRV/RTV + 2 NRTIs Switch (Intensification With NRTIs) Allowed ITT Analysis 100 93 100 92.0 92 87.5 CI, confidence interval; DRV, darunavir; ITT, intent to treat; PP, per protocol; RTV, ritonavir; TLOVR, time to loss of virologic response. The panel on the left of this slide illustrates the results of the MONET trial at 96 weeks. The primary endpoint for MONET was 48 weeks; at that time, the intent-to-treat, time to loss of virologic response analysis showed that darunavir/ritonavir monotherapy was noninferior to darunavir/ritonavir plus 2 NRTIs. However, the 96-week data indicated that monotherapy was not noninferior by the same analysis; almost 75% of the monotherapy patients were undetectable through 96 weeks compared with almost 81% of the patients in the darunavir/ritonavir plus 2 NRTIs arm. Interestingly, there was a larger number of patients with hepatitis C virus (HCV) randomized to the darunavir/ritonavir monotherapy arm (19% vs 12% in the triple combination arm). The investigators hypothesized that adherence might not have been as good among the HCV-coinfected patients. HCV coinfection (and IV drug use) was correlated with the primary endpoint outcome. The diagram at the bottom of this column shows that patients who had documented virologic failure on darunavir/ritonavir monotherapy were able to resuppress HIV-1 RNA with reintensification with NRTIs. When use of this strategy was not counted as virologic failure, the monotherapy arm was noninferior to the triple-therapy arm: 92% of patients in the monotherapy arm and 90.7% of patients on triple therapy suppressed HIV-1 RNA to < 50 copies/mL. Results from the MONOI study of darunavir/ritonavir monotherapy are shown in the right-hand panel of the slide; again there are 2 analyses. One is the per-protocol analysis, which shows that monotherapy was noninferior to triple combination therapy with high rates of success (94% vs 99%, respectively) in maintaining virologic suppression. On the other hand, the intent-to-treat analysis shows that monotherapy was not noninferior: 87.5% of patients in the darunavir/ritonavir monotherapy arm vs 92% of patients in the darunavir/ritonavir plus 2 NRTIs arm achieved virologic suppression. = +1.4% (-5.5% to +8.3%) Lower limit of 90% CI: 80 80 Patients Meeting Primary Endpoint /%) 60 60 40 40 Non infériorité Non infériorité Non démontrée 20 20 127 129 102 102 DRV/RTV Mono DRV/RTV + 2 NRTIs DRV/RTV Mono DRV/RTV + 2 NRTIs 1. Clumeck N, et al. JAC Katlama C, et al. AIDS. 2010;24:
 80. Lower limit of 90% CI: Patients Meeting Primary Endpoint /%) Non infériorité. Non démontrée. Non infériorité DRV/RTV Mono. DRV/RTV + 2 NRTIs. DRV/RTV Mono. DRV/RTV + 2 NRTIs. Switch (Intensification With NRTIs) Allowed. ITT Analysis CI, confidence interval; DRV, darunavir; ITT, intent to treat; PP, per protocol; RTV, ritonavir; TLOVR, time to loss of virologic response. The panel on the left of this slide illustrates the results of the MONET trial at 96 weeks. The primary endpoint for MONET was 48 weeks; at that time, the intent-to-treat, time to loss of virologic response analysis showed that darunavir/ritonavir monotherapy was noninferior to darunavir/ritonavir plus 2 NRTIs. However, the 96-week data indicated that monotherapy was not noninferior by the same analysis; almost 75% of the monotherapy patients were undetectable through 96 weeks compared with almost 81% of the patients in the darunavir/ritonavir plus 2 NRTIs arm. Interestingly, there was a larger number of patients with hepatitis C virus (HCV) randomized to the darunavir/ritonavir monotherapy arm (19% vs 12% in the triple combination arm). The investigators hypothesized that adherence might not have been as good among the HCV-coinfected patients. HCV coinfection (and IV drug use) was correlated with the primary endpoint outcome. The diagram at the bottom of this column shows that patients who had documented virologic failure on darunavir/ritonavir monotherapy were able to resuppress HIV-1 RNA with reintensification with NRTIs. When use of this strategy was not counted as virologic failure, the monotherapy arm was noninferior to the triple-therapy arm: 92% of patients in the monotherapy arm and 90.7% of patients on triple therapy suppressed HIV-1 RNA to < 50 copies/mL. Results from the MONOI study of darunavir/ritonavir monotherapy are shown in the right-hand panel of the slide; again there are 2 analyses. One is the per-protocol analysis, which shows that monotherapy was noninferior to triple combination therapy with high rates of success (94% vs 99%, respectively) in maintaining virologic suppression. On the other hand, the intent-to-treat analysis shows that monotherapy was not noninferior: 87.5% of patients in the darunavir/ritonavir monotherapy arm vs 92% of patients in the darunavir/ritonavir plus 2 NRTIs arm achieved virologic suppression. = +1.4% (-5.5% to +8.3%) Lower limit of 90% CI: Patients Meeting Primary Endpoint /%) Non infériorité. Non infériorité. Non démontrée DRV/RTV Mono. DRV/RTV + 2 NRTIs. DRV/RTV Mono. DRV/RTV + 2 NRTIs. 1. Clumeck N, et al. JAC Katlama C, et al. AIDS. 2010;24:")
10
145 Essai PIVOT : résultats à long terme d'un essai de switch vers monothérapie d'IP/r (1) Essai randomisé ouvert conduit dans 43 centres du Royaume Uni Trithérapie Monothérapie IP/r (n = 296) Choix de l’IP laissé au prescripteur *** Poursuite trithérapie (n = 291) Sous trithérapie (avec INNTI ou IP) CV < 50 c/ml depuis > 24 sem. CD4 > 100/mm3 Suivi 5 ans Médiane 44 mois Randomisation 1:1 ** * * Reprise des INTI si CV > 50 c/ml, retour définitif à la trithérapie si échec virologique confirmé (CV > 50 c/ml x 3), toxicité ou souhait du patient ** Retour temporaire à la trithérapie pour grossesse/allaitement ou gestion d'une interaction médicamenteuse pendant une courte durée *** DRV/r : 80 % ; LPV/r : 14 %, autres : 7% PIVOT : Protease Inhibitor monotherapy Versus Ongoing Triple Therapy. Critères de jugement Principal : perte d'options thérapeutiques, définie par l'apparition d'une nouvelle résistance de niveau intermédiaire ou haute à au moins 1 ARV auquel le virus était sensible à l’inclusion Secondaire : survenue de complications graves de la maladie Analyses en ITT, hypothèse de non-infériorité, marge inférieure 10 % Paton N, CROI 2014, Abs. 550LB
 Choix de l’IP laissé au prescripteur *** Poursuite trithérapie (n = 291) Sous trithérapie (avec INNTI ou IP) CV < 50 c/ml depuis > 24 sem. CD4 > 100/mm3. Suivi 5 ans. Médiane 44 mois. Randomisation 1:1. ** * * Reprise des INTI si CV > 50 c/ml, retour définitif à la trithérapie si échec virologique confirmé (CV > 50 c/ml x 3), toxicité ou souhait du patient. ** Retour temporaire à la trithérapie pour grossesse/allaitement ou gestion d une interaction médicamenteuse pendant une courte durée. *** DRV/r : 80 % ; LPV/r : 14 %, autres : 7% PIVOT : Protease Inhibitor monotherapy Versus Ongoing Triple Therapy. Critères de jugement. Principal : perte d options thérapeutiques, définie par l apparition d une nouvelle résistance de niveau intermédiaire ou haute à au moins 1 ARV auquel le virus était sensible à l’inclusion. Secondaire : survenue de complications graves de la maladie. Analyses en ITT, hypothèse de non-infériorité, marge inférieure 10 % Paton N, CROI 2014, Abs. 550LB.")
11
Différence Tri – Mono IP/r
146 Essai PIVOT : résultats à long terme d'un essai de switch vers monothérapie d'IP/r (2) Caractéristiques des patients et résultats entre l’inclusion et la fin du suivi Trithérapie (n = 291) Monothérapie IP/r (n = 296) Différence Tri – Mono IP/r (IC 95 %) p HSH 60 % Blanc 71 % 66 % Femme 22 % 25 % Sérologie VHC+ 7 (2 %) 14 (5 %) CD4 J0 512 ( ) 516 ( ) CD4 nadir 181 (90-258) 170 (80-239) Années depuis début ARV 3,9 (2,0-6,4) 4,2 (2,4-6,9) Nb ARV reçus en tout 5 (3-6) 4 (3-6) IP ou INNTI à J0 IP INNTI 134 (46 %) 127 (54 %) 139 (47 %) 155 (53 %) Rebond CV > 50 c/ml, confirmé, n (%) 8 (3,2 %) 95 (35,0 %) 31,8 % (24,6 à 39,0 %) < 0,001 Perte d'options thérapeutiques à M36, n (%) 2 (0,7 %) 6 (2,1 %) 1,4 (-0,4 à 3,4 %) 0,15 Perte d'options thérapeutiques fin d'essai, n (%) 4 (1,8 %) 0,2 % (-2,5 à 2,6 %) 0,85 Evolution CD4/mm3, moyenne (ET) +91 (9) +108 (9) +17 (-10 à +43) 0,21 Evénements indésirables grade 3/4 % 55 % 46 % -8,4 % (-16,4 à 0,3 %) 0,043 Evolution fonction neuro-cognitives (NPZ-5), moyenne (ET) +0,51 (0,04) +0,50 (0,04) -0,01 (-0,11 à + 0,09) 0,86 Cout des ARV (£), moyenne 30 230 21 260 -8 970 - Les auteurs concluent donc à la non-infériorité de la stratégie de monothérapie d'IP/r sur le critère principal de préservation des options thérapeutiques. Les événements indésirables de grade 3 et 4 sont un peu moins fréquents dans le bras monothérapie. Il a tout de même été observé 35 % de rebonds virologiques chez les patients du bras monothérapie IP/r, avec nécessité de modifier le traitement de façon transitoire ou définitive. 58 % des patients du bras monothérapie restaient en monothérapie à la fin de l’essai. Paton N, CROI 2014, Abs. 550LB
 Caractéristiques des patients et résultats entre l’inclusion et la fin du suivi. Trithérapie. (n = 291) Monothérapie IP/r. (n = 296) Différence Tri – Mono IP/r. (IC 95 %) p. HSH. 60 % Blanc. 71 % 66 % Femme. 22 % 25 % Sérologie VHC+ 7 (2 %) 14 (5 %) CD4 J ( ) 516 ( ) CD4 nadir. 181 (90-258) 170 (80-239) Années depuis début ARV. 3,9 (2,0-6,4) 4,2 (2,4-6,9) Nb ARV reçus en tout. 5 (3-6) 4 (3-6) IP ou INNTI à J0. IP. INNTI. 134 (46 %) 127 (54 %) 139 (47 %) 155 (53 %) Rebond CV > 50 c/ml, confirmé, n (%) 8 (3,2 %) 95 (35,0 %) 31,8 % (24,6 à 39,0 %) < 0,001. Perte d options thérapeutiques à M36, n (%) 2 (0,7 %) 6 (2,1 %) 1,4 (-0,4 à 3,4 %) 0,15. Perte d options thérapeutiques fin d essai, n (%) 4 (1,8 %) 0,2 % (-2,5 à 2,6 %) 0,85. Evolution CD4/mm3, moyenne (ET) +91 (9) +108 (9) +17 (-10 à +43) 0,21. Evénements indésirables grade 3/4 % 55 % 46 % -8,4 % (-16,4 à 0,3 %) 0,043. Evolution fonction neuro-cognitives (NPZ-5), moyenne (ET) +0,51 (0,04) +0,50 (0,04) -0,01 (-0,11 à + 0,09) 0,86. Cout des ARV (£), moyenne Les auteurs concluent donc à la non-infériorité de la stratégie de monothérapie d IP/r sur le critère principal de préservation des options thérapeutiques. Les événements indésirables de grade 3 et 4 sont un peu moins fréquents dans le bras monothérapie. Il a tout de même été observé 35 % de rebonds virologiques chez les patients du bras monothérapie IP/r, avec nécessité de modifier le traitement de façon transitoire ou définitive. 58 % des patients du bras monothérapie restaient en monothérapie à la fin de l’essai. Paton N, CROI 2014, Abs. 550LB.")
12
McKinnon JE et al. AIDS 2006;20:2331-5.

13
MONET: DRV/r does not increase IL-6 or hs-CRP levels
Levels of the inflammatory markers, interleukin-6 (IL-6) and C-reactive protein (CRP), are elevated in HIV-infection. High levels of IL-6 (>3 pg/mL) and CRP (>5 mg/L) have been associated with more rapid progression to AIDS and death1 Marker DRV/r + 2 NRTIs DRV/r monotherapy IL-6 >3 pg/mL 20/65 (31%) 15/64 (23%) hs-CRP > 5 mg/L 8/80 (10%) 9/75 (12%) p=n.s. for both comparisons, chi-square test There was no difference between the treatment arms in IL-6 or hs-CRP levels at the Week 144 visit Rodger A, et al. JID 2009, 200: Arribas JR, et al .EACS, Belgrade, Serbia, October Abstract PS 10/2.
 and C-reactive protein (CRP), are elevated in HIV-infection. High levels of IL-6 (>3 pg/mL) and CRP (>5 mg/L) have been associated with more rapid progression to AIDS and death1. Marker. DRV/r + 2 NRTIs. DRV/r monotherapy. IL-6 >3 pg/mL. 20/65 (31%) 15/64 (23%) hs-CRP > 5 mg/L. 8/80 (10%) 9/75 (12%) p=n.s. for both comparisons, chi-square test. There was no difference between the treatment arms in IL-6 or hs-CRP levels at the Week 144 visit. Rodger A, et al. JID 2009, 200: Arribas JR, et al .EACS, Belgrade, Serbia, October Abstract PS 10/2.")
14
Bithérapie IP/r + 3TC

15
SALT: study design A multicentre, open-label, non-inferiority trial to determine whether 3TC + ATV/r is non-inferior to two NRTIs + ATV/r in HIV-positive patients on a three-drug regimen HIV-1-infected patients on a stable 3-drug regimen. Treatment switch because of toxicity, intolerance, or simplification; no previous treatment failure; no resistance mutations to study medications; HIV-1 RNA < 50 copies/mL for ≥6 months; HBsAg-negative status N = 286 ATV/r + 3TC (n = 143) ATV/r + two NRTIs* (n = 143) Randomisation 1:1 Week 24 Week 48 Week 96 Primary endpoint: Virological response (HIV-1 RNA < 50 copies/mL, TLOVR) at 48 weeks *Control arm nucleosides were selected by the investigator: TDF + FTC (75.6%), ABC + 3TC (23.7%), ZDV + 3TC (0.7%). ABC, abacavir; HBsAg, hepatitis B surface antigen; ZDV, zidovudine. Perez-Molina et al. IAC 2014, Poster LBPE18.
 ATV/r + two NRTIs* (n = 143) Randomisation. 1:1. Week 24. Week 48. Week 96. Primary endpoint: Virological response (HIV-1 RNA < 50 copies/mL, TLOVR) at 48 weeks. *Control arm nucleosides were selected by the investigator: TDF + FTC (75.6%), ABC + 3TC (23.7%), ZDV + 3TC (0.7%). ABC, abacavir; HBsAg, hepatitis B surface antigen; ZDV, zidovudine. Perez-Molina et al. IAC 2014, Poster LBPE18.")
16
SALT: treatment efficacy at 48 weeks
Treatment efficacy was 83.6% for ATV/r + 3TC vs 78.4% for ATV/r + two NRTIs Non-inferiority was demonstrated The results were consistent across the sensitivity analysis 95% CI for the difference Favours ATV/r + two NRTIs Favours ATV/r + 3TC Non-inferiority, Δ = –12% 0% –4.8% 5.2% 15.2% 83.6% 78.4% ATV/r + 3TC + two NRTIs 109/139 112/134 Perez-Molina et al. IAC 2014, Poster LBPE18.

17
SALT: other results at 48 weeks (1)
There were nine virological failures (confirmed as HIV RNA > 50 copies/mL) Five in the ATV/r + 3TC arm vs four in the ATV/r + two NRTIs arm Six could not be amplified because of low VL Only one patient (ATV/r + two NRTIs arm) developed resistance mutations (M184V) No NRTI or PI resistance mutations documented in the ATV/r + 3TC arm Average change in CD4 count from baseline +9.9 cells/μL for ATV/r + 3TC and –9.2 cells/μL for ATV/r + two NRTIs Changes in renal function, bone density and fat gain/distribution were similar between groups Changes in neurocognitive function (GDS; five domains) were not significantly different between the study arms Perez-Molina et al. IAC 2014, Poster LBPE18.
 Five in the ATV/r + 3TC arm vs four in the ATV/r + two NRTIs arm. Six could not be amplified because of low VL. Only one patient (ATV/r + two NRTIs arm) developed resistance mutations (M184V) No NRTI or PI resistance mutations documented in the ATV/r + 3TC arm. Average change in CD4 count from baseline cells/μL for ATV/r + 3TC and –9.2 cells/μL for ATV/r + two NRTIs. Changes in renal function, bone density and fat gain/distribution were similar between groups. Changes in neurocognitive function (GDS; five domains) were not significantly different between the study arms. Perez-Molina et al. IAC 2014, Poster LBPE18.")
18
Investigator-selected NRTIs in FDC*
OLE: Simplification to Dual ART With LPV/RTV + 3TC or FTC in Suppressed Pts Randomized, open-label phase III noninferiority trial Primary endpoint: free of VF at Wk 48 Wk 48 primary analysis Lopinavir/Ritonavir 400/100 mg BID + Lamivudine or Emtricitabine (n = 118) HIV-infected patients with HIV-1 RNA < 50 c/mL; on triple ART with LPV/RTV + 3TC or FTC + NRTI for 6 mos; no resistance to LPV/RTV or 3TC or FTC (N = 239) For more information about this study, go online to Lopinavir/Ritonavir 400/100 mg BID + Lamivudine or Emtricitabine + Investigator-selected NRTIs in FDC* (n = 121) *TDF/FTC: 60%; ABC/3TC: 28%; Other: 12% Gatell J, et al. AIDS Abstract LBPE17.
 HIV-infected patients with HIV-1 RNA < 50 c/mL; on triple ART with LPV/RTV + 3TC or FTC + NRTI for 6 mos; no resistance to LPV/RTV or 3TC or FTC (N = 239) For more information about this study, go online to Lopinavir/Ritonavir 400/100 mg BID + Lamivudine or Emtricitabine + Investigator-selected NRTIs in FDC* (n = 121) *TDF/FTC: 60%; ABC/3TC: 28%; Other: 12% Gatell J, et al. AIDS Abstract LBPE17.")
19
Therapeutic Response*
OLE: Switching Suppressed Pts to Dual ART Noninferior to Triple ART at Wk 48 Δ -0.6% (95% CI: -6.9% to 8.1%) New grade 3/4 AEs in 9 pts in each arm Significantly greater increases in TC (P = .02), numerically greater increases in TG (P = .09) in dual-ART arm Numerically greater decreases in creatinine in triple-ART arm New lab abnormalities similar VF in 3 pts in each arm 1 pt (dual-ART) tested for resistance; had K103N and M184V SALT trial of switches in suppressed pts showed switch to ATV/RTV + 3TC noninferior to switch to ATV/RTV NRTIs[2] 100 91.5 90.9 Dual ART (n = 118) Triple ART (n = 121) 80 60 Patients (%)[1] 40 mITT, modified intent-to-treat; TC, total cholesterol; TG., triglycerides 20 3.3 5.1 2.5 2.5 3.3 0.8 n = Therapeutic Response* VF D/C Due to AE D/C for Other Reasons *HIV-1 RNA < 50 c/mL at Wk 48 (mITT). 1. Gatell J, et al. AIDS Abstract LBPE17. Graphic used with permission. 2. Perez-Molina JA, et al. AIDS Abstract LBPE18.
 New grade 3/4 AEs in 9 pts in each arm. Significantly greater increases in TC (P = .02), numerically greater increases in TG (P = .09) in dual-ART arm. Numerically greater decreases in creatinine in triple-ART arm. New lab abnormalities similar. VF in 3 pts in each arm. 1 pt (dual-ART) tested for resistance; had K103N and M184V. SALT trial of switches in suppressed pts showed switch to ATV/RTV + 3TC noninferior to switch to ATV/RTV + 2 NRTIs[2] Dual ART (n = 118) Triple ART (n = 121) Patients (%)[1] 40. mITT, modified intent-to-treat; TC, total cholesterol; TG., triglycerides n = Therapeutic Response* VF. D/C Due to AE. D/C for Other Reasons. *HIV-1 RNA < 50 c/mL at Wk 48 (mITT). 1. Gatell J, et al. AIDS Abstract LBPE17. Graphic used with permission. 2. Perez-Molina JA, et al. AIDS Abstract LBPE18.")
20
Cas n2 Mr M 55 ans Infection à VIH depuis 12 ans (primo inf)
Génotype initial: K103N Nadir de CD4 400 par mm3 Observant Conduite sexuelle à risque Traitement initial : TDF+FTC+LPV/r puis DRV/r Indétectable Dyslipidémie modérée Fumeur Souhaite une simplification thérapeutique et est demandeur d’un STR

21
Que lui proposer vous ? Pas de changement de traitement Un STR : Eviplera Un STR : Stribild 2 INTI + Anti intégrase 2 INTI + IP non boosté Autres options thérapeutiques

23
Nombre de comprimés associé à une moins bonne adhérence et moins bonne reponse
virologique dans les regimes OAD et BID Adherence supérieure dans les regimes OAD Ps de difference de suppression virologique Un bon niveau d adherence persiste plus longtemps en OAD

26
Quels switch avec bénéfice sur les lipides ? (LDL C ou ratio)
")
27
SPIRAL: Switch to RAL Noninferior to Maintaining PI/RTV Regimens
Patients With VF RAL (n = 4) PI/RTV (n = 6) Prior VF 1 3 Prior suboptimal ART 2 Prior resistance mutations 5 Resistance test at VF 4 Mutations 3 (PR, RT) Free of Treatment Failure at Wk 48 (ITT, S = F) Patients (%) 100 89.2 86.6 80 60 40 Mean Change From Baseline to Wk 48, % Switch to RAL Continue PI/RTV P Value Triglycerides -22.1 +4.7 < .0001 TC -11.2 +1.8 LDL-C -6.5 +3.0 < .001 HDL-C -3.2 +5.8 Total to HDL-C ratio -4.9 -1.3 < .05 20 Switch to RAL Continue PI/RTV Martinez E, et al. AIDS. 2010;24:
 PI/RTV (n = 6) Prior VF Prior suboptimal ART. 2. Prior resistance mutations. 5. Resistance test at VF. 4. Mutations. 3 (PR, RT) Free of Treatment Failure at Wk 48 (ITT, S = F) Patients (%) Mean Change From Baseline to Wk 48, % Switch to RAL. Continue PI/RTV. P Value. Triglycerides < TC LDL-C < HDL-C Total to HDL-C ratio < Switch to RAL. Continue PI/RTV. Martinez E, et al. AIDS. 2010;24:")
28
SPIRIT Changes from Baseline in Fasting Lipids
TC LDL TG HDL .03 (3) (-1) (-1) (-2) (-2) -.03 (-4) -0.1 -0.03 -0.05 -0.05 -0.1 -0.2 0.1 .08 -0.3 (-14) (-16) (-16) Mean Changes from BL, mmol/L (mg/dL) -0.4 -.36 -.41 -0.41 - -0.5 -0.1 (-53) (-24) -0.6 (-25) (-25) Change in TC:HDL ratio -.62 -.60 -0.2 -0.7 (-64) -.65 -.65 -0.21 -0.27 RPV/FTC/TDF (immediate, D1-W24) PI+RTV+2NRTIs (D1-W24) RPV/FTC/TDF (delayed, W24-W48) RPV/FTC/TDF (immediate, D1-W48) -.72 -0.3 -0.8 -0.35 (-80) -0.9 -.90 -0.4 Switching to RPV/FTC/TDF resulted in improvement in fasting lipids, including TC, LDL, TGs, and TC:HDL ratio at Week 24 and maintained through Week 48 TC - total cholesterol, LDL - low-density lipoprotein, TG - triglycerides, HDL - high-density lipoprotein
 (-1) (-1) (-2) (-2) (-4) (-14) (-16) (-16) Mean Changes from BL, mmol/L (mg/dL) (-53) (-24) (-25) (-25) Change in TC:HDL ratio (-64) RPV/FTC/TDF (immediate, D1-W24) PI+RTV+2NRTIs (D1-W24) RPV/FTC/TDF (delayed, W24-W48) RPV/FTC/TDF (immediate, D1-W48) (-80) Switching to RPV/FTC/TDF resulted in improvement in fasting lipids, including TC, LDL, TGs, and TC:HDL ratio at Week 24 and maintained through Week 48. TC - total cholesterol, LDL - low-density lipoprotein, TG - triglycerides, HDL - high-density lipoprotein.")
29
TDF/FTC/EVG/c (Stribild®) S48 Evaluation principale
126 Essai STRATEGY-PI : simplification par TDF/FTC/EVG/c d’une trithérapie par TDF/FTC + IP/r Résultats à S48 (1) 433 patients VIH+ sous TDF/FTC + IP/r avec CV < 50 c/ml depuis au moins 6 mois en 1er ou 2ème régime ARV sans historique d’échec virologique et sans résistance à TDF ou FTC dans historique génotypique DFGeCG > 70 ml/min TDF/FTC/EVG/c (Stribild®) 2:1 (n = 140) TDF/FTC + IP/r (n = 293) S96 S48 Evaluation principale Essai international, randomisé, ouvert Critère principal : proportion de patients avec maintien d’une CV < 50 c/ml à S48 Analyse FDA snapshot, borne de non infériorité : 12 % Si la non infériorité est établie, un test de supériorité est prévu dans le protocole Questionnaires de qualité de vie et symptômes Analyse génotypique pour les patients avec un rebond (2 visites consécutives avec CV > 50 c/ml et la seconde > 400 c/ml ou une seule CV > 400 c/ml à S48 ou à dernière visite) Arribas J, CROI 2014, Abs. 551LB
 433 patients VIH+ sous TDF/FTC + IP/r avec CV < 50 c/ml depuis au moins 6 mois. en 1er ou 2ème régime ARV. sans historique d’échec virologique et sans résistance à TDF ou FTC dans historique génotypique. DFGeCG > 70 ml/min. TDF/FTC/EVG/c (Stribild®) 2:1. (n = 140) TDF/FTC + IP/r. (n = 293) S96. S48 Evaluation principale. Essai international, randomisé, ouvert. Critère principal : proportion de patients avec maintien d’une CV < 50 c/ml à S48 Analyse FDA snapshot, borne de non infériorité : 12 % Si la non infériorité est établie, un test de supériorité est prévu dans le protocole. Questionnaires de qualité de vie et symptômes. Analyse génotypique pour les patients avec un rebond (2 visites consécutives avec CV > 50 c/ml et la seconde > 400 c/ml ou une seule CV > 400 c/ml à S48 ou à dernière visite) Arribas J, CROI 2014, Abs. 551LB.")
30
Evolution des lipides (à jeun) entre inclusion et S48
134 Essai STRATEGY-PI : simplification par TDF/FTC/EVG/c d’une trithérapie par TDF/FTC + IP/r Résultats à S48 (9) Evolution des lipides (à jeun) entre inclusion et S48 TDF/FTC/EVG/c TDF/FTC + IP/r Tous patients Patients sous LPV/r au screening Valeurs médianes à J0 (mg/dl) p = 0,86 p = 0,81 p = 0,001 p = 0,31 - 16 1 3 60 50 40 30 20 10 (mg/dl) Chol-T LDL-c TG HDL-c p = 0,002 p = 0,16 p = 0,003 p = 0,016 - 25 13 46 2 1 9 5 60 50 40 30 20 10 (mg/dl) Chol-T LDL-c TG HDL-c Dans les sous-groupes de patients sous ATV/r et DRV/r des différences significatives sont observées pour : Triglycérides pour ATV/r : - 12 (TDF/FTC/EVG/c) vs + 15 mg/dl (p = 0,01) HDL-c pour DRV/r : + 3 (TDF/FTC/EVG/c) vs 0 mg/dl (p = 0,03) Arribas J, CROI 2014, Abs. 551LB
 Evolution des lipides (à jeun) entre inclusion et S48. TDF/FTC/EVG/c. TDF/FTC + IP/r. Tous patients. Patients sous LPV/r au screening Valeurs médianes à J0 (mg/dl) p = 0,86. p = 0,81. p = 0,001. p = 0, (mg/dl) Chol-T LDL-c TG HDL-c p = 0,002. p = 0,16. p = 0,003. p = 0, (mg/dl) Chol-T LDL-c TG HDL-c. Dans les sous-groupes de patients sous ATV/r et DRV/r des différences significatives sont observées pour : Triglycérides pour ATV/r : - 12 (TDF/FTC/EVG/c) vs + 15 mg/dl (p = 0,01) HDL-c pour DRV/r : + 3 (TDF/FTC/EVG/c) vs 0 mg/dl (p = 0,03) Arribas J, CROI 2014, Abs. 551LB.")
32
Cas n 3 Mr B 40 ans Découverte du VIH en 2003 CD4 400/mm3
Charge virale copies/ml Sans traitement jusqu’en 06/2006 ( réticence) A cette époque CD4= 280 , CV = 2800 copies/ml Instauration d’un traitement par TDF+ATZ/r
 A cette époque CD4= 280 , CV = 2800 copies/ml. Instauration d’un traitement par TDF+ATZ/r.")
33
Cas n3 Rapidement indétectable (M3) Augmentation des CD4 ( 400)
Hyperbilirubinémie avec ictère conjonctival Bilirubine totale fluctuente entre 50 et 90 En Juin 2007 , souhaite adaptation thérapeutique Que proposez vous ?

34
Cas N3 « deboost » Nette diminution de la bilirubine Entre 30 et 50
Est resté indétectable Toujours sous tt en 2014

35
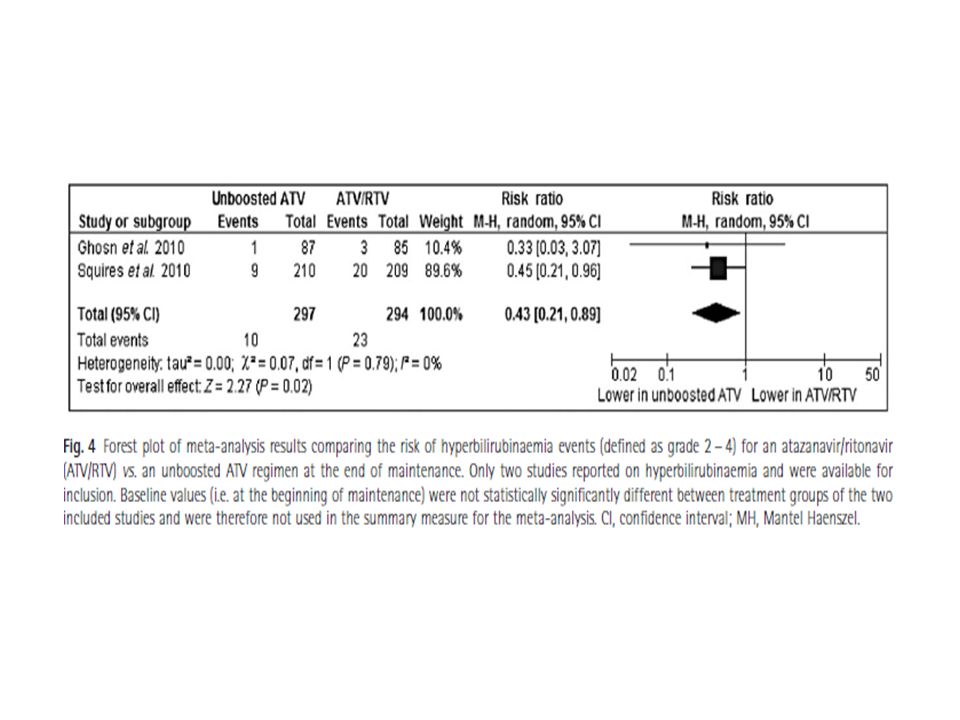
ARIES: Boosted vs Unboosted ATV Maintenance in Naive Pts
Wk 36 randomization if HIV-1 RNA < 50 c/mL* Wk 84 primary endpoint ATV 400 mg QD + ABC/3TC FDC (n = 210) Antiretroviral-naive pts with HIV-1 RNA ≥ 1000 c/mL; no CD4+ cell count restrictions; HLA-B*5701 negative (N = 515) ATV/RTV 300/100 mg QD + ABC/3TC FDC (n = 515) Wk 144 For more information about this study, go online to: ATV/RTV 300/100 mg QD + ABC/3TC FDC (n = 209) *Stratified by BL HIV-1 RNA < or ≥ 100,000 c/mL Squires K, et al. IAS Abstract WELBB103. 35 35
 Antiretroviral-naive pts with HIV-1 RNA ≥ 1000 c/mL; no CD4+ cell count restrictions; HLA-B*5701 negative. (N = 515) ATV/RTV 300/100 mg QD + ABC/3TC FDC. (n = 515) Wk 144. For more information about this study, go online to: ATV/RTV 300/100 mg QD. + ABC/3TC FDC. (n = 209) *Stratified by BL HIV-1 RNA < or ≥ 100,000 c/mL. Squires K, et al. IAS Abstract WELBB")
36
ARIES: Boosted vs Unboosted ATV Maintenance: Wk 84 Results
ATV (n = 210) 100 ATV/RTV (n = 209) 86 85 87 80.8 82 79 80 60 HIV-1 RNA < 50 c/mL at Wk 84 (%) 40 20 Overall Results BL HIV-1 RNA < 100,000 c/mL BL HIV-1 RNA ≥ 100,000 c/mL Squires K, et al. IAS Abstract WELBB103. Graphic used with permission. 36
 100. ATV/RTV (n = 209) HIV-1 RNA < 50 c/mL at Wk 84 (%) Overall Results. BL HIV-1 RNA < 100,000 c/mL. BL HIV-1 RNA ≥ 100,000 c/mL. Squires K, et al. IAS Abstract WELBB103. Graphic used with permission. 36.")
37
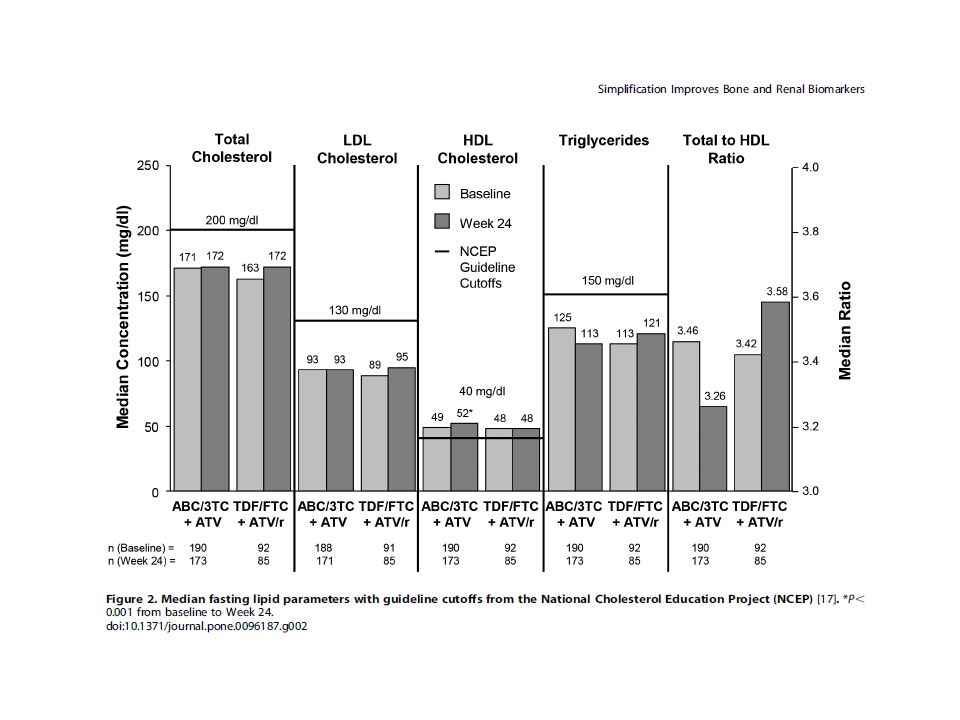
ARIES: Boosted vs Unboosted ATV Maintenance: Lipids and Safety
ATV (n = 210) NCEP Guidelines TC 200 mg/dL 200 ATV/RTV (n = 209) TG 150 mg/dL 160 LDL 130 mg/dL 120 Median Concentration (mg/dL) 80 HDL 40 mg/dL 40 BL Wk 36 Wk 84 BL Wk 36 Wk 84 BL Wk 36 Wk 84 BL Wk 36 Wk 84 Lipid-lowering medication usage: ATV 13% vs ATV/RTV 16% through 84 wks Grade 2-4 hyperbilirubinemia higher in ATV/RTV arm vs ATV arm: 10% vs 4% No MIs at Wk 84 Squires K, et al. IAS Abstract WELBB103. Graphic used with permission. 37
 NCEP Guidelines. TC 200 mg/dL ATV/RTV (n = 209) TG 150 mg/dL LDL 130 mg/dL Median Concentration (mg/dL) 80. HDL 40 mg/dL. 40. BL. Wk 36. Wk 84. BL. Wk 36. Wk 84. BL. Wk 36. Wk 84. BL. Wk 36. Wk 84. Lipid-lowering medication usage: ATV 13% vs ATV/RTV 16% through 84 wks. Grade 2-4 hyperbilirubinemia higher in ATV/RTV arm vs ATV arm: 10% vs 4% No MIs at Wk 84. Squires K, et al. IAS Abstract WELBB103. Graphic used with permission. 37.")
42
NEAT: risk factors for VF in 886 patients receiving unboosted ATV
Variable Univariate analysis Multivariate analysis HR (95% CI) p Female gender Age ≥ 45 years CDC classification 2-3 HCV co-infection Nadir CD4 count < 200 cells/mm3 Peak of HIV viral load > 105 copies/mL Virological failure on PI Virological failure on NRTI Virological failure on NNRTI CD4 cell count < 400 cells/mm3 at switch Switch for simplification ART with PI before the switch 1.37 ( ) 1.00 ( ) 1.45 ( ) 1.30 ( ) 1.36 ( ) 0.89 ( ) 2.48 ( ) 2.14 ( ) 1.44 ( ) 1.11 ( ) 1.23 ( ) 1.67 ( ) 0.080 > 0.99 0.13 0.14 0.078 0.5 < 0.0005 0.12 0.57 0.23 0.039 2.04 ( ) 1.63 ( ) 0.006 0.049 NRTIs associated with atazanavir ABC AZT TDF ddI 0.82 ( ) 0.85 ( ) 1.22 ( ) 1.33 ( ) 0.26 0.52 0.25 0.24 Pavie et al. J Antimicrob Chemother 66:2372−8. Unboosted ATV is not approved for use in Europe 42 42
 p. Female gender. Age ≥ 45 years. CDC classification 2-3. HCV co-infection. Nadir CD4 count < 200 cells/mm3. Peak of HIV viral load > 105 copies/mL. Virological failure on PI. Virological failure on NRTI. Virological failure on NNRTI. CD4 cell count < 400 cells/mm3 at switch. Switch for simplification. ART with PI before the switch ( ) 1.00 ( ) 1.45 ( ) 1.30 ( ) 1.36 ( ) 0.89 ( ) 2.48 ( ) 2.14 ( ) 1.44 ( ) 1.11 ( ) 1.23 ( ) 1.67 ( ) > < ( ) 1.63 ( ) NRTIs associated with atazanavir. ABC. AZT. TDF. ddI ( ) 0.85 ( ) 1.22 ( ) 1.33 ( ) Pavie et al. J Antimicrob Chemother 66:2372−8. Unboosted ATV is not approved for use in Europe")
43
Cas N3 Depuis 6 mois dégradation de la fonction rénale
Creat a 110Mmol/l ( 75 en 2003) clearance a 78 ( 150 en 2003) Que faites vous ?
 clearance a 78 ( 150 en 2003) Que faites vous")
44
Cas 3 Pas d’autres médicaments néphrotoxique Bilan néphro
Pas de protéinurie Phosphoremie 0,8 Bandelette U nl Pas de glycosurie Que faites vous ?

45
CAS 2 Ce qui a été proposé Kivexa Reyataz après HLA B5701

46
Protocol-specified HAARTa
ASSURE Study Design Open-label, multicenter, non-inferiority study of subjects with confirmed HIV RNA <75 c/mL All subjects had ≥6 months’ treatment with TDF/FTC + ATV/r as last regimen Primary endpoint: proportion of subjects with HIV RNA <50 c/mL at Week 24 by the time to loss of virologic response (TLOVR) algorithm 2:1 Randomization ABC/3TC + ATV n=199 Protocol-specified HAARTa TDF/FTC + ATV/r N=296 ASSURE is an open-label, multicenter, non-inferiority study of subjects with confirmed HIV RNA <75 c/mL, ≥ 6 months’ treatment with TDF/FTC +ATV/r as last regimen and eCrCL ≥50 mL/min. Subjects were randomized 2:1 to initiate ABC/3TC + ATV or continue TDF/FTC + ATV/r. The primary endpoint was % with HIV RNA <50 c/mL at Wk 24 by the Time to Loss Of Virologic Response (TLOVR) algorithm. TDF/FTC + ATV/r n=97 ART naive ≥6 months 24 48 Weeks a First or second regimen switch allowed for any reason EXCEPT virologic failure. Wohl D, et al ICAAC 2012
 algorithm. 2:1 Randomization. ABC/3TC + ATV. n=199. Protocol-specified HAARTa. TDF/FTC + ATV/r. N=296. ASSURE is an open-label, multicenter, non-inferiority study of subjects with confirmed HIV RNA <75 c/mL, ≥ 6 months’ treatment with TDF/FTC +ATV/r as last regimen and eCrCL ≥50 mL/min. Subjects were randomized 2:1 to initiate ABC/3TC + ATV or continue TDF/FTC + ATV/r. The primary endpoint was % with HIV RNA <50 c/mL at Wk 24 by the Time to Loss Of Virologic Response (TLOVR) algorithm. TDF/FTC + ATV/r. n=97. ART naive. ≥6 months Weeks. a First or second regimen switch allowed for any reason EXCEPT virologic failure. Wohl D, et al ICAAC")
47
Primary Analysis: Proportion with HIV-1 RNA <50 c/mL by TLOVR
ABC/3TC + ATV is non-inferior to TDF/FTC + ATV/r based on a 12% margin Adjusted treatment difference: % 95% CI: (-7.97%, 8.64%) Wohl D, et al ICAAC 2012
 Wohl D, et al ICAAC")
51
Simplification Thérapeutique (2)
VIROSEM 2014 Simplification Thérapeutique (2) Jean Luc Meynard, St Antoine, Paris Pierre de Truchis, Garches
 Jean Luc Meynard, St Antoine, Paris. Pierre de Truchis, Garches.")
52
Me GF, 42 ans Née 1972, AVP 1985: paraplégie complète T12-L1
Transfusion, infection VIH diagnostiquée en 1989 Antécédents: Vessie neurologique, autosondages, infections urinaires, pyélonéphrites, colonisation E.Coli; entérocystoplastie 2002. Cholecystectomie Phlebite 1994 Capsulite bilatérale des épaules Dorsalgies / « Charcot-spine » 2009 Colopathie « fonctionnelle » Affections liées au VIH: Zona Pneumopathies bactériennes Candidose récurrente Statut immunovirologique: Traitement ARV en 1993: AZT+ddI Nadir CD4: 160

53
Me GF, 42 ans dates ARV CV CD4 1993 AZT+ddI puis 3TC - 172 5/07/96 d4T+3TC+IDV 4400 161 11/07/97 : <200 235 22/12/98 ABC+3TC+r/IDV 890 192 10/11/99 7190 309 23/12/09 3TC+ddI+r/LPV 51200 201 29/11/01 907 433 17/07/03 17200 320 17/03/04 TDF+ddI+EFV+rLPV 5700 197 6/09/05 TDF+ddI+r/fAPV 8920 23/12/05 AZT+FTC+TDF+rTPV+T20 18500 216 29/11/06 : (stop T20) <50 374 2/06/08 AZT+TDF+FTC+rDRV <40 523 20/09/10 <20 525 Génotypes:1999: RT = 184V PRO = 10I, 46I, 63P, 88D 2005: RT= 74LV,70KE, 90I,100I,103R,179D PRO: 20M 36I 41K 46I 54L 62V 63P 82A 88D 90M
 < /06/08. AZT+TDF+FTC+rDRV. < /09/10. < Génotypes:1999: RT = 184V PRO = 10I, 46I, 63P, 88D. 2005: RT= 74LV,70KE, 90I,100I,103R,179D PRO: 20M 36I 41K 46I 54L 62V 63P 82A 88D 90M.")
54
Me GF, 42 ans: 2010 Complications urinaires et ostéo-articulaires de la paraplégie Traitement ARV: AZT+Truvada+RTV100/DRV600 x2/j CD4= 462 (30%), CV<20 Troubles digestifs, ballonnements, diarrhées récurrentes Difficultés de prises des ARV, prises manquées, interruptions de quelques jours répétées
, CV<20. Troubles digestifs, ballonnements, diarrhées récurrentes. Difficultés de prises des ARV, prises manquées, interruptions de quelques jours répétées.")
55
Me GF, 42 ans: 2010 Que proposez vous concernant le Tt ARV:
Consultation ETP Dosage plasmatique des ARV Simplification thérapeutique avec réduction/suppression des nucléosidiques Monothérapie r/DRV Combinaison Etravirine + Raltégravir Combinaison IP+Raltégravir

56
Etudes de switch chez patients en succès
essai Tt référence Seuil efficacité suivi % succès ATAZIP 2nuc+rLPV <200 S48 85,8% SWEET AZT+3TC+EFV <50 84% OK04 90% Mills TDF+FTC+rLPV 91,4% Alize 2nuc+IP <400 87,6% Monet 2nucs+rDRV 85,3% SWAN 2nucs+IP 66% SLOAT 2nucs+rLPV 88,5% AI266273 tritherapie - MONOI 92% SPIRAL 86,6% SWIFT ABC+3TC+IP 83,3% ARIES ABC+3TC+rATV 81% STARTMRK 2nuc+EFV 87% RAL+ETV 50 SPIRIT 2IN + IP S24 89,9%

57
Me GF, 42 ans: 2010 Évaluation SSR
Tentative de prise en charge psychothérapie de soutien Dosage plasmatique des ARV: RTV= 670 ng/ml DRV (C12h)= 4977 ng/ml Suppression AZT Passage prise unique quotidienne: Truvada + RTV100/ DRV800 x1/j
= 4977 ng/ml. Suppression AZT. Passage prise unique quotidienne: Truvada + RTV100/ DRV800 x1/j.")
58
Me GF, 42 ans: 2012 Traitement ARV: Truvada +R/DRV 800
Effets secondaires persistants: épisodes diarrhées et ballonnements, sensation de malaise, asthénie Biologie: CD4=590 (33%), CV<20 Créatinine 110μM/l, Phosphore: 0,69mM/l MDRD 70ml/mn protéinurie 0,55g/l, Albuminurie: 180mg/l Dosage des ARV: TDF (C22h): 115 ng/ml RTV (C22h): 230 ng/ml, DRV (C22h): 3169 ng/ml
, CV<20. Créatinine 110μM/l, Phosphore: 0,69mM/l. MDRD 70ml/mn. protéinurie 0,55g/l, Albuminurie: 180mg/l. Dosage des ARV: TDF (C22h): 115 ng/ml. RTV (C22h): 230 ng/ml, DRV (C22h): 3169 ng/ml.")
59
Me GF, 42 ans: 2012 Que proposez vous concernant le Tt ARV:
Poursuite Tt inchangé Réduction posologie des ARV (IP,TDF) Monothérapie r/DRV Bithérapie avec r/DRV Combinaison Etravirine + Raltégravir Combinaison IP+Raltégravir
 Monothérapie r/DRV. Bithérapie avec r/DRV. Combinaison Etravirine + Raltégravir. Combinaison IP+Raltégravir.")
60
Me GF, 42 ans: 2012 Que proposez vous concernant le Tt ARV:
Poursuite Tt inchangé Réduction posologie des ARV (IP,TDF) Monothérapie r/DRV Bithérapie avec r/DRV Combinaison Etravirine + Raltégravir Combinaison IP+Raltégravir
 Monothérapie r/DRV. Bithérapie avec r/DRV. Combinaison Etravirine + Raltégravir. Combinaison IP+Raltégravir.")
61
Canadian HIV Treatment Cohort Study: Durability of First ART Regimen
Retrospective, observational study (n=2965) Initiate ART EFV/FTC/TDF (single-tablet regimen) Raltegravir, darunavir/r, or atazanavir/r NRTIs Primary endpoint Any change/break in first ART regimen for >30 days Median follow-up: 2.5 years Discontinuation of first regimen: 49% Adjusted hazard ratio for discontinuation (reference: EFV/FTC/TDF) Atazanavir/r + 2 NRTIs: 1.16 (P=0.01) Raltegravir + 2 NRTIs: 0.58 (P=0.06) First ART Discontinuation Probability of Treatment Discontinuation Slide: Canadian HIV Treatment Cohort Study: Durability of First ART Regimen Machouf and colleagues conducted a retrospective, observational study in 2965 HIV-infected patients starting ART ( ) to compare the duration of first-line single-tablet regimens (STRs) to other recommended first-line therapies (non-STRs).1 EFV/FTC/TDF (single-tablet regimen). Raltegravir, darunavir/r, or atazanavir/r + 2 NRTIs. The primary endpoint was any change/break in first ART regimen for >30 days.1 The median follow-up was 2.5 years. Approximately half of the patients discontinued the first regimen. Compared with the STR arm, patients in the atazanavir/r-based arm were more likely to discontinue ART whereas patients in the raltegravir arm were less likely.1 Reference Machouf N, Szadkowski L, Trottier B, et al. Do single tablet regimens translate into more durable HIV treatments? Evidence from the Canadian observational cohort (CANOC). Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract WEPDB0103. EVF/FTC/TDF (n=1420) Raltegravir + 2 NRTIs (n=87) Darunavir/r + 2 NRTIs (n=214) Atazanavir/r + 2 NRTIs (n=1244) Time (months) Machouf N, et al. 20th IAC. Melbourne, Abstract WEPDB0103.
 Initiate ART EFV/FTC/TDF (single-tablet regimen) Raltegravir, darunavir/r, or atazanavir/r + 2 NRTIs. Primary endpoint. Any change/break in first ART regimen for >30 days. Median follow-up: 2.5 years. Discontinuation of first regimen: 49% Adjusted hazard ratio for discontinuation (reference: EFV/FTC/TDF) Atazanavir/r + 2 NRTIs: 1.16 (P=0.01) Raltegravir + 2 NRTIs: 0.58 (P=0.06) First ART Discontinuation. Probability of Treatment Discontinuation. Slide: Canadian HIV Treatment Cohort Study: Durability of First ART Regimen. Machouf and colleagues conducted a retrospective, observational study in 2965 HIV-infected patients starting ART ( ) to compare the duration of first-line single-tablet regimens (STRs) to other recommended first-line therapies (non-STRs).1. EFV/FTC/TDF (single-tablet regimen). Raltegravir, darunavir/r, or atazanavir/r + 2 NRTIs. The primary endpoint was any change/break in first ART regimen for >30 days.1. The median follow-up was 2.5 years. Approximately half of the patients discontinued the first regimen. Compared with the STR arm, patients in the atazanavir/r-based arm were more likely to discontinue ART whereas patients in the raltegravir arm were less likely.1. Reference. Machouf N, Szadkowski L, Trottier B, et al. Do single tablet regimens translate into more durable HIV treatments Evidence from the Canadian observational cohort (CANOC). Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract WEPDB0103. EVF/FTC/TDF (n=1420) Raltegravir + 2 NRTIs (n=87) Darunavir/r + 2 NRTIs (n=214) Atazanavir/r + 2 NRTIs (n=1244) Time (months) Machouf N, et al. 20th IAC. Melbourne, Abstract WEPDB0103.")
63
Un STR en 1ère ligne est-il associé à une meilleure durabilité et efficacité ? (2)
Probabilité de rester sous le 1er traitement Prédicteurs d'arrêt du 1er traitement (modèle ajusté) RAL ATV DRV ATR 1,0 0,8 0,6 0,4 0,0 1 2 3 4 5 6 Années p = 0,039 HR (IC 95 %) Année initiation 1,21 (1,06 - 1,38) UDIV 2,14 (1,18 - 3,86) CV > c/ml 1,40 (1,03 - 1,91) 3è agent EFV (ATR) RAL ATV DRV Référence 0,36 (0,18 - 0,72) 1,21 (0,80 - 1,81) 0,99 (0,62 - 1,59) Probabilité de maintien du succès virologique Prédicteurs de perte de réponse virologique (modèle ajusté) La principale cause d’arrêt de 1ère ligne est la survenue d’effets indésirables (55 % des raisons d’arrêts). RAL ATV DRV ATR 1,0 0,8 0,6 0,4 0,0 1 2 3 4 5 6 Années p = 0,015 HR (IC 95 %) Année initiation 1,12 (0, ,32) UDIV 2,57 (1,31 - 5,09) CV > c/ml 1,40 (0,92 - 2,15) 3è agent EFV (ATR) RAL ATV DRV Référence 1,04 (0,45 - 2,37) 2,28 (1,27 - 4,12) 2,09 (1,09 - 3,99) Trottier B, IAS 2013, Abs. TUPDB0106
 RAL. ATV. DRV. ATR. 1,0. 0,8. 0,6. 0,4. 0, Années. p = 0,039. HR (IC 95 %) Année initiation. 1,21 (1,06 - 1,38) UDIV. 2,14 (1,18 - 3,86) CV > c/ml. 1,40 (1,03 - 1,91) 3è agent EFV (ATR) RAL. ATV. DRV. Référence 0,36 (0,18 - 0,72) 1,21 (0,80 - 1,81) 0,99 (0,62 - 1,59) Probabilité de maintien du succès virologique. Prédicteurs de perte de réponse virologique. (modèle ajusté) La principale cause d’arrêt de 1ère ligne est la survenue d’effets indésirables (55 % des raisons d’arrêts). RAL. ATV. DRV. ATR. 1,0. 0,8. 0,6. 0,4. 0, Années. p = 0,015. HR (IC 95 %) Année initiation. 1,12 (0,95 - 1,32) UDIV. 2,57 (1,31 - 5,09) CV > c/ml. 1,40 (0,92 - 2,15) 3è agent EFV (ATR) RAL. ATV. DRV. Référence 1,04 (0,45 - 2,37) 2,28 (1,27 - 4,12) 2,09 (1,09 - 3,99) Trottier B, IAS 2013, Abs. TUPDB0106.")
64
CANOC Cohort: Risk of Virologic Failure in Patients Who Switch First ART for Reasons Other Than Virologic Failure Canadian cohort study (n=2807) Initiate first ART 1/2005 through 6/2012 HIV RNA <50 copies/mL Subsequent ART switch (36%) Once: 14% >2 times: 22% ART switching was associated with Longer duration of ART Subsequent virologic failure Female gender Provincial location ART switching for “tolerability” Might represent specific patient characteristics where ART intolerance is a marker for factors associated with poor adherence versus specific ART concerns Adjusted Odds Ratio for Regimen Switch and Risk of Virologic Failure (HIV RNA >1000 copies/mL) Adjusted OR (95% CI) Regimen switch 1.35 ( ) P<0.001 Male gender 0.35 ( ) IDU 2.85 ( ) Slide: CANOC Cohort: Risk of Virologic Failure in Patients Who Switch First ART for Reasons Other Than Virologic Failure In a Canadian cohort study, Hull and colleagues evaluated factors associated with regimen switch for non-virologic failure and the association between switching and subsequent virologic failure among 2807 HIV-infected persons who initiated first ART (1/2005-6/2012). Patients had to be HIV RNA <50 copies/mL with ART.1 Subsequent ART switch (36%): once: 14%; >2 times: 22%. ART switching was associated with a longer duration of ART, subsequent virologic failure, female gender, and Provincial location in canada.1 ART switching for “tolerability” might represent specific patient characteristics where ART intolerance is a marker for factors associated with poor adherence versus specific ART concerns.1 Reference Hull M, Cescon A, Raboud J, et al. Switching from first antiretroviral therapy regimen while virologically suppressed is associated with increased risk of subsequent virologic failure. Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract TUAB0103. Hull M, et al. 20th IAC. Melbourne, Abstract TUAB0103.
 Initiate first ART 1/2005 through 6/2012. HIV RNA <50 copies/mL. Subsequent ART switch (36%) Once: 14% >2 times: 22% ART switching was associated with. Longer duration of ART. Subsequent virologic failure. Female gender. Provincial location. ART switching for tolerability Might represent specific patient characteristics where ART intolerance is a marker for factors associated with poor adherence versus specific ART concerns. Adjusted Odds Ratio for Regimen Switch and. Risk of Virologic Failure. (HIV RNA >1000 copies/mL) Adjusted OR. (95% CI) Regimen switch ( ) P< Male gender ( ) IDU ( ) Slide: CANOC Cohort: Risk of Virologic Failure in Patients Who Switch First ART for Reasons Other Than Virologic Failure. In a Canadian cohort study, Hull and colleagues evaluated factors associated with regimen switch for non-virologic failure and the association between switching and subsequent virologic failure among 2807 HIV-infected persons who initiated first ART (1/2005-6/2012). Patients had to be HIV RNA <50 copies/mL with ART.1. Subsequent ART switch (36%): once: 14%; >2 times: 22%. ART switching was associated with a longer duration of ART, subsequent virologic failure, female gender, and Provincial location in canada.1. ART switching for tolerability might represent specific patient characteristics where ART intolerance is a marker for factors associated with poor adherence versus specific ART concerns.1. Reference. Hull M, Cescon A, Raboud J, et al. Switching from first antiretroviral therapy regimen while virologically suppressed is associated with increased risk of subsequent virologic failure. Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract TUAB0103. Hull M, et al. 20th IAC. Melbourne, Abstract TUAB0103.")
65
Me GF, 42 ans: 2012 Que proposez vous concernant le Tt ARV:
Poursuite Tt inchangé Réduction posologie des ARV (IP,TDF) Monothérapie r/DRV Bithérapie 3TC+r/IP Combinaison IP+Raltégravir Combinaison Etravirine + Raltégravir
 Monothérapie r/DRV. Bithérapie 3TC+r/IP. Combinaison IP+Raltégravir. Combinaison Etravirine + Raltégravir.")
66
145 Essai PIVOT : résultats à long terme d'un essai de switch vers monothérapie d'IP/r (1) Essai randomisé ouvert conduit dans 43 centres du Royaume Uni Trithérapie Monothérapie IP/r (n = 296) Choix de l’IP laissé au prescripteur *** Poursuite trithérapie (n = 291) Sous trithérapie (avec INNTI ou IP) CV < 50 c/ml depuis > 24 sem. CD4 > 100/mm3 Suivi 5 ans Médiane 44 mois Randomisation 1:1 ** * * Reprise des INTI si CV > 50 c/ml, retour définitif à la trithérapie si échec virologique confirmé (CV > 50 c/ml x 3), toxicité ou souhait du patient ** Retour temporaire à la trithérapie pour grossesse/allaitement ou gestion d'une interaction médicamenteuse pendant une courte durée *** DRV/r : 80 % ; LPV/r : 14 %, autres : 7% PIVOT : Protease Inhibitor monotherapy Versus Ongoing Triple Therapy. Critères de jugement Principal : perte d'options thérapeutiques, définie par l'apparition d'une nouvelle résistance de niveau intermédiaire ou haute à au moins 1 ARV auquel le virus était sensible à l’inclusion Secondaire : survenue de complications graves de la maladie Analyses en ITT, hypothèse de non-infériorité, marge inférieure 10 % Paton N, CROI 2014, Abs. 550LB
 Choix de l’IP laissé au prescripteur *** Poursuite trithérapie (n = 291) Sous trithérapie (avec INNTI ou IP) CV < 50 c/ml depuis > 24 sem. CD4 > 100/mm3. Suivi 5 ans. Médiane 44 mois. Randomisation 1:1. ** * * Reprise des INTI si CV > 50 c/ml, retour définitif à la trithérapie si échec virologique confirmé (CV > 50 c/ml x 3), toxicité ou souhait du patient. ** Retour temporaire à la trithérapie pour grossesse/allaitement ou gestion d une interaction médicamenteuse pendant une courte durée. *** DRV/r : 80 % ; LPV/r : 14 %, autres : 7% PIVOT : Protease Inhibitor monotherapy Versus Ongoing Triple Therapy. Critères de jugement. Principal : perte d options thérapeutiques, définie par l apparition d une nouvelle résistance de niveau intermédiaire ou haute à au moins 1 ARV auquel le virus était sensible à l’inclusion. Secondaire : survenue de complications graves de la maladie. Analyses en ITT, hypothèse de non-infériorité, marge inférieure 10 % Paton N, CROI 2014, Abs. 550LB.")
67
Différence Tri – Mono IP/r
146 Essai PIVOT : résultats à long terme d'un essai de switch vers monothérapie d'IP/r (2) Caractéristiques des patients et résultats entre l’inclusion et la fin du suivi Trithérapie (n = 291) Monothérapie IP/r (n = 296) Différence Tri – Mono IP/r (IC 95 %) p HSH 60 % Blanc 71 % 66 % Femme 22 % 25 % Sérologie VHC+ 7 (2 %) 14 (5 %) CD4 J0 512 ( ) 516 ( ) CD4 nadir 181 (90-258) 170 (80-239) Années depuis début ARV 3,9 (2,0-6,4) 4,2 (2,4-6,9) Nb ARV reçus en tout 5 (3-6) 4 (3-6) IP ou INNTI à J0 IP INNTI 134 (46 %) 127 (54 %) 139 (47 %) 155 (53 %) Rebond CV > 50 c/ml, confirmé, n (%) 8 (3,2 %) 95 (35,0 %) 31,8 % (24,6 à 39,0 %) < 0,001 Perte d'options thérapeutiques à M36, n (%) 2 (0,7 %) 6 (2,1 %) 1,4 (-0,4 à 3,4 %) 0,15 Perte d'options thérapeutiques fin d'essai, n (%) 4 (1,8 %) 0,2 % (-2,5 à 2,6 %) 0,85 Evolution CD4/mm3, moyenne (ET) +91 (9) +108 (9) +17 (-10 à +43) 0,21 Evénements indésirables grade 3/4 % 55 % 46 % -8,4 % (-16,4 à 0,3 %) 0,043 Evolution fonction neuro-cognitives (NPZ-5), moyenne (ET) +0,51 (0,04) +0,50 (0,04) -0,01 (-0,11 à + 0,09) 0,86 Cout des ARV (£), moyenne 30 230 21 260 -8 970 - Les auteurs concluent donc à la non-infériorité de la stratégie de monothérapie d'IP/r sur le critère principal de préservation des options thérapeutiques. Les événements indésirables de grade 3 et 4 sont un peu moins fréquents dans le bras monothérapie. Il a tout de même été observé 35 % de rebonds virologiques chez les patients du bras monothérapie IP/r, avec nécessité de modifier le traitement de façon transitoire ou définitive. 58 % des patients du bras monothérapie restaient en monothérapie à la fin de l’essai. Paton N, CROI 2014, Abs. 550LB
 Caractéristiques des patients et résultats entre l’inclusion et la fin du suivi. Trithérapie. (n = 291) Monothérapie IP/r. (n = 296) Différence Tri – Mono IP/r. (IC 95 %) p. HSH. 60 % Blanc. 71 % 66 % Femme. 22 % 25 % Sérologie VHC+ 7 (2 %) 14 (5 %) CD4 J ( ) 516 ( ) CD4 nadir. 181 (90-258) 170 (80-239) Années depuis début ARV. 3,9 (2,0-6,4) 4,2 (2,4-6,9) Nb ARV reçus en tout. 5 (3-6) 4 (3-6) IP ou INNTI à J0. IP. INNTI. 134 (46 %) 127 (54 %) 139 (47 %) 155 (53 %) Rebond CV > 50 c/ml, confirmé, n (%) 8 (3,2 %) 95 (35,0 %) 31,8 % (24,6 à 39,0 %) < 0,001. Perte d options thérapeutiques à M36, n (%) 2 (0,7 %) 6 (2,1 %) 1,4 (-0,4 à 3,4 %) 0,15. Perte d options thérapeutiques fin d essai, n (%) 4 (1,8 %) 0,2 % (-2,5 à 2,6 %) 0,85. Evolution CD4/mm3, moyenne (ET) +91 (9) +108 (9) +17 (-10 à +43) 0,21. Evénements indésirables grade 3/4 % 55 % 46 % -8,4 % (-16,4 à 0,3 %) 0,043. Evolution fonction neuro-cognitives (NPZ-5), moyenne (ET) +0,51 (0,04) +0,50 (0,04) -0,01 (-0,11 à + 0,09) 0,86. Cout des ARV (£), moyenne Les auteurs concluent donc à la non-infériorité de la stratégie de monothérapie d IP/r sur le critère principal de préservation des options thérapeutiques. Les événements indésirables de grade 3 et 4 sont un peu moins fréquents dans le bras monothérapie. Il a tout de même été observé 35 % de rebonds virologiques chez les patients du bras monothérapie IP/r, avec nécessité de modifier le traitement de façon transitoire ou définitive. 58 % des patients du bras monothérapie restaient en monothérapie à la fin de l’essai. Paton N, CROI 2014, Abs. 550LB.")
68
Essai EARNEST : 3 schémas avec IP/r en 2ème ligne en Afrique de l’Est (1)
Essai de stratégie de 2ème ligne en Afrique de l’Est (14 sites en Ouganda, Zimbabwe, Malawi, Kenya, Zambie) comparant 3 schémas avec IP/r (LPV/r dans plus de 99 % des cas) 1 277 adultes/adolescents sous 1ère ligne INNTI > 1 an ; avec observance > 90 % dans le dernier mois, en échec sur critère clinique (OMS 2010), CD4 (confirmé sur CV) ou CV Randomisation IP/r INTI en accord avec standard local TDF + 3TC/FTC : 70 % ddI + ABC : 12 % TDF + 3TC + ZDV : 9 % ZDV + 3TC : 4 % IP/r + RAL (induction 12 semaines) IP/r (monothérapie) SUIVI 144 SEMAINES Critère principal à S96 : « bon contrôle de la maladie VIH » défini par l’ensemble des critères suivants Vivant et pas de nouvel événement OMS-4 entre S0 et S96 et CD4 > 250/mm3 à S96 et CV < c/ml ou > c/ml sans mutation de R aux IP à S96 n = 426 n = 418 n = 433 Paton N, IAS 2013, Abs. WELBB02
 comparant 3 schémas avec IP/r (LPV/r dans plus de 99 % des cas) adultes/adolescents sous 1ère ligne INNTI > 1 an ; avec observance > 90 % dans le dernier mois, en échec sur critère clinique (OMS 2010), CD4 (confirmé sur CV) ou CV. Randomisation. IP/r INTI. en accord avec standard local TDF + 3TC/FTC : 70 % ddI + ABC : 12 % TDF + 3TC + ZDV : 9 % ZDV + 3TC : 4 % IP/r + RAL. (induction 12 semaines) IP/r. (monothérapie) SUIVI 144 SEMAINES. Critère principal à S96 : « bon contrôle de la maladie VIH » défini par l’ensemble des critères suivants. Vivant et pas de nouvel événement OMS-4 entre S0 et S96 et. CD4 > 250/mm3 à S96 et. CV < c/ml ou > c/ml sans mutation de R aux IP à S96. n = 426. n = 418. n = 433. Paton N, IAS 2013, Abs. WELBB02.")
69
Essai EARNEST : 3 schémas avec IP/r en 2ème ligne en Afrique de l’Est (4)
Contrôle de la CV à S96 IP/r + RAL vs IP/r + INTI p = 0,36 p = 0,87 p = 0,97 p = 0,88 IP/r mono vs IP/r + INTI p = 0,002 p < 0,0001 p < 0,0001 p < 0,0001 91 88 86 74 93 87 73 83 67 61 44 20 40 60 80 100 < c/ml < c/ml < 400 c/ml < 50 c/ml IP/r + INTI IP/r + RAL Monothérapie IP/r % Paton N, IAS 2013, Abs. WELBB02

70
IAC 2014

71
IAC 2014

72
Me GF, 42 ans: 2012 Que proposez vous concernant le Tt ARV:
Poursuite Tt inchangé Réduction posologie des ARV (IP,TDF) Monothérapie r/DRV Bithérapie 3TC+r/IP Combinaison IP+Raltégravir Combinaison Etravirine + Raltégravir
 Monothérapie r/DRV. Bithérapie 3TC+r/IP. Combinaison IP+Raltégravir. Combinaison Etravirine + Raltégravir.")
73
DRV/r 800/100 mg qd + TDF/FTC qd
113 Essai NEAT001/ANRS143 : DRV/r + (RAL ou TDF/FTC) en 1ère ligne de traitement (1) Essai de phase 3, randomisé, en ouvert, multicentrique (15 pays européens) DRV/r 800/100 mg qd + TDF/FTC qd DRV/r 800/100 mg qd + RAL 400 mg bid Minimum S96 Randomisation 1:1 stratifiée par pays et sous-étude immuno-virologique VIH+, naïfs d’ARV ≥ 18 ans CV > c/ml CD4 ≤ 500/mm3 AgHBs négatif Pas de mutations majeures de résistance (IAS-USA) Essai de non-infériorité : marge de la différence < 9 % pour le taux d’échec de RAL + DRV/r vs TDF/FTC + DRV/r à S96 (estimé par méthodes de Kaplan-Meier) en intention de traiter Raffi F, CROI 2014, Abs. 84LB
 en 1ère ligne de traitement (1) Essai de phase 3, randomisé, en ouvert, multicentrique (15 pays européens) DRV/r 800/100 mg qd + TDF/FTC qd. DRV/r 800/100 mg qd + RAL 400 mg bid. Minimum S96. Randomisation 1:1 stratifiée par pays et sous-étude immuno-virologique. VIH+, naïfs d’ARV ≥ 18 ans. CV > c/ml. CD4 ≤ 500/mm3. AgHBs négatif. Pas de mutations majeures de résistance (IAS-USA) Essai de non-infériorité : marge de la différence < 9 % pour le taux d’échec de RAL + DRV/r vs TDF/FTC + DRV/r à S96 (estimé par méthodes de Kaplan-Meier) en intention de traiter. Raffi F, CROI 2014, Abs. 84LB.")
74
118 Essai NEAT001/ANRS143 : DRV/r + (RAL ou TDF/FTC) en 1ère ligne de traitement (6) CV < 50 c/ml (% parmi patients avec données disponibles) 4 8 12 18 24 32 48 64 80 96 401 404 385 389 377 382 387 376 388 356 374 RAL + DRV/r TDF/FTC + DRV/r 20 40 60 100 Semaines 89 % 91 % 93 % n Modification moyenne (IC 95 %) depuis J0 des CD4/mm3 S48 S96 RAL + DRV/r + 197 (184, 210) + 267 (250, 285) TDF/FTC + DRV/r + 193 (180, 206) + 266 (249, 283) Raffi F, CROI 2014, Abs. 84LB
 depuis J0 des CD4/mm3. S48. S96. RAL + DRV/r (184, 210) (250, 285) TDF/FTC + DRV/r (180, 206) (249, 283) Raffi F, CROI 2014, Abs. 84LB.")
75
MODERN Trial: Treatment Outcomes (Week 48)
Maraviroc + darunavir/r Significantly lower rates of HIV RNA suppression IDMC recommended study termination (10/2013) Majority of virologic failures had HIV RNA <400 copies/mL Within each arm there was comparable efficacy by tropism assay used for screening No treatment-emergent resistance in either arm Comparable safety HIV RNA <50 Copies/mL Difference (%): -9.5 (-14.8, -4.2)* MVC + DRV/r FTC/TDF + DRV/r 89% 87% 80% 80% 77% 65% Patients (%) Slide: MODERN Trial: Treatment Outcomes (Week 48) At week 48, patients in the maraviroc + darunavir/r arm had significantly lower rates of HIV RNA suppression. The IDMC recommended study termination (10/2013).1 The majority of virologic failures had HIV RNA <400 copies/mL. In addition, within each arm there was comparable efficacy by tropism assay used for screening.1 There was no treatment-emergent resistance in either arm and both arms had comparable safety.1 Reference Stellbrink H-J, Pulik P, Szlavik J, et al. Maraviroc (MVC) dosed once daily with darunavir/ritonavir (DRV/r) in a 2 drug-regimen compared to emtricitabine/tenofovir (TDF/FTC) with DRV/r; 48-week results from MODERN (Study A ). Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract TUAB0101. VF (10%) VF (3%) Overall (n=396/401) <100K (n=315/318) >100K (n=81/83) Baseline HIV RNA (copies/mL) *Did not meet the -10% non-inferiority criteria. Stellbrink H-J, et al. 20th IAC. Melbourne, Abstract TUAB0101.
 Majority of virologic failures had HIV RNA <400 copies/mL. Within each arm there was comparable efficacy by tropism assay used for screening. No treatment-emergent resistance in either arm. Comparable safety. HIV RNA <50 Copies/mL. Difference (%): -9.5 (-14.8, -4.2)* MVC + DRV/r. FTC/TDF + DRV/r. 89% 87% 80% 80% 77% 65% Patients (%) Slide: MODERN Trial: Treatment Outcomes (Week 48) At week 48, patients in the maraviroc + darunavir/r arm had significantly lower rates of HIV RNA suppression. The IDMC recommended study termination (10/2013).1. The majority of virologic failures had HIV RNA <400 copies/mL. In addition, within each arm there was comparable efficacy by tropism assay used for screening.1. There was no treatment-emergent resistance in either arm and both arms had comparable safety.1. Reference. Stellbrink H-J, Pulik P, Szlavik J, et al. Maraviroc (MVC) dosed once daily with darunavir/ritonavir (DRV/r) in a 2 drug-regimen compared to emtricitabine/tenofovir (TDF/FTC) with DRV/r; 48-week results from MODERN (Study A ). Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract TUAB0101. VF. (10%) VF. (3%) Overall. (n=396/401) <100K. (n=315/318) >100K. (n=81/83) Baseline. HIV RNA (copies/mL) *Did not meet the -10% non-inferiority criteria. Stellbrink H-J, et al. 20th IAC. Melbourne, Abstract TUAB0101.")
76
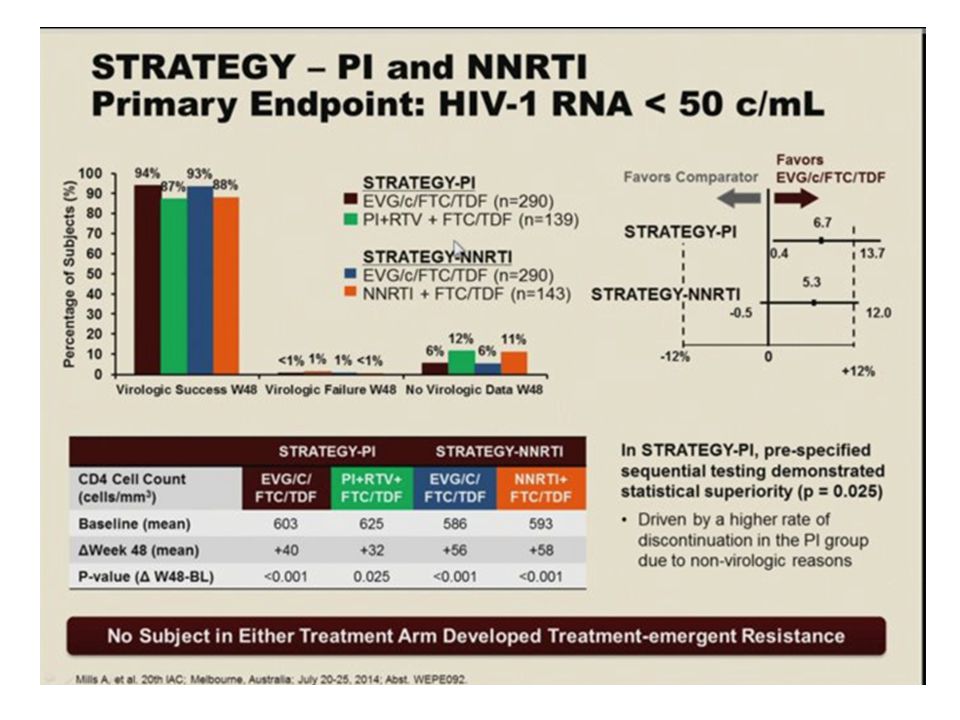
STRATEGY Studies: Switching to Elvitegravir/Cobicistat/FTC/TDF
Phase 3b studies Open label, on 1st or 2nd ART regimen, non-inferiority (12% margin) Randomized 2:1 Elvitegravir/Cobicistat/Emtricitabine/Tenofovir DF qd (n=293) STRATEGY-PI Stable PI/r + FTC/TDF (HIV RNA <50 copies/mL for >6 months) PI + RTV + Emtricitabine/Tenofovir DF (n=140) Randomized 2:1 Elvitegravir/Cobicistat/Emtricitabine/Tenofovir DF qd (n=291) STRATEGY-NNRTI Stable NNRTI + FTC/TDF (HIV RNA <50 copies/mL for >6 months) Slide: STRATEGY Studies: Switching to Elvitegravir/Cobicistat/FTC/TDF The phase 3b STRATEGY switch studies evaluated the efficacy and safety of switching virologically suppressed HIV patients on either a ritonavir-boosted PI or NNRTI regimen to the single-tablet regimen of elvitegravir/cobicistat/emtricitabine/tenofovir DF.1 The primary endpoint was HIV RNA <50 copies/mL at week 48. The non-inferiority margin was 12%.1 Reference Mills A, Wade B, Arribas J, et al. Safety analysis of switching to STB from a RTV-boosted PI or NNRTI Plus TVD regimen. Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract WEPE092. NNRTI + Emtricitabine/Tenofovir DF (n=143) Week 48 Primary Endpoint HIV RNA <50 copies/mL (“snapshot”) Week 96 Secondary outcomes: change in lipids and CD4, safety and tolerability (through week 96). Mills A, et al. 20th IAC. Melbourne, Abstract WEPE092.
 Randomized. 2:1. Elvitegravir/Cobicistat/Emtricitabine/Tenofovir DF qd. (n=293) STRATEGY-PI. Stable PI/r + FTC/TDF. (HIV RNA <50 copies/mL. for >6 months) PI + RTV + Emtricitabine/Tenofovir DF. (n=140) Randomized. 2:1. Elvitegravir/Cobicistat/Emtricitabine/Tenofovir DF qd. (n=291) STRATEGY-NNRTI. Stable NNRTI + FTC/TDF. (HIV RNA <50 copies/mL. for >6 months) Slide: STRATEGY Studies: Switching to Elvitegravir/Cobicistat/FTC/TDF. The phase 3b STRATEGY switch studies evaluated the efficacy and safety of switching virologically suppressed HIV patients on either a ritonavir-boosted PI or NNRTI regimen to the single-tablet regimen of elvitegravir/cobicistat/emtricitabine/tenofovir DF.1. The primary endpoint was HIV RNA <50 copies/mL at week 48. The non-inferiority margin was 12%.1. Reference. Mills A, Wade B, Arribas J, et al. Safety analysis of switching to STB from a RTV-boosted PI or NNRTI Plus TVD regimen. Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract WEPE092. NNRTI + Emtricitabine/Tenofovir DF. (n=143) Week 48. Primary Endpoint. HIV RNA <50 copies/mL. ( snapshot ) Week 96. Secondary outcomes: change in lipids and CD4, safety and tolerability (through week 96). Mills A, et al. 20th IAC. Melbourne, Abstract WEPE092.")
77
STRATEGY Studies: Virologic Outcomes (Week 48)
STRATEGY-PI HIV RNA <50 Copies/mL STRATEGY-NNRTI HIV RNA <50 Copies/mL Difference (%): 6.7 (0.4, 13.7)* Difference (%): 5.3 (-0.5, 12.0)* 94% 93% 87% 88% Patients (%) Patients (%) Slide: STRATEGY Studies: Virologic Outcomes (Week 48) The switch to the single-tablet regimen of elvitegravir/cobicistat/emtricitabine/tenofovir DF was found to meet non-inferiority criteria versus remaining on a stable NNRTI- or PI/r-based regimen.1 There was a low rate of virologic failure in both treatment arms of both studies.1 Reference Mills A, Wade B, Arribas J, et al. Safety analysis of switching to STB from a RTV-boosted PI or NNRTI Plus TVD regimen. Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract WEPE092. VF (<1%) VF (1%) VF (1%) VF (<1%) EVG/COBI/FTC/TDF (n=293) PI/r + FTC/TDF (n=140) EVG/COBI/FTC/TDF (n=291) NNRTI + FTC/TDF (n=143) *Non-inferiority criteria met. VF: virologic failure. Mills A, et al. 20th IAC. Melbourne, Abstract WEPE092.
: 6.7 (0.4, 13.7)* Difference (%): 5.3 (-0.5, 12.0)* 94% 93% 87% 88% Patients (%) Patients (%) Slide: STRATEGY Studies: Virologic Outcomes (Week 48) The switch to the single-tablet regimen of elvitegravir/cobicistat/emtricitabine/tenofovir DF was found to meet non-inferiority criteria versus remaining on a stable NNRTI- or PI/r-based regimen.1. There was a low rate of virologic failure in both treatment arms of both studies.1. Reference. Mills A, Wade B, Arribas J, et al. Safety analysis of switching to STB from a RTV-boosted PI or NNRTI Plus TVD regimen. Program and abstracts of the 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia. Abstract WEPE092. VF (<1%) VF (1%) VF (1%) VF (<1%) EVG/COBI/FTC/TDF. (n=293) PI/r + FTC/TDF. (n=140) EVG/COBI/FTC/TDF. (n=291) NNRTI + FTC/TDF. (n=143) *Non-inferiority criteria met. VF: virologic failure. Mills A, et al. 20th IAC. Melbourne, Abstract WEPE092.")
79
Me GF, 42 ans: 2012 Que proposez vous concernant le Tt ARV:
Poursuite Tt inchangé Réduction posologie des ARV (IP,TDF) Monothérapie r/DRV Bithérapie 3TC+r/IP Combinaison IP+Raltégravir Combinaison Etravirine + Raltégravir
 Monothérapie r/DRV. Bithérapie 3TC+r/IP. Combinaison IP+Raltégravir. Combinaison Etravirine + Raltégravir.")
80
39 patients, CV<50, suivis 27 mois
ITT: =82,1% à 12 mois

81
18 patients avec CV<200, suivis 48 semaines

82
The CD4/CD8 ratio and plasma lipids improved. Tolérance:
N=25 patients , age 54 years Previous ARV therapy: 16 years on ARV ( median of 9 previous regimens); 21 (84%) patients had previous virological failure; and 15 (60%) patients had a genotypic test that showed 3 NRTI mutations in 9 (36%), 4 or more PI mutations in 11 (44%), and 1 NNRTI mutation in 8 (32%) patients. At 48 weeks, efficacy = 84% (95% CI 65.3%–93.6%) by ITT analysis = 91.3% (95% CI 73.2%–97.6%) by PP analysis. One (4%) patient died, two (8%) discontinued due to intolerance and one (4%) experienced virological failure. The CD4/CD8 ratio and plasma lipids improved. Tolérance: 2 (8%) patients discontinued treatment due to gastro-intestinal intolerance after 8 weeks, attributed to etravirine.There were no cases of rash. One patient died due to biliary sepsis at week 40 (unrelated to antiretroviral therapy). All three patients who changed due to abnormalities in renal function showed improvement in estimated glomerular filtration rate. All patients with gastrointestinal intolerance improved except for one case of diarrhoea in a patient with cirrhosis. Neuropsychiatric symptoms improved in all patients who discontinued efavirenz-based therapy.
; 21 (84%) patients had previous virological failure; and 15 (60%) patients had a genotypic test that showed 3 NRTI mutations in 9 (36%), 4 or more PI mutations in 11 (44%), and 1 NNRTI mutation in 8 (32%) patients. At 48 weeks, efficacy = 84% (95% CI 65.3%–93.6%) by ITT analysis = 91.3% (95% CI 73.2%–97.6%) by PP analysis. One (4%) patient died, two (8%) discontinued due to intolerance and one (4%) experienced virological failure. The CD4/CD8 ratio and plasma lipids improved. Tolérance: 2 (8%) patients discontinued treatment due to gastro-intestinal intolerance after 8 weeks, attributed to etravirine.There were no cases of rash. One patient died due to biliary sepsis at week 40 (unrelated to antiretroviral therapy). All three patients who changed due to abnormalities in renal function showed improvement in estimated glomerular filtration rate. All patients with gastrointestinal intolerance improved except for one case of diarrhoea in a patient with cirrhosis. Neuropsychiatric symptoms improved in all patients who discontinued efavirenz-based therapy.")
83
RAL + ETR chez des patients avec CV indétectable
Etude observationnelle rétrospective 91 patients avec CV < 50 c/ml, ayant reçu au moins 1 mois de RAL + ETR Motif du switch pour la bithérapie : 58 % pour toxicité 10 % pour simplification Suivi médian de 11,5 mois (65 patients à M6, 48 à M12) : 21 arrêts 3 échecs virologiques 5 arrêts pour intolérance RAL et/ou ETR 13 arrêts pour autre raison CV < 50 c/ml M6 = 55/56 (98 %), M12 = 36/39 (95 %) Les 3 échecs virologiques avaient un antécédent de traitement par INNTI, avec dans 2 cas sur 3 un antécédent de mutations de résistance aux INNTI Conclusion : la bithérapie RAL + ETR ne doit pas être utilisée en cas d’antécédent d’échec sous INNTI est associée à un taux élevé d’arrêts de traitement Seuls les patients ayant reçu plus d’un mois de l’association RAL + ETR sont analysés. Il n’est pas précisé combien de patients mis sous cette bithérapie ont arrêté au cours du 1er mois. La raison du switch pour la bithérapie n’est pas indiquée chez un tiers des patients. Les raisons d’arrêt ne sont pas clairement indiquées. Calin R, IAS 2013, Abs. WEPE516
 : 21 arrêts. 3 échecs virologiques. 5 arrêts pour intolérance RAL et/ou ETR. 13 arrêts pour autre raison. CV < 50 c/ml M6 = 55/56 (98 %), M12 = 36/39 (95 %) Les 3 échecs virologiques avaient un antécédent de traitement par INNTI, avec dans 2 cas sur 3 un antécédent de mutations de résistance aux INNTI. Conclusion : la bithérapie RAL + ETR. ne doit pas être utilisée en cas d’antécédent d’échec sous INNTI. est associée à un taux élevé d’arrêts de traitement. Seuls les patients ayant reçu plus d’un mois de l’association RAL + ETR sont analysés. Il n’est pas précisé combien de patients mis sous cette bithérapie ont arrêté au cours du 1er mois. La raison du switch pour la bithérapie n’est pas indiquée chez un tiers des patients. Les raisons d’arrêt ne sont pas clairement indiquées. Calin R, IAS 2013, Abs. WEPE516.")
84
Me GF, 42 ans: 2012 Adaptation posologique des ARV proposée du fait
Atteinte rénale modérée sous ténofovir Troubles digestifs persistants sous DRV Dosage élevé de TDF et de DRV Traitement 11/06/12 Truvada 1jour/2 + FTC + RTV100/DRV600 x1

85
Lien effet-dose concernant la tolérance/EI des ARV
nucléosidiques : TFV et tubulopathies DDI et pancréatite d4T et mitochondriopathie INNTI : EFV et SNC/suicidalité, NVP et foie Inhibiteurs d’entrée: MVC et hypotension Antiprotéases : IP et lipides, risque CV ATV et lithiases Anti-intégrases : RAL et troubles du sommeil D’après G. Peytavin

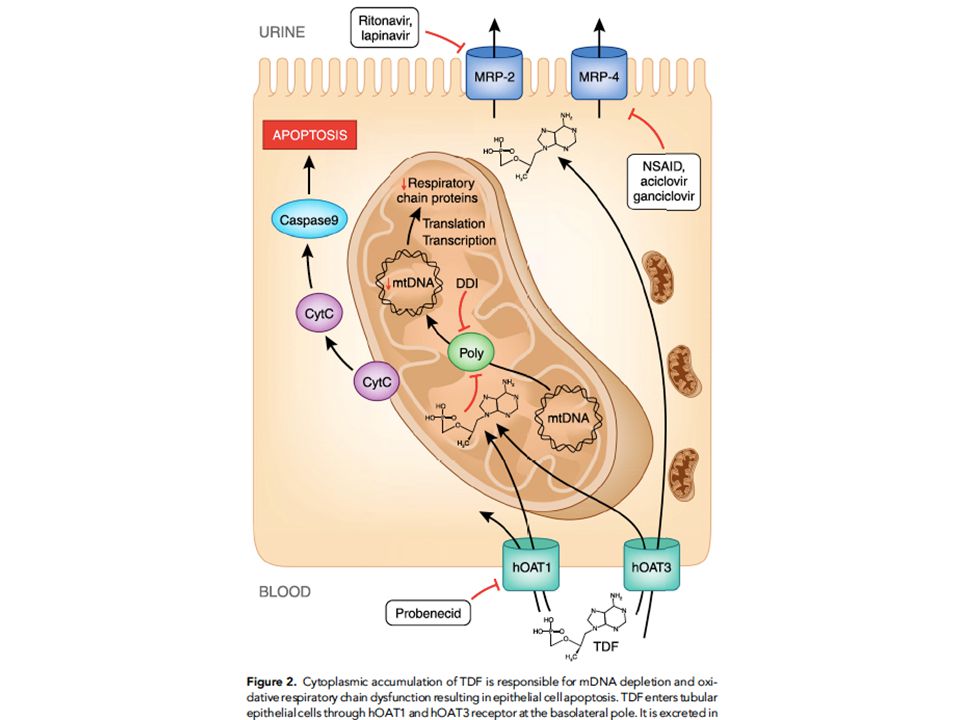
87
Impairment in kidney tubular function in patients receiving tenofovir is associated with higher tenofovir plasma concentrations 92 patients sous TDF depuis 33 mois (méd.) 18 patients KTD+ 74 patients normal renal function Dosage TDF= C12h Sonia Rodrıguez-Novo et coll., AIDS 2010, 24:1063–1075
 18 patients KTD+ 74 patients normal renal function. Dosage TDF= C12h. Sonia Rodrıguez-Novo et coll., AIDS 2010, 24:1063–1075.")
88
Atteinte rénale définie par eGFR<90 ml/mn
Association Between Tenofovir Exposure and Reduced Kidney Function in a Cohort of HIV-Positive Patients: Results From 10 Years of Follow-up 1043 patients suivis 10 ans Atteinte rénale définie par eGFR<90 ml/mn Tenofovir exposure increased the risk of kidney dysfunction by 63% (HR, 1.63; 95% CI 1.26–2.10) The cumulative eGFR loss directly attributable to TDF after 1, 2, 3, and 4 years of TDF exposure was −3.05 (P = .017), −4.05 (P = .000), −2.42 (P = .023), and −3.09 mL/min/1.73 m2 (P = .119) C. Laprise et coll., Clin. Inf. Dis, 2012
 The cumulative eGFR loss directly attributable to TDF after 1, 2, 3, and 4 years of TDF exposure was −3.05 (P = .017), −4.05 (P = .000), −2.42 (P = .023), and −3.09 mL/min/1.73 m2 (P = .119) C. Laprise et coll., Clin. Inf. Dis,")
89
Réduction de dose de ténofovir chez 56 patients avec atteinte rénale et/ou surdosage plasmatique de TDF D. Marigot-Outtandy1, JNI 2014

90
56 patients sous TDF réduit
D. Marigot-Outtandy1, JNI 2014

91
Me GF, 42 ans: 2014 Traitement TDF/2jrs+FTC+rDRV600: disparition diarrhée et ballonnements Evolution fonction rénale: Créatinine 92μM/l, MDRD 85ml/mn, protéinurie 0,35g/l Dosage TDF Cres= 67ng/ml, DRV= 1430ng/ml dates ARV CV CD4 11/06/12 TDF1/2+FTC+rDRV <20 515 18/12/12 :* 465 5/09/13 673 16/03/14 21 565 30/06/14 494 9/09/14 584 *: prise DRV/r 5 jours sur 7

93
Me LB, 1946 Affections liées au VIH:
infection VIH diagnostiquée en 1994 Antécédents: Phlébite des MI 1997, sclérose varices 2001 Anémie ferriprive 1998 Herpès génital récurrent, condylomes BPCO post tabagique cataracte Affections liées au VIH: Zona 2003 Candidose récurrente Pneumopathies bactériennes Statut immunovirologique: Traitement ARV en 1996??: d4T+3TC+IDV, non suivi Nadir CD4: 200

94
Me LB, 1946 dates ARV CV CD4 1997 d4T+3TC+IDV? - ? 25/09/97 d4T+3TC+r/SQV 135500 200 17/09/98 : <50 687 28/01/99 AZT+3TC+EFV 549 11/05/01 906 19/02/02 151000 459 2/03/04 65000 365 7/06/04 430 31/05/05 135000 384 17/07/06 TDF+FTC+EFV 141000 397 28/08/06 :? 79 396 2/01/08 AZT+3TC+r/LPV 206000 336 17/03/08 TDF+FTC+rDRV 257000 241 2/09/09 <20 525 Génotypes: 2007: RT = 65R 184V-100I 103N PRO = 36I, 62V 2008: RT= 103N PRO: 36I 62V

95
Me LB, 1946: 2008 Arrêts répétés et prolongés du traitement ARV jusqu’en 2007; difficultés de suivi. Pas d’effets indésirables majeurs mais se plaint d’un malaise général sous traitement Lipodystrophie ( hypertrophie abdominale: VAT:166cm2, SAT:198cm2), lipomes Ostéodensitométrie: t-score hanche G: -1.0, rachis L: -1.5 Tt ARV: Truvada +r/DRV (17/03/08) 2008: CV<20, CD4=480 à 618 Réclame une diminution des prises d’ARV….
, lipomes. Ostéodensitométrie: t-score hanche G: -1.0, rachis L: Tt ARV: Truvada +r/DRV (17/03/08) 2008: CV<20, CD4=480 à 618. Réclame une diminution des prises d’ARV….")
96
Me LB, 1946: 2008 Quelle adaptation thérapeutique proposer:
Simplification pour Eviplera Pas de changement de Tt Monothérapie r/DRV Diminution de posologie du DRV Switch pour Truvada+raltégravir

97
Me LB, 1946: 2008 Quelle adaptation thérapeutique proposer:
Simplification pour Eviplera: antécédents mutation 184V et INNRT Pas de changement de Tt: Risque de nouvelles interruptions Monothérapie r/DRV: Doute sur observance Diminution de posologie du DRV: Pas de publications… Switch pour Truvada+raltégravir: Risque de tt suboptimal, antécédents de résistance RT (SWITCHMRK)
")
98
Me LB, 1946: 2010 et après Refus prise en charge ETP Pas de suivi psy
Dosages plasmatiques DRV satisfaisants, voire élevés: RTV C12h= 137 ng/ml; DRV C12h= 5248 ng/ml Pas de changement de molécules… mais réduction des prises hebdomadaires: Réduction des prises hebdomadaires : Truvada +r/DRV jours/7 (puis 4 jours/7)
")
99
Me LB, 1946: 2010 et après Dosages plasmatiques:
DRV Cres(J3)= 60ng/ml, RTV<10 ng/ml, TDF= 10ng/ml Traitement Truvada + R/DRV800 dates ARV CV CD4 17/03/08 TDF+FTC+rDRV 257000 241 2/09/09 : <20 525 17/03/10 TDF+FTC+rDRV 4j/7 521 16/09/10 591 17/05/11 625 18/09/12 584 28/05/13 TDF+FTC+rDRV 3j/7 29 20/01/14 682 28/07/14 757
= 60ng/ml, RTV<10 ng/ml, TDF= 10ng/ml. Traitement Truvada + R/DRV800. dates. ARV. CV. CD4. 17/03/08. TDF+FTC+rDRV /09/09. : < /03/10. TDF+FTC+rDRV 4j/ /09/ /05/ /09/ /05/13. TDF+FTC+rDRV 3j/ /01/ /07/")
100
• JID 2004:189 (1 June) • Dybul et al., 1974-82
Eight patients with a history of receiving combination ART that maintained suppression of plasma HIV RNA to <50 copies/mL received a once-daily SIT regimen of didanosine, lamivudine, and efavirenz. For 7 patients, suppression of plasma HIV RNA to <50 copies/mL was maintained for 60–84 weeks. Four patients with adequate samples had no evidence for an increase in plasma viremia for up to 72 weeks, by use of an assay with a limit of detection of <1 copy/mL. The lack of rebound viremia may be the result of the persistence of efavirenz in plasma on day 7 of the no-therapy period, as was detected in 7 of 7 patients. • JID 2004:189 (1 June) • Dybul et al.,
 • Dybul et al.,")
101
FOTO: 5-Days-On, 2-Days-Off Treatment Strategy With EFV/TDF/FTC
Cohen, Glasgow 2008; IAS 2009

102
Dominique Mathez D Mathez, ANRS 102

103
Etude Leibowitch et al., FASEB Journal, 2010

104
PLoS ONE | www.plosone.org, April 2010 | Volume 5 | Issue 4 | e10307

105
Traitement intermittent court: données publiées
essai N pts ARV Type étude suivi succès Dybul 2001 10 IP,INN Ouverte, 7on-7off >48S 8/10 Dybul 2005 8 EFV 7/8 Cohen, FOTO, 2009 25 50 Randomisée 24S, 5j/7 ouverte S48 24S 48S 100% 90% Reynolds 2010 57 Randomisée, 5j/7 72S Leibowitch 2011 63 52 Tous ARV Ouverte, 4j/7 3j/7 57S 39S 46/52 (88%) Total 188 173/188 (92%) *Étude BJ Rudy 2009 (AIDS RESEARCH AND HUMAN RETROVIRUSES Volume 25, Number 6, 2009) exclue: 32 adolescents, CV parfois non indétectable à J0, traitements ARV parfois inefficaces (résistance préalable)
 Total /188 (92%) *Étude BJ Rudy 2009 (AIDS RESEARCH AND HUMAN RETROVIRUSES Volume 25, Number 6, 2009) exclue: 32 adolescents, CV parfois non indétectable à J0, traitements ARV parfois inefficaces (résistance préalable)")
106
Données actualisées cohorte JL 2013
84 patients traités 4jrs/7 Durée médiane 53 semaines (7-321)- 48 pts suivis pendant>1 an Devenir des 84 patients: Échec sous Tt 4j/7: 0 Toujours 4j/7: Arrêt patient, reprise 7j/7: 3 <4jrs/7: Perdu de vue: 1 N= Durée méd. IP 22 50 sem NNRTI 46 mixte 11 Autre combo 5 69 sem
- 48 pts suivis pendant>1 an. Devenir des 84 patients: Échec sous Tt 4j/7: 0. Toujours 4j/7: 10. Arrêt patient, reprise 7j/7: 3. <4jrs/7: 70. Perdu de vue: 1. N= Durée méd. IP sem. NNRTI. 46. mixte. 11. Autre combo sem.")
107
Adhesion, durée arrêt ARV, et risque de rebond virologique sous INNRT
72 patients sous NNRTI >3mois, VL<50 Observance mesurée par MEMS Définition rebond = VL>400 Risque VF: +10%adherence: OR=0,56[0,37-0,81] +1 interruption>2d: OR=1,34 [1,15-1,68] durée interruption+1d: OR=1,38 [1,13-1,77] Parienti JJ, PlOs One, 2008, 3 (7), e2783
, e2783.")
108
Évolution des marqueurs inflammatoires sous traitement intermittent :
Suivi longitudinal : 7 => 4 => 3 jours par semaine Semaines depuis l’instauration des ARVs D. Mathez

109
Évolution de l’ADN proviral sous traitement intermittent :
D. Mathez

110
Évolution des marqueurs inflammatoires sous traitement intermittent :
Losanges ocre jaune : points transversaux, patients tous 7 jours sur 7 Ronds verts : points longitudinaux, patients à 7 => 4 => 3 jours/ sem D. Mathez

Présentations similaires