Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Prévention de la néphropathie aux produits de contraste
Philippe Thorel

2
Physiopathologie NTA Endothéline ? Adénosine ? ↓ NO ?
↑ viscosité sanguine ? Vasoconstriction rénale ? Stress oxydatif ? Cytotoxicité directe ? Hypoxie médullaire ? NTA

3
Facteurs de risque IRC +++ Diabète Insuffisance cardiaque
Dose et Type PdC (haute osmolarité ++) Myélome
 Myélome.")
4
Hypothèses sur l ’effet protecteur de l’hydratation
Dilution du PdC dans la lumière tubulaire Réduction activation SRAA ? Diminution production radicaux libres ? Alcalinisation des urines (bicarbonates) ?
")
5
Aucune certitude… NaCl ? HCO3- ? N-Acetyl-Cystéine ??
Volume d’hydratation ?

6
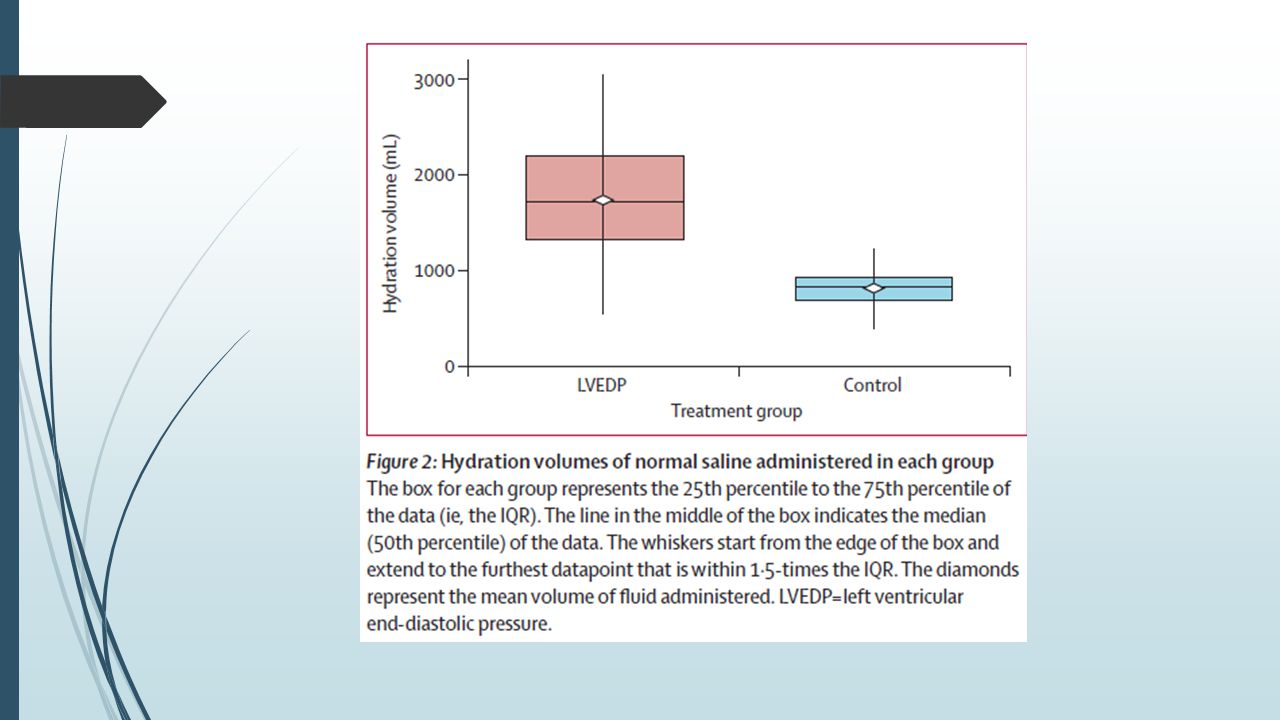
Haemodynamic-guided fluid administration for the prevention of contrast-induced acute kidney injury : the POSEIDON randomised trial Somjat S Brar et al. Lancet Mai 2014

7
Objectif Évaluer différentes stratégies d’hydratation basées sur la pression télédiastolique du VG chez des patients ayant une coronarographie

8
Methodes Essai randomisé Simple aveugle Patients consécutifs
Cathéterisme cardiaque au Kaiser medical center, Los Angeles Entre Octobre 2010 et Juillet 2012

9
Critères d’inclusion DFG < 60 mL/min (MDRD) Au moins 1 parmi :
Diabète Insuffisance cardiaque HTA Age > 75 ans Exclusion : cathéterisme urgent, transplantation rénale, injection PdC < 48h, allergie aux PdC

10
coro Traitement: 1h 4h 5 mL/kg/h si PTDVG < 13mmHg 3 mL/kg/h si PTDVG mmHg 1.5 mL/kg/h si PTDVG >18 mmHg 3 mL/kg coro Contrôle : 1h 4h 3 mL/kg 1.5 mL/kg/h

11
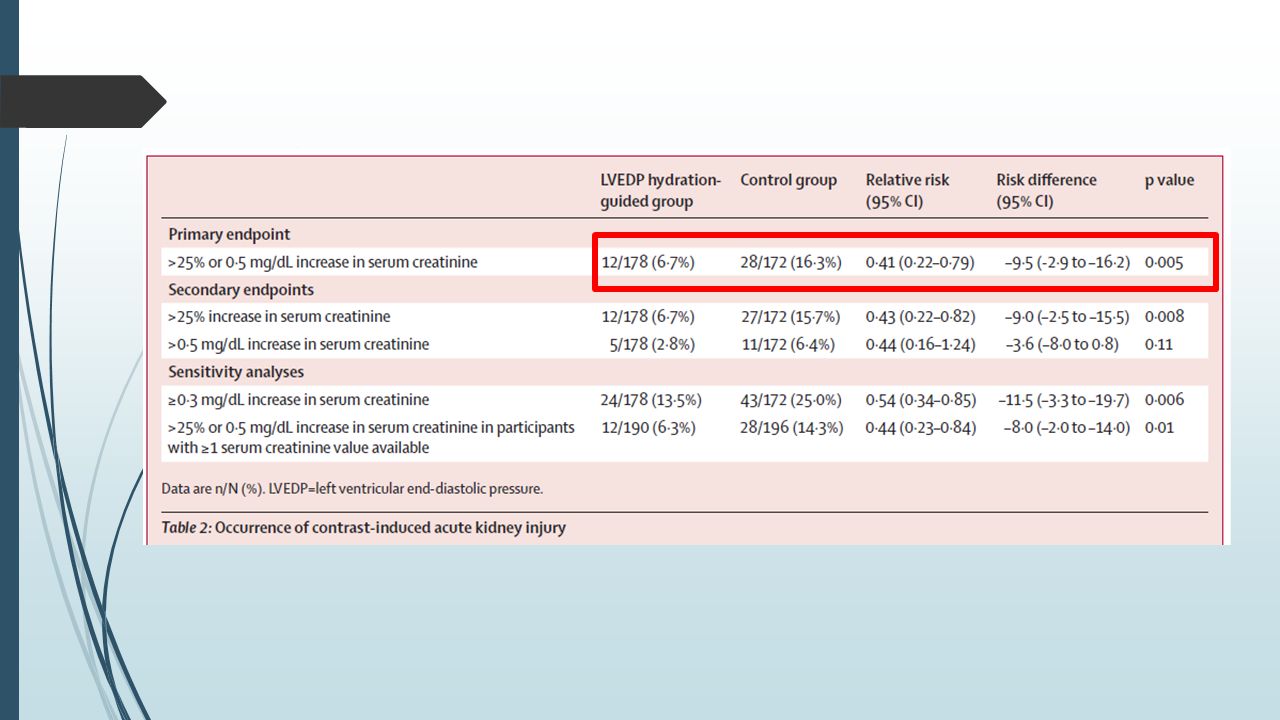
Critère de jugement principal : survenue d’IRA
Dosage de créatinine: J0 (avant injection) 2 fois entre J1 et J4 Critère de jugement principal : survenue d’IRA ↑ Cr > 25% ou 0,5mg/dL (44µmol/L)
 2 fois entre J1 et J4. Critère de jugement principal : survenue d’IRA. ↑ Cr > 25% ou 0,5mg/dL (44µmol/L)")
12
Résultats

16
Discussion Étude randomisée Forte puissance
Patients ayant un cathétérisme cardiaque Hydratation faible groupe contrôle

17
A randomized comparison of 1-h sodium bicarbonate hydration versus standard peri-procedural saline hydration in patients with chronic kidney disease undergoing intravenous contrast-enhanced computerized tomography J. Kooiman et al., NDT Feb 2014

18
Methodes Essai randomisé De non-infériorité En ouvert
4 hôpitaux hollandais Janvier 2010 – Juin 2012

19
Critères d’inclusion Patients ayant un TDM injecté
DFG < 60 mL/min (MDRD) Exclusion si : Administration PdC < 7j Allergie aux PdC grossesse
 Exclusion si : Administration PdC < 7j. Allergie aux PdC. grossesse.")
20
TDM Groupe 1: 1h Groupe 2 : 1000mL NaCl 0,9% 1000mL NaCl 0,9% 4-12h
HCO3- 1,4% 1h Groupe 2 : 1000mL NaCl 0,9% 1000mL NaCl 0,9% 4-12h 4-12h

21
Critère de jugement principal :
Dosage Créatinine : J0 (avant hydratation) Entre J2 et J3 Critère de jugement principal : Augmentation relative créatininémie / J0 Secondaire : incidence d’IRA, survenue évènements CV Evaluation de coûts : Coûts directs, ambulatoire/HdJ,…
 Entre J2 et J3. Critère de jugement principal : Augmentation relative créatininémie / J0. Secondaire : incidence d’IRA, survenue évènements CV. Evaluation de coûts : Coûts directs, ambulatoire/HdJ,…")
24
Élévation moyenne créatininémie :
1,2% pour groupe bicarbonate 1,5% pour groupe serum phy p < 0,0001 pour non-infériorité OAP : HCO3- : 0/267 NaCl : 6/281

25
Analyse de coûts

26
Discussion Étude randomisée Forte puissance Procédure simple
Applicable en ambulatoire Critère de jugement principal

27
Maioli et al. Journal of the American College of Cardiology, Jan 2014
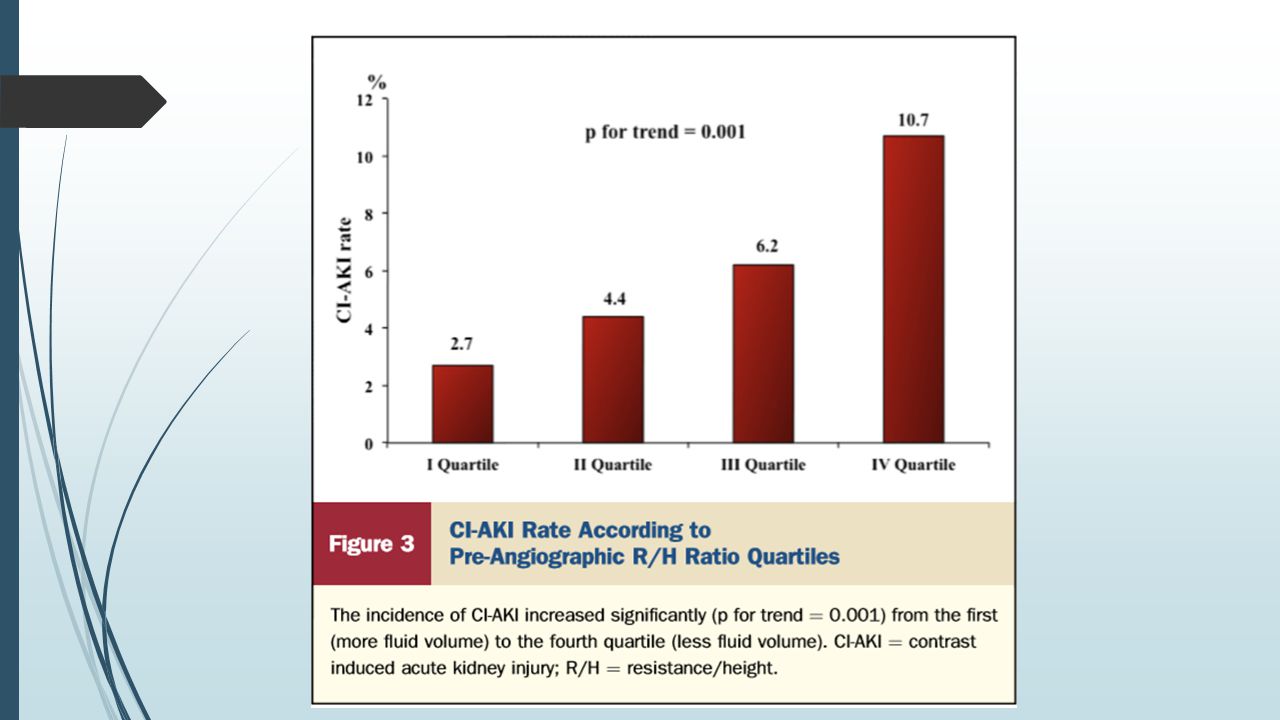
Pre-procedural Bioimpedance Vector Analysis of Fluid Status and Prediction of Contrast-Induced Acute Kidney Injury Maioli et al. Journal of the American College of Cardiology, Jan 2014

28
Principe BIVA Mesure Resistance (R) et Reactance (Xc)
Calcul Impedance 𝑍 =√( 𝑅 2 +𝑋 𝑐 2 ) Calcul ratios R/H et Z/H (H=taille patient) Z R
 Calcul ratios R/H et Z/H (H=taille patient) Z. R.")
29
Xc/H R/H

30
Méthodes Recrutement tous patients ayant coronarographie
Hopital de Prato Entre Septembre 2009 et Aout 2011 Exclusion : Coro urgente Machine indisponible Administration PdC <10j Dialyse Refus du patient

31
Procédure Hydratation 1mL/kg/h NaCl 0,9% 12h avant et 12h après
NAC 600 x 2 J0, J1 Dosage créat J0, J1, J2, J3 Mesure BIVA en salle de coro Évaluation mesure sur 50 patients : 0,5% intrapatient/1,6% interopérateur CJP : survenue IRA ↑ Créat > 0,5 mg/dL (44µmol/L) dans les 3 jours
 dans les 3 jours.")
32
Résultats 900 patients inclus 54 cas IRA (6,0%)
2,3 % (14/586) parmi DFG > 60mL/min 12,7% (40/314) parmi DFG < 60mL/min
 parmi DFG > 60mL/min. 12,7% (40/314) parmi DFG < 60mL/min.")
34
Pas d’IRA IRA

36
Discussion 1e étude évaluant BCM avant PdC
Procédure simple, peu coûteuse Descriptive Coronarographie Reproductibilité ?

37
QUE FAIRE ?

38
Mesures générales Produit de contraste Evaluer volémie
faible osmolarité/iso-osmolaires Limitation dose Evaluer volémie BCM ? Hydratation IV / Arrêt diurétiques N-Acetyl-Cystéine ? (1200mg x 2 PO J-1 et J0) (statines ?) (arrêt IEC/ARA2 ?)
 (statines ) (arrêt IEC/ARA2 )")
39
Thorel et al. The Bois-Guillaume Journal of Nephrology, Nov 2014
Clinical practice towards prevention of contrast-induced acute kidney injury : a prospective monocenter study Thorel et al. The Bois-Guillaume Journal of Nephrology, Nov 2014

40
Méthodes Cas = Néphrologues exerçant au CHU BG N=9
Le 20/10/14 entre 18h et 19h Questionnaire standardisé

41
Résultats oui non NSPP HCO3-/NaCl ? HCO3- : 5 NaCl : 2 2 Volume
1L J-1 :1 1L J-1, J0 : 7 1L J-1, J0, J1 : 1 Hydratation orale ? 4 (si risque modéré) 5 Arrêt diurétiques 9 N-AcetylCystéine ? 3 6 Arrêt IEC/ARA2 ? 7
 5. Arrêt diurétiques. 9. N-AcetylCystéine Arrêt IEC/ARA2 7.")
42
Ce que disent les KDIGO 4.4.1: We recommend i.v. volume expansion with either isotonic sodium chloride or sodium bicarbonate solutions, rather than no i.v. volume expansion, in patients at increased risk for CI-AKI. (1A) 4.4.2: We recommend not using oral fluids alone in patients at increased risk of CI-AKI. (1C) 4.4.3: We suggest using oral NAC, together with i.v. iso- tonic crystalloids, in patients at increased risk of CI-AKI. (2D) 4.4.4: We suggest not using theophylline to prevent CI-AKI. (2C) 4.4.5: We recommend not using fenoldopam to prevent CI-AKI. (1B) 4.5.1: We suggest not using prophylactic intermittent hemodialysis (IHD) or hemofiltration (HF) for contrast-media removal in patients at increased risk for CI-AKI. (2C)
 4.4.2: We recommend not using oral fluids alone in patients at increased risk of CI-AKI. (1C) 4.4.3: We suggest using oral NAC, together with i.v. iso- tonic crystalloids, in patients at increased risk of CI-AKI. (2D) 4.4.4: We suggest not using theophylline to prevent CI-AKI. (2C) 4.4.5: We recommend not using fenoldopam to prevent CI-AKI. (1B) 4.5.1: We suggest not using prophylactic intermittent hemodialysis (IHD) or hemofiltration (HF) for contrast-media removal in patients at increased risk for CI-AKI. (2C)")
43
Quel protocole d’hydratation ??
Patient ambulatoire, risque modéré : Patient hospitalisé / haut risque : 250mL HCO3- 14‰ 1h 1000mL NaCl 0,9% 1000mL NaCl 0,9% 12h 12h 250mL HCO3- 14‰ 500mL HCO3- 14‰ 6h 1h

Présentations similaires




















,>")


