Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Nouvelles stratégies de prise en charge
Traitements non antibiotiques des infections graves B. Guery (Lille)
")
2
1991….

3
Placebo n=92 HA-1A n=105 70% 77% 51% 43% Double blind randomized study, 543 patients

4
« We stopped the trial at the first interim analysis because the all-cause mortality rate for patients treated with HA-1A who did not have Gram-negative bacteremia (42%; 244 of 577) exceeded that of the patients given placebo (38%; 230 of 608) by an amount greater than that in the prespecified safety stopping rule (F = 0.09; Fisher one-tailed exact test). » Objective: To compare the effectiveness of 100 mg of HA-1A and placebo in reducing the 14-day all-cause mortality rate in patients with septic shock and gram-negative bacteremia in the Centocor: HA-1A Efficacy in Septic Shock (CHESS) trial, and to assess the safety of 100 mg of HA-1 A given to patients with septic shock who did not have gram-negative bacteremia. • Design: Large, simple, group-sequential, randomized, double-blind, multicenter, placebo-controlled trial. • Setting: 603 investigators at 513 community and university-affiliated hospitals in the United States. • Patients: Within 6 hours before enrollment, the patients had been in shock with a systolic blood pressure of less than 90 mm Hg after adequate fluid challenge or had received vasopressors to maintain blood pressure. These episodes of shock began within 24 hours of enrollment. A presumptive clinical diagnosis of gram-negative infection as the cause of the shock episode and a commitment from the patients' physicians to provide full supportive care were required. • Measurements: Blood cultures were obtained within 48 hours of enrollment, and death at day 14 after treatment was recorded. Adverse events occurring within 14 days after enrollment were also tabulated. • Results: 2199 patients were enrolled; 621 (28.2%) met all enrollment criteria, received HA-1 A or placebo, and had confirmed gram-negative bacteremia. Mortality rates in this group were as follows: placebo, 32% (95 of 293) and HA-1 A, 33% (109 of 328) (P = 0.864, Fisher exact test, two-tailed; 95% CI for the difference, -6.2% to 8.6%). Mortality rates in the patients without gram-negative bacteremia were as follows: placebo, 37% (292 of 793) and HA-1 A, 41% (318 of 785) (P = 0.073, Fisher exact test, one-tailed; CI, -0.8% to 8.8%). • Conclusions: In this trial, HA-1 A was not effective in reducing the 14-day mortality rate in patients with gram-negative bacteremia and septic shock. These data do not support using septic shock as an indication for HA-1 A treatment. If HA-1 A is effective in reducing the mortality rate in patients dying from endotoxemia, these patients must be identified using other treatment criteria.
 trial, and to assess the safety of 100 mg of HA-1 A given to patients with septic shock who did not have gram-negative bacteremia. • Design: Large, simple, group-sequential, randomized, double-blind, multicenter, placebo-controlled trial. • Setting: 603 investigators at 513 community and university-affiliated hospitals in the United States. • Patients: Within 6 hours before enrollment, the patients had been in shock with a systolic blood pressure of less than 90 mm Hg after adequate fluid challenge or had received vasopressors to maintain blood pressure. These episodes of shock began within 24 hours of enrollment. A presumptive clinical diagnosis of gram-negative infection as the cause of the shock episode and a commitment from the patients physicians to provide full supportive care were required. • Measurements: Blood cultures were obtained within 48 hours of enrollment, and death at day 14 after treatment was recorded. Adverse events occurring within 14 days after enrollment were also tabulated. • Results: 2199 patients were enrolled; 621 (28.2%) met all enrollment criteria, received HA-1 A or placebo, and had confirmed gram-negative bacteremia. Mortality rates in this group were as follows: placebo, 32% (95 of 293) and HA-1 A, 33% (109 of 328) (P = 0.864, Fisher exact test, two-tailed; 95% CI for the difference, -6.2% to 8.6%). Mortality rates in the patients without gram-negative bacteremia were as follows: placebo, 37% (292 of 793) and HA-1 A, 41% (318 of 785) (P = 0.073, Fisher exact test, one-tailed; CI, -0.8% to 8.8%). • Conclusions: In this trial, HA-1 A was not effective in reducing the 14-day mortality rate in patients with gram-negative bacteremia and septic shock. These data do not support using septic shock as an indication for HA-1 A treatment. If HA-1 A is effective in reducing the mortality rate in patients dying from endotoxemia, these patients must be identified using other treatment criteria.")
5
Objective: Phase III study to confirm a trend observed in a
previous phase II study showing that a single dose of lenercept, human recombinant p55 tumor necrosis factor receptor-immunoglobulin G1 (TNFR55-IgG1) fusion protein, decreased mortality in patients with severe sepsis or early septic shock. Design: Multicenter, double-blind, phase III, placebo-controlled, randomized study. Setting: A total of 108 community and university-affiliated hospitals in the United States (60), Canada (6) and Europe (42). Patients: A total of 1,342 patients were recruited who fulfilled the entry criteria within the 12-hr period preceding the study drug administration. Intervention: After randomization, an intravenous dose of 0.125 mg/kg lenercept or placebo was given. The patient was monitored for up to 28 days, during which standard diagnostic, supportive, and therapeutic care was provided. Measurements and Main Results: The primary outcome measure was 28-day all-cause mortality. Baseline characteristics were as follows: a total of 1,342 patients were randomized; 662 received lenercept and 680 received placebo. The mean age was 60.5 yrs (range, 17–96 yrs); 39% were female; 65% had medical admissions, 8% had scheduled surgical admissions, and 27% had unscheduled surgical admissions; 73% had severe sepsis without shock, and 27% had severe sepsis with early septic shock. Lenercept and placebo groups were similar at baseline with respect to demographic characteristics, simplified acute physiology score II-predicted mortality, profiles of clinical site of infection and microbiological documentation, number of dysfunctioning organs, and interleukin-6 (IL-6) plasma concentration. Lenercept pharmacokinetics were similar in severe sepsis and early septic shock patients. Tumor necrosis factor was bound in a stable manner to lenercept as reflected by the accumulation of total serum tumor necrosis factor a concentrations. There were 369 deaths, 177 on lenercept (27% mortality) and 192 on placebo (28% mortality). A one-sided Cochran-Armitage test, stratified by geographic region and baseline, predicted 28-day all-cause mortality (simplified acute physiology score II), gave a p value of .141 (one-sided). Lenercept treatment had no effect on incidence or resolution of organ dysfunctions. There was no evidence that lenercept was detrimental in the overall population. Conclusion: Lenercept had no significant effect on mortality in the study population. ( “Lenercept had no significant effect on mortality in the study population”
 fusion protein, decreased mortality in. patients with severe sepsis or early septic shock. Design: Multicenter, double-blind, phase III, placebo-controlled, randomized study. Setting: A total of 108 community and university-affiliated. hospitals in the United States (60), Canada (6) and Europe (42). Patients: A total of 1,342 patients were recruited who fulfilled. the entry criteria within the 12-hr period preceding the study drug. administration. Intervention: After randomization, an intravenous dose of mg/kg lenercept or placebo was given. The patient was monitored. for up to 28 days, during which standard diagnostic, supportive, and therapeutic care was provided. Measurements and Main Results: The primary outcome measure. was 28-day all-cause mortality. Baseline characteristics. were as follows: a total of 1,342 patients were randomized; 662. received lenercept and 680 received placebo. The mean age was yrs (range, 17–96 yrs); 39% were female; 65% had medical. admissions, 8% had scheduled surgical admissions, and 27% had. unscheduled surgical admissions; 73% had severe sepsis without. shock, and 27% had severe sepsis with early septic shock. Lenercept and placebo groups were similar at baseline with. respect to demographic characteristics, simplified acute physiology. score II-predicted mortality, profiles of clinical site of infection. and microbiological documentation, number of dysfunctioning. organs, and interleukin-6 (IL-6) plasma concentration. Lenercept pharmacokinetics were similar in severe sepsis and. early septic shock patients. Tumor necrosis factor was bound in. a stable manner to lenercept as reflected by the accumulation of. total serum tumor necrosis factor a concentrations. There were. 369 deaths, 177 on lenercept (27% mortality) and 192 on placebo. (28% mortality). A one-sided Cochran-Armitage test, stratified by. geographic region and baseline, predicted 28-day all-cause mortality. (simplified acute physiology score II), gave a p value of (one-sided). Lenercept treatment had no effect on incidence or. resolution of organ dysfunctions. There was no evidence that. lenercept was detrimental in the overall population. Conclusion: Lenercept had no significant effect on mortality in. the study population. ( Lenercept had no significant effect on mortality in the study population")
6
2001….

7
The inflammatory and procoagulant host responses to infection are intricately linked. Infectious agents and inflammatory cytokines such as tumor necrosis factor (TNF- ) and interleukin-1 activate coagulation by stimulating the release of tissue factor from monocytes and the endothelium. The presentation of tissue factor leads to the formation of thrombin and a fibrin clot. Inflammatory cytokines and thrombin can both impair the endogenous fibrinolytic potential by stimulating the release of plasminogen-activator inhibitor 1 (PAI-1) from platelets and the endothelium. PAI-1 is a potent inhibitor of tissue plasminogen activator, the endogenous pathway for lysing a fibrin clot. In addition, the procoagulant thrombin is capable of stimulating multiple inflammatory pathways and further suppressing the endogenous fibrinolytic system by activating thrombin-activatable fibrinolysis inhibitor (TAFI). The conversion of protein C, by thrombin bound to thrombomodulin, to the serine protease activated protein C is impaired by the inflammatory response. Endothelial injury results in decreased thrombomodulin levels. The end result of the host response to infection may be the development of diffuse endovascular injury, microvascular thrombosis, organ ischemia, multiorgan dysfunction, and death. Activated protein C can intervene at multiple points during the systemic response to infection. It exerts an antithrombotic effect by inactivating factors Va and VIIIa, limiting the generation of thrombin. As a result of decreased thrombin levels, the inflammatory, procoagulant, and antifibrinolytic response induced by thrombin is reduced. In vitro data indicate that activated protein C exerts an antiinflammatory effect by inhibiting the production of inflammatory cytokines (TNF- , interleukin-1, and interleukin-6) by monocytes and limiting the rolling of monocytes and neutrophils on injured endothelium by binding selectins. Activated protein C indirectly increases the fibrinolytic response by inhibiting PAI-1.12,13,14,15,16,17 NEJM 2001

8
Mortalité –20% 24.7% 30.8% NEJM 2001

10
LPS TNF Pas bon…..

12
“My approach is nontraditional, but from a uniquely Western perspective.”

13
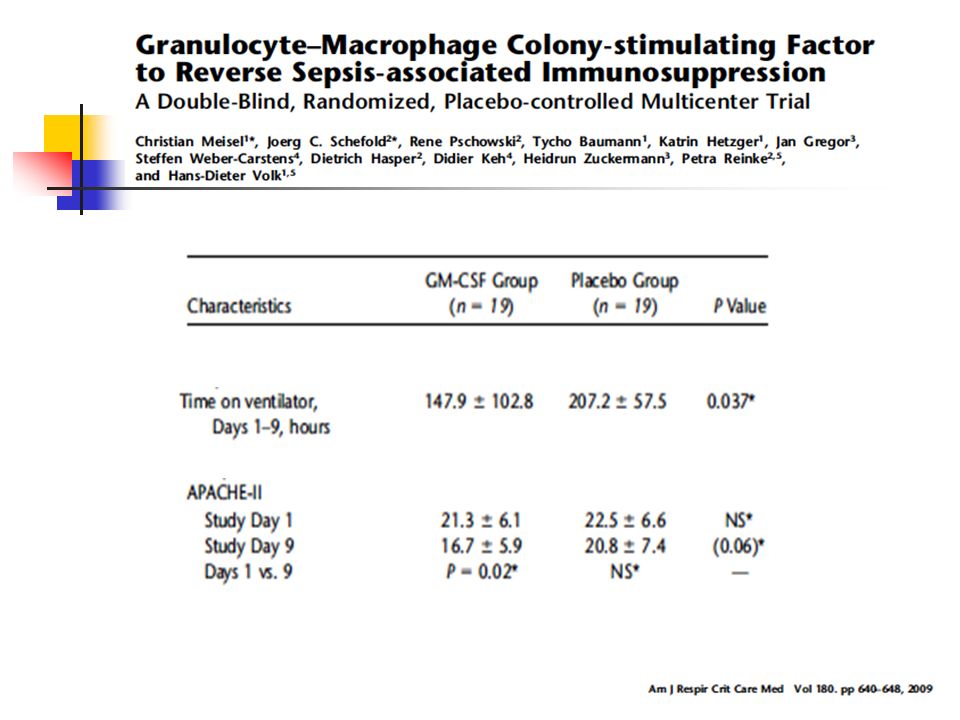
19 patients/group GM-CSF (4 mg/kg/d) or placebo for 8 days.
Rationale: Sustained sepsis-associated immunosuppression is associated with uncontrolled infection, multiple organ dysfunction, and death. Objectives: In the first controlled biomarker-guided immunostimulatory trial in sepsis, we tested whether granulocyte–macrophage colony-stimulating factor (GM-CSF) reverses monocyte deactivation, a hallmark of sepsis-associated immunosuppression (primary endpoint), and improves the immunological and clinical course of patients with sepsis. Methods: In a prospective, randomized, double-blind, placebo-controlled, multicenter trial, 38 patients (19/group) with severe sepsis or septic shock and sepsis-associated immunosuppression (monocytic HLA-DR [mHLA-DR] ,8,000 monoclonal antibodies (mAb) per cell for 2 d) were treated with GM-CSF (4 mg/kg/d) or placebo for 8 days. The patients’ clinical and immunological course was followed up for 28 days. Measurements and Main Results: Both groups showed comparable baseline mHLA-DR levels (5, ,628 vs. 5, ,332 mAb per cell), which significantly increased within 24 hours in the GM-CSF group. After GM-CSF treatment, mHLA-DR was normalized in 19/19 treated patients, whereas this occurred in 3/19 control subjects only (P , 0.001). GM-CSF also restored ex-vivo Toll-like receptor 2/4– induced proinflammatory monocytic cytokine production. In patients receiving GM-CSF, a shorter time of mechanical ventilation ( vs h, P ), an improved Acute Physiology and Chronic Health Evaluation-II score (P ), and a shorter length of both intrahospital and intensive care unit stay was observed (59633 vs and vs d, respectively, both not significant). Side effects related to the intervention were not noted. Conclusions: Biomarker-guided GM-CSF therapy in sepsis is safe and effective for restoring monocytic immunocompetence. Use of GMCSF may shorten the time of mechanical ventilation and hospital/ intensive care unit stay. A multicenter trial powered for the improvement of clinical parameters and mortality as primary endpoints seems indicated. Clinical trial registered
 reverses monocyte deactivation, a hallmark of sepsis-associated immunosuppression (primary. endpoint), and improves the immunological and clinical course of. patients with sepsis. Methods: In a prospective, randomized, double-blind, placebo-controlled, multicenter trial, 38 patients (19/group) with severe sepsis. or septic shock and sepsis-associated immunosuppression (monocytic. HLA-DR [mHLA-DR] ,8,000 monoclonal antibodies (mAb) per. cell for 2 d) were treated with GM-CSF (4 mg/kg/d) or placebo for. 8 days. The patients’ clinical and immunological course was followed. up for 28 days. Measurements and Main Results: Both groups showed comparable. baseline mHLA-DR levels (5, ,628 vs. 5, ,332 mAb per. cell), which significantly increased within 24 hours in the GM-CSF. group. After GM-CSF treatment, mHLA-DR was normalized in 19/19. treated patients, whereas this occurred in 3/19 control subjects only. (P , 0.001). GM-CSF also restored ex-vivo Toll-like receptor 2/4– induced proinflammatory monocytic cytokine production. In patients. receiving GM-CSF, a shorter time of mechanical ventilation. ( vs h, P ), an improved Acute Physiology. and Chronic Health Evaluation-II score (P ), and a shorter. length of both intrahospital and intensive care unit stay was. observed (59633 vs and vs d, respectively, both not significant). Side effects related to the intervention were. not noted. Conclusions: Biomarker-guided GM-CSF therapy in sepsis is safe and. effective for restoring monocytic immunocompetence. Use of GMCSF. may shorten the time of mechanical ventilation and hospital/ intensive care unit stay. A multicenter trial powered for the improvement. of clinical parameters and mortality as primary endpoints. seems indicated. Clinical trial registered.")
17
Etude prospective randomisée double aveugle
21 patients Etude prospective randomisée double aveugle The efficacy and safety of high-dose intravenous polyspecific immunoglobulin G (IVIG) as adjunctive therapy in streptococcal toxic shock syndrome (STSS) were evaluated in a multicenter, randomized, double-blind, placebo-controlled trial. The trial was prematurely terminated because of slow patient recruitment, and results were obtained from 21 enrolled patients (10 IVIG recipients and 11 placebo recipients). The primary end point was mortality at 28 days, and a 3.6-fold higher mortality rate was found in the placebo group. A significant decrease in the sepsis-related organ failure assessment score at days 2 (Pp.02) and 3 (Pp.04) was noted in the IVIG group. Furthermore, a significant increase in plasma neutralizing activity against superantigens expressed by autologous isolates was noted in the IVIG group after treatment (Pp.03).Although statistical significance was not reached in the primary end point, the trial provides further support for IVIG as an efficacious adjunctive therapy in STSS. NS
 as adjunctive therapy. in streptococcal toxic shock syndrome (STSS) were evaluated in a multicenter, randomized, double-blind, placebo-controlled trial. The trial was prematurely terminated because of slow patient recruitment, and results. were obtained from 21 enrolled patients (10 IVIG recipients and 11 placebo recipients). The primary end. point was mortality at 28 days, and a 3.6-fold higher mortality rate was found in the placebo group. A. significant decrease in the sepsis-related organ failure assessment score at days 2 (Pp.02) and 3 (Pp.04) was noted in the IVIG group. Furthermore, a significant increase in plasma neutralizing activity against. superantigens expressed by autologous isolates was noted in the IVIG group after treatment (Pp.03).Although. statistical significance was not reached in the primary end point, the trial provides further support for IVIG. as an efficacious adjunctive therapy in STSS. NS.")
18
Primary challenge Relapse
Clostridium difficile is the leading cause of nosocomial antibiotic-associated diarrhea, and recent outbreaks of strains with increased virulence underscore the importance of identifying novel approaches to treat and prevent relapse of Clostridium difficile-associated diarrhea (CDAD). CDAD pathology is induced by two exotoxins, toxin A and toxin B, which have been shown to be cytotoxic and, in the case of toxin A, enterotoxic. In this report we describe fully human monoclonal antibodies (HuMAbs) that neutralize these toxins and prevent disease in hamsters. Transgenic mice carrying human immunoglobulin genes were used to isolate HuMAbs that neutralize the cytotoxic effects of either toxin A or toxin B in cell-based in vitro neutralization assays. Three anti-toxin A HuMAbs (3H2, CDA1, and 1B11) could all inhibit the enterotoxicity of toxin A in mouse intestinal loops and the in vivo toxicity in a systemic mouse model. Four anti-toxin B HuMAbs (MDX-1388, , 1G10, and 2A11) could neutralize cytotoxicity in vitro, although systemic toxicity in the mouse could not be neutralized. Anti-toxin A HuMAb CDA1 and anti-toxin B HuMAb MDX-1388 were tested in the well-established hamster model of C. difficile disease. CDA1 alone resulted in a statistically significant reduction of mortality in hamsters; however, the combination treatment offered enhanced protection. Compared to controls, combination therapy reduced mortality from 100% to 45% (P < ) in the primary disease hamster model and from 78% to 32% (P < ) in the less stringent relapse model Primary challenge Relapse
. CDAD pathology is induced by two exotoxins, toxin A and toxin B, which have been shown to be cytotoxic and, in the case of toxin A, enterotoxic. In. this report we describe fully human monoclonal antibodies (HuMAbs) that neutralize these toxins and prevent. disease in hamsters. Transgenic mice carrying human immunoglobulin genes were used to isolate HuMAbs. that neutralize the cytotoxic effects of either toxin A or toxin B in cell-based in vitro neutralization assays. Three anti-toxin A HuMAbs (3H2, CDA1, and 1B11) could all inhibit the enterotoxicity of toxin A in mouse. intestinal loops and the in vivo toxicity in a systemic mouse model. Four anti-toxin B HuMAbs (MDX-1388, , 1G10, and 2A11) could neutralize cytotoxicity in vitro, although systemic toxicity in the mouse could. not be neutralized. Anti-toxin A HuMAb CDA1 and anti-toxin B HuMAb MDX-1388 were tested in the. well-established hamster model of C. difficile disease. CDA1 alone resulted in a statistically significant reduction. of mortality in hamsters; however, the combination treatment offered enhanced protection. Compared to. controls, combination therapy reduced mortality from 100% to 45% (P < ) in the primary disease. hamster model and from 78% to 32% (P < ) in the less stringent relapse model. Primary challenge. Relapse.")
19
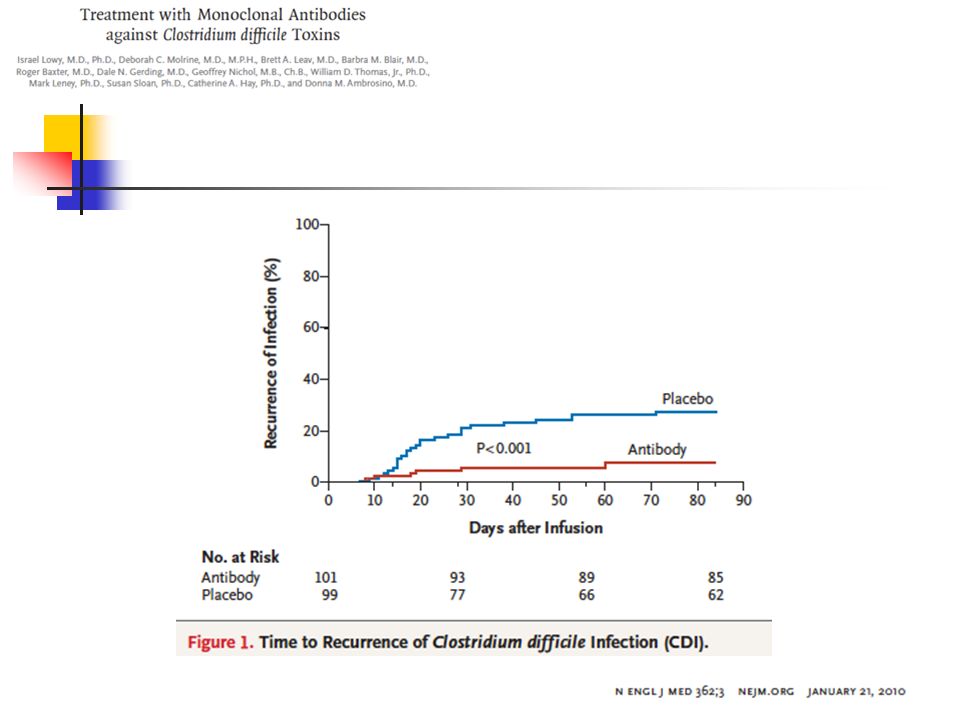
Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neu- tralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary out- come was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among pa- tients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P=0.06); among patients with more than one previous episode of C. difficile infection, recur- rence rates were 7% and 38%, respectively (P=0.006). The mean duration of the ini- tial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P=0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov num- ber, NCT )
 and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary out- come was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among pa- tients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P=0.06); among patients with more than one previous episode of C. difficile infection, recur- rence rates were 7% and 38%, respectively (P=0.006). The mean duration of the ini- tial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P=0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov num- ber, NCT )")
21
The combined administration of CDA1 and CDB1 human monoclonal antibodies in addition to antibiotics significantly reduced the recurrence of C. difficile infection.

22
TTSS: a needle Kubori et al. Science 1998

23
Surmortalité et SST III
Infection aiguë Infection chronique SSTT [+] 89% 41% SSTT [+] SSTT [-] Mortalité 21% 3% The ability of Pseudomonas aeruginosa to secrete specific toxins using the type III-mediated pathway has been reported. To determine the association of this phenotype with human illness, immunoblot analysis was used to detect expression of type III secretory proteins in P. aeruginosa isolates from respiratory tract or blood cultures of 108 consecutive patients. Relative risk of mortality was 6-fold greater with expression of the type III secretory proteins ExoS, ExoT, ExoU, or PcrV. Phenotype was independently correlated with toxicity in cellular and murine models. Prevalence of this phenotype was significantly higher in acutely infected patients than in chronically infected patients with cystic fibrosis. These results suggest that the type III protein secretion system is integral to increased P. aeruginosa virulence. A positive phenotype is a predictor of poor clinical outcome. In the future, such analyses may help distinguish potentially lethal infection from colonization and help determine appropriate therapy for critically ill patients. RR décès PcrV seule 7,4 PcrV + toxine(s) 8,7 (Roy Burman et al, J Infect Dis )
 8,7. (Roy Burman et al, J Infect Dis )")
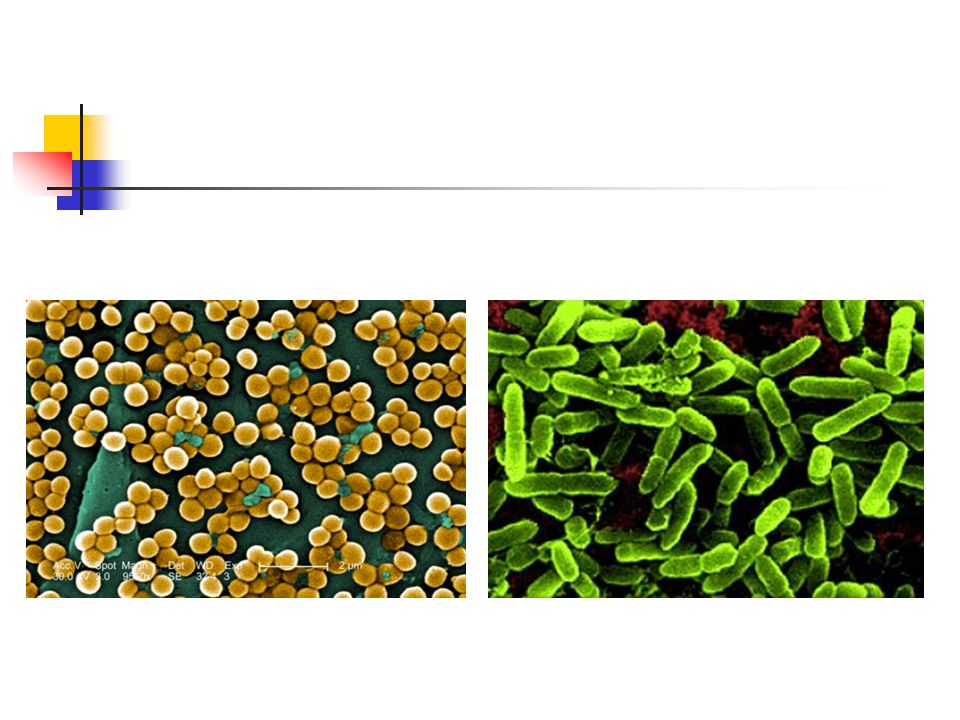
24
Pneumonie à P.aeruginosa
35 patients ventilés Pneumonie à P.aeruginosa Production de Protéines Issues du système de sécrétion de type III + 27/35 - 8/35 22 Sévère 5 Modérées 3 Sévères 5 Modérées (81%) (19%) (38%) (62%) ExoU : 10/35 (29%) associée à 90% de formes sévères Hauser et al, Crit Care Med 2002
 (19%) (38%) (62%) ExoU : 10/35 (29%) associée à 90% de formes sévères. Hauser et al, Crit Care Med")
25
Shime et al, J Immunol 2001 Les immunoglobulines polyclonales
L’administration d’immunoglobulines polyclonales 1 heure ou 4 heures après l’infection pulmonaire à P. aeruginosa est capable de diminuer la mortalité. Effect lié à la portion Fab. In a mouse survival study, the i.v. administration of anti-PcrV IgG after the airspace instillation of a lethal dose of P. aeruginosa resulted in the complete survival of the animals Shime et al, J Immunol 2001

27
Pseudomonas aeruginosa Cell Membrane TTSS
Membrane disruption and toxin injection into cell PcrV Protein Anti-PcrV Antibody (KB001)
")
28
“Overall, the human monoclonal antibody KBPA-101 was well tolerated over the entire dose range in healthy volunteers, and no serious adverse events have been reported.”

29
KB001 Trial Chastre et al ATS 2010

30
Chastre et al ATS 2010

31
Chastre et al ATS 2010

32
Chastre et al ATS 2010

33
A Phase I/II Randomized, Double-Blind, Placebo-Controlled, Single-Dose, Dose Escalation Study of KB001 in Cystic Fibrosis Patients Infected with Pseudomonas aeruginosa Milla, Carlos E; Accurso, Frank J.; Chmiel, James F.; McCoy, Karen S.; Billings, Joanne L; Atkinson, Jeffrey J; Clancy, John P; Liou, Theodore G; Acton, James D; Lynch, Susan V; Slusher, Nicole A; Burns, Jane L.; Mayer-Hamblett, Nicole; Harris, Kirk J; Patel, Rajesh; Tremblay, Thomas M; Parli, Teresa J. Twenty-seven subjects with a sputum Pa burden of >1 x 105 cfu/gm on screening and on stable CF therapy were randomized in dose-escalating cohorts to receive single IV infusions of placebo or KB001 at either 3 mg/kg or 10 mg/kg. Clinical, pharmacokinetic and immunogenicity outcomes were assessed. Pharmacodynamic endpoints included assessment of sputum microbial ecology and changes from baseline in Pa burden and inflammation ATS 2010

34
A Phase I/II Randomized, Double-Blind, Placebo-Controlled, Single-Dose, Dose Escalation Study of KB001 in Cystic Fibrosis Patients Infected with Pseudomonas aeruginosa Milla, Carlos E; Accurso, Frank J.; Chmiel, James F.; McCoy, Karen S.; Billings, Joanne L; Atkinson, Jeffrey J; Clancy, John P; Liou, Theodore G; Acton, James D; Lynch, Susan V; Slusher, Nicole A; Burns, Jane L.; Mayer-Hamblett, Nicole; Harris, Kirk J; Patel, Rajesh; Tremblay, Thomas M; Parli, Teresa J. ATS 2010

35
Vfr VqsR lasR lasI QscR RhlR RhlI RsaL RsaL LasR LasI RhlR RhlI PqsR
Activation Inhibition RsaL lasR lasI RsaL QscR LasR LasI C12 C12 PQS RhlR RhlI pqsH RhlR RhlI pqsR PqsR C4 C4 pqsA pqsB pqsC pqsD pqsE

36
QS Inhibition with macrolides
Elastase Insert = courbe de croissance A: courbe de croissance avec qté croissante d’azithro. La plus faible = 2 microg/ml Rhamnolipid Not bactericidal Not bacteriostatic QS Inhibition Tateda K et al. AAC 2001

37
no AZM (control) 2 g/ml AZM 4 g/ml AZM 8 g/ml AZM 12 g/ml AZM
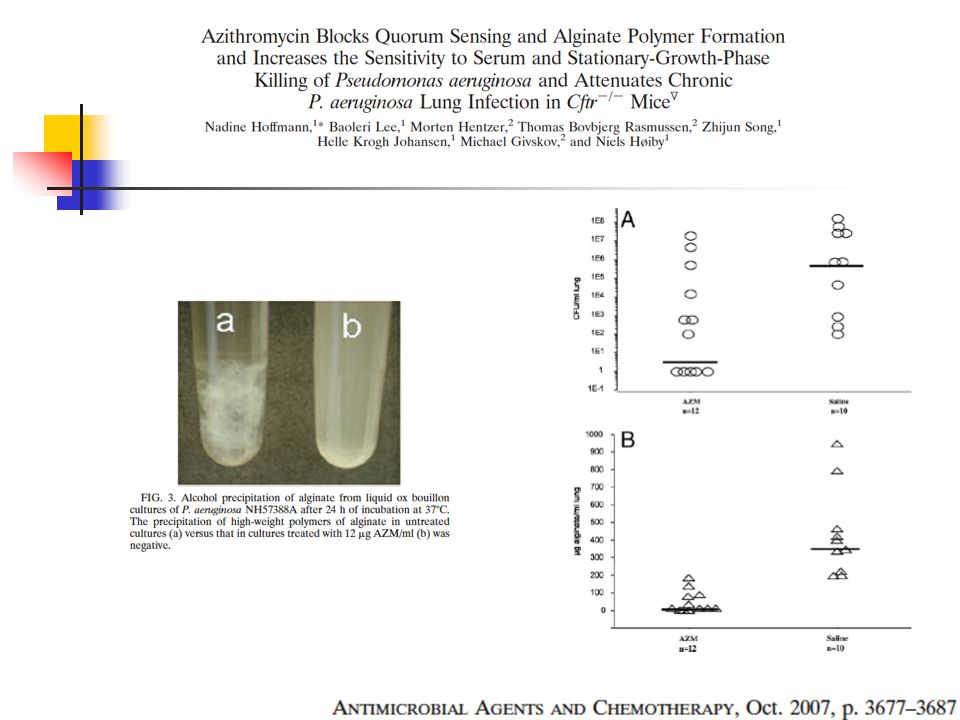
The consequences of O-acetylated alginate-producing Pseudomonas aeruginosa biofilms in the lungs of chronically infected cystic fibrosis (CF) patients are tolerance to both antibiotic treatments and effects on the innate and the adaptive defense mechanisms. In clinical trials, azithromycin (AZM) has been shown to improve the lung function of CF patients. The present study was conducted in accordance with previous in vitro studies suggesting that the effect of AZM may be the inhibition of alginate production, blockage of quorum sensing (QS), and increased sensitivity to hydrogen peroxide and the complement system. Moreover, we show that AZM may affect the polymerization of P. aeruginosa alginate by the incomplete precipitation of polymerized alginate and high levels of readily dialyzable uronic acids. In addition, we find that mucoid bacteria in the stationary growth phase became sensitive to AZM, whereas cells in the exponential phase did not. Interestingly, AZM-treated P. aeruginosa lasI mutants appeared to be particularly resistant to serum, whereas bacteria with a functional QS system did not. We show in a CF mouse model of chronic P. aeruginosa lung infection that AZM treatment results in the suppression of QS-regulated virulence factors, significantly improves the clearance of P. aeruginosa alginate biofilms, and reduces the severity of the lung pathology compared to that in control mice. We conclude that AZM attenuates the virulence of P. aeruginosa, impairs its ability to form fully polymerized alginate biofilms, and increases its sensitivity to complement and stationary-phase killing, which may explain the clinical efficacy of AZM. no AZM (control) 2 g/ml AZM 4 g/ml AZM 8 g/ml AZM 12 g/ml AZM
 patients are tolerance to both antibiotic treatments and effects on the innate and the. adaptive defense mechanisms. In clinical trials, azithromycin (AZM) has been shown to improve the lung function. of CF patients. The present study was conducted in accordance with previous in vitro studies suggesting that the. effect of AZM may be the inhibition of alginate production, blockage of quorum sensing (QS), and increased. sensitivity to hydrogen peroxide and the complement system. Moreover, we show that AZM may affect the polymerization. of P. aeruginosa alginate by the incomplete precipitation of polymerized alginate and high levels of. readily dialyzable uronic acids. In addition, we find that mucoid bacteria in the stationary growth phase became. sensitive to AZM, whereas cells in the exponential phase did not. Interestingly, AZM-treated P. aeruginosa lasI. mutants appeared to be particularly resistant to serum, whereas bacteria with a functional QS system did not. We. show in a CF mouse model of chronic P. aeruginosa lung infection that AZM treatment results in the suppression. of QS-regulated virulence factors, significantly improves the clearance of P. aeruginosa alginate biofilms, and. reduces the severity of the lung pathology compared to that in control mice. We conclude that AZM attenuates the. virulence of P. aeruginosa, impairs its ability to form fully polymerized alginate biofilms, and increases its sensitivity. to complement and stationary-phase killing, which may explain the clinical efficacy of AZM. no AZM (control) 2 g/ml AZM. 4 g/ml AZM. 8 g/ml AZM. 12 g/ml AZM.")
39
7 patients colonized by QS-proficient isolates
320 P. aeruginosa isolates and tracheal aspirates from 29 patients, six developed VAP (20%). 7 patients colonized by QS-proficient isolates 57% developed VAP as compared to 22 patients colonized by QS-deficient isolates 9% developed VAP (p = 0.018). Thorax Aug;65(8):703-1
. 7 patients colonized by QS-proficient isolates. 57% developed VAP as compared to. 22 patients colonized by QS-deficient isolates. 9% developed VAP (p = 0.018). Thorax Aug;65(8):")
40
With the rising development of bacterial resistance the search for new medical treatments beyond conventional antimicrobials has become a key aim of public health research. Possible innovative strategies include the inhibition of bacterial virulence. However, consideration must be given to the evolutionary and environmental consequences of such new interventions. Virulence and cooperative social behaviour of the bacterium Pseudomonas aeruginosa rely on the quorum-sensing (QS) controlled production of extracellular products (public goods). Hence QS is an attractive target for anti-virulence interventions. During colonization, non-cooperating (and hence less virulent) P. aeruginosa QS-mutants, benefiting from public goods provided by wild type isolates, naturally increase in frequency providing a relative protection from invasive infection. We hypothesized that inhibition of QS-mediated gene expression removes this growth advantage and selection of less virulent QS-mutants, and maintains the predominance of more virulent QS-wild type bacteria. We addressed this possibility in a placebo-controlled trial investigating the anti-QS properties of azithromycin, a macrolide antibiotic devoid of bactericidal activity on P. aeruginosa, but interfering with QS, in intubated patients colonized by P. aeruginosa. In the absence of azithromycin, non-cooperating (and hence less virulent) lasR (QS)-mutants increased in frequency over time. Azithromycin significantly reduced QS-gene expression measured directly in tracheal aspirates. Concomitantly the advantage of lasR-mutants was lost and virulent wild-type isolates predominated during azithromycin treatment. We confirmed these results in vitro with fitness and invasion experiments. Azithromycin reduced growth rate of the wild-type, but not of the lasR-mutant. Furthermore, the lasR-mutant efficiently invaded wild-type populations in the absence, but not in the presence of azithromycin. These in vivo and in vitro results demonstrate that anti-virulence interventions based on QS-blockade diminish natural selection towards reduced virulence and therefore may increase the prevalence of more virulent genotypes in the Hospital environment. More generally, the impact of intervention on the evolution of virulence of pathogenic bacteria should be assessed.
 controlled production of extracellular products (public goods). Hence QS is an attractive target for. anti-virulence interventions. During colonization, non-cooperating (and hence less virulent) P. aeruginosa QS-mutants, benefiting from public goods provided by wild type isolates, naturally increase in frequency providing a relative protection. from invasive infection. We hypothesized that inhibition of QS-mediated gene expression removes this growth advantage. and selection of less virulent QS-mutants, and maintains the predominance of more virulent QS-wild type bacteria. We. addressed this possibility in a placebo-controlled trial investigating the anti-QS properties of azithromycin, a macrolide. antibiotic devoid of bactericidal activity on P. aeruginosa, but interfering with QS, in intubated patients colonized by P. aeruginosa. In the absence of azithromycin, non-cooperating (and hence less virulent) lasR (QS)-mutants increased in. frequency over time. Azithromycin significantly reduced QS-gene expression measured directly in tracheal aspirates. Concomitantly the advantage of lasR-mutants was lost and virulent wild-type isolates predominated during azithromycin. treatment. We confirmed these results in vitro with fitness and invasion experiments. Azithromycin reduced growth rate of. the wild-type, but not of the lasR-mutant. Furthermore, the lasR-mutant efficiently invaded wild-type populations in the. absence, but not in the presence of azithromycin. These in vivo and in vitro results demonstrate that anti-virulence. interventions based on QS-blockade diminish natural selection towards reduced virulence and therefore may increase the. prevalence of more virulent genotypes in the Hospital environment. More generally, the impact of intervention on the. evolution of virulence of pathogenic bacteria should be assessed.")
41
erythema ⁄inflammation, ulceration ⁄ granulation ⁄ polyps,
- Physician erythema ⁄inflammation, ulceration ⁄ granulation ⁄ polyps, discharge quantity, discharge type and odour Patients Discomfort, itchiness, wetness, smell Objectives: To evaluate the efficacy and safety of a therapeutic bacteriophage preparation (Biophage-PA) targeting antibiotic-resistant Pseudomonas aeruginosa in chronic otitis. Design: Randomised, double-blind, placebo-controlled Phase I/II clinical trial approved by UK Medicines and Healthcare products Regulatory Agency (MHRA) and the Central Office for Research Ethics Committees (COREC) ethical review process. Setting: A single specialist university hospital. Participants: 24 patients with chronic otitis with a duration of several years (2–58). Each patient had, at the time of entry to the trial, an ear infection because of an antibiotic- resistant P. aeruginosa strain sensitive to one or more of the six phages present in Biophage-PA. Participants were randomised in two groups of 12 treated with either a single dose of Biophage-PA or placebo and followed up at 7, 21 and 42 days after treatment by the same otologist. Ears were thoroughly cleaned on each occasion and clinical and microbiological indicators measured. Main outcome measures: Physician assessed erythema ⁄inflammation, ulceration ⁄ granulation ⁄ polyps, discharge quantity, discharge type and odour using a Visual Analogue Scale (VAS). Patients reported discomfort, itchiness, wetness and smell also using a VAS. Bacterial levels of P. aeruginosa and phage counts from swabs were measured initially and at follow-up. At each visit patients were asked about side effects using a structured form. Digital otoscopic images were obtained on days 0 and 42 for illustrative purposes only. Results: Relative to day 0, pooled patient- and physician- reported clinical indicators improved for the phage treated group relative to the placebo group. Variation from baseline levels was statistically significant for combined data from all clinic days only for the phage treated group. Variation from baseline levels was statistically significant for the majority of the patient assessed clinical indicators only for the phage treated group. P. aeruginosa counts were significantly lower only in the phage treated group. No treatment related adverse event was reported. Conclusion: The first controlled clinical trial of a therapeutic bacteriophage preparation showed efficacy and safety in chronic otitis because of chemo-resistant P. aeruginosa.
 targeting. antibiotic-resistant Pseudomonas aeruginosa in chronic. otitis. Design: Randomised, double-blind, placebo-controlled. Phase I/II clinical trial approved by UK Medicines and. Healthcare products Regulatory Agency (MHRA) and the. Central Office for Research Ethics Committees (COREC) ethical review process. Setting: A single specialist university hospital. Participants: 24 patients with chronic otitis with a duration. of several years (2–58). Each patient had, at the time. of entry to the trial, an ear infection because of an antibiotic- resistant P. aeruginosa strain sensitive to one or more. of the six phages present in Biophage-PA. Participants. were randomised in two groups of 12 treated with either. a single dose of Biophage-PA or placebo and followed up. at 7, 21 and 42 days after treatment by the same otologist. Ears were thoroughly cleaned on each occasion and. clinical and microbiological indicators measured. Main outcome measures: Physician assessed. erythema ⁄inflammation, ulceration ⁄ granulation ⁄ polyps, discharge quantity, discharge type and odour using a. Visual Analogue Scale (VAS). Patients reported discomfort, itchiness, wetness and smell also using a VAS. Bacterial levels of P. aeruginosa and phage counts from. swabs were measured initially and at follow-up. At each. visit patients were asked about side effects using a. structured form. Digital otoscopic images were obtained. on days 0 and 42 for illustrative purposes only. Results: Relative to day 0, pooled patient- and physician- reported clinical indicators improved for the phage. treated group relative to the placebo group. Variation. from baseline levels was statistically significant for. combined data from all clinic days only for the phage. treated group. Variation from baseline levels was. statistically significant for the majority of the patient. assessed clinical indicators only for the phage treated. group. P. aeruginosa counts were significantly lower only. in the phage treated group. No treatment related adverse. event was reported. Conclusion: The first controlled clinical trial of a. therapeutic bacteriophage preparation showed efficacy. and safety in chronic otitis because of chemo-resistant. P. aeruginosa.")
42
2h pi Preventive 4d

43
Microbiote

44
Sekirov, 2010

45
Spécifique de chaque individu
14 sujets sains Spécifique de chaque individu Zoetendal, 1998

46
Probiotiques Terme introduit en 1953 par Werner Kollath
Par opposition aux antibiotiques Ce sont des facteurs microbiens qui stimulent la croissance d’autres microorganismes. La nécessité du caractère vivant des souches est ajouté à la définition par Roy Fuller en 1989.

47
Probiotiques Alfred Nissle
Isolement en 1917 d’une souche de E. coli à partir de selles d’un soldat qui, lors d’une épidémie de Shigellose, n’a pas développé d’entérocolite. Utilisation de sa souche avec succès dans des cas de Salmonellose et Shigellose [Nissle 1959].

48
Essais contrôlés et diarrhée post-antibiotique
D’Souza 2002 BMJ Cremonini Aliment Pharmocol Ther Szajewska 2005 Hawrelak Digestion Adulte Szajewska 2006 J Pediatr Johnston CMAJ 2007 Cochrane Database Syst Rev. Enfant Efficacité modérée des probiotiques à prévenir la diarrhée post-ATB S. boulardii ou L. rhamnosus GG chez l’enfant L. casei DN chez la personne âgée Pb dans la définition de la diarrhée et de la gravité clinique

49
Essais contrôlés et colite à Clostridium difficile
Lewis 2007 Am J Gastroenterol Pour Dendukuri 2005 CMAJ Contre Difficulté à discerner prévention et traitement au moment de la colite

50
Ampicillin (1 g/L), vancomycin (500 mg/L), neomycin sulfate (1 g/L), and metronidazole (1 g/L) in drinking water for 4 wk before PR8 virus infection (10 pfu per mouse). Antibiotic-treated mice fail to induce acquired immunity to influenza virus infection. C57BL/6 mice were given ampicillin (1 g/L), vancomycin (500 mg/L), neomycin sulfate (1 g/L), and metronidazole (1 g/L) in drinking water for 4 wk before PR8 virus infection (10 pfu per mouse). Two weeks later, serum and nasal wash were collected and Ag-specific antibody titers were measured (A), and T-cells were isolated from spleen and restimulated with flu virion or NP peptide for 72 h, and IFN-γ production from CD4 T cells (B) and CD8 T cells (C) was measured. (D) Lymphocytes were collected from the lung of infected animals at 14 d postinfection and stained with flu-specific tetramer. (E) The lung washes of flu-infected mice were harvested at 9 d postinfection, and viral titers were measured by plaque assay. *P < 0.05 and ***P < vs. water-fed group. Data represent the mean ± SD. Similar results were obtained from three separate experiments Proc Natl Acad Sci USA 2011
, vancomycin (500 mg/L), neomycin sulfate. (1 g/L), and metronidazole (1 g/L) in drinking water for 4 wk. before PR8 virus infection (10 pfu per mouse). Two weeks. later, serum and nasal wash were collected and Ag-specific. antibody titers were measured (A), and T-cells were isolated. from spleen and restimulated with flu virion or NP peptide. for 72 h, and IFN-γ production from CD4 T cells (B) and CD8 T. cells (C) was measured. (D) Lymphocytes were collected from. the lung of infected animals at 14 d postinfection and stained. with flu-specific tetramer. (E) The lung washes of flu-infected. mice were harvested at 9 d postinfection, and viral titers were. measured by plaque assay. *P < 0.05 and ***P < vs. water-fed group. Data represent the mean ± SD. Similar. results were obtained from three separate experiments. Proc Natl Acad Sci USA")
51
Greffe de flore….. Bakken et al, Anaerobe 2009

Présentations similaires














2009 population and high risk group vaccination coverage during the 2009-2010 pandemic, France ESCAIDE Lisbon, 11-13 November 2010.>")
 / Information about the study trip to Strasbourg (29th-31st March 2009) Château de.>")





