Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Actualités des traitements ARV: du Sud au Nord Pierre-Marie Girard IMEA & Hôpital ST Antoine DU IMEA FOURNIER PARIS VII Novembre 2009 Partie I

2
Les Cohortes au SUD

3
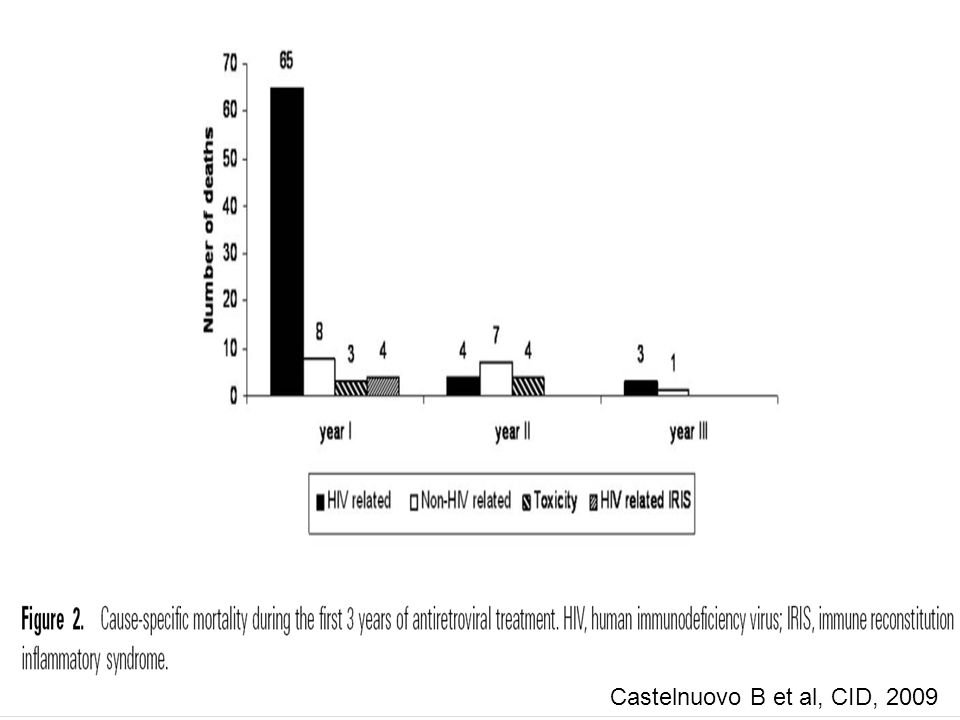
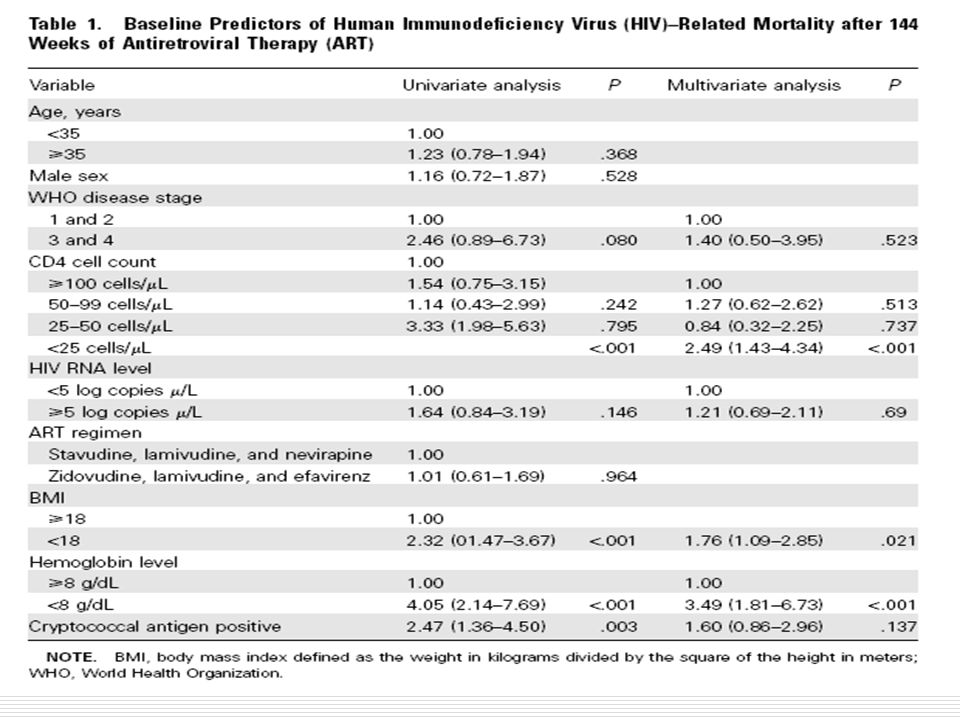
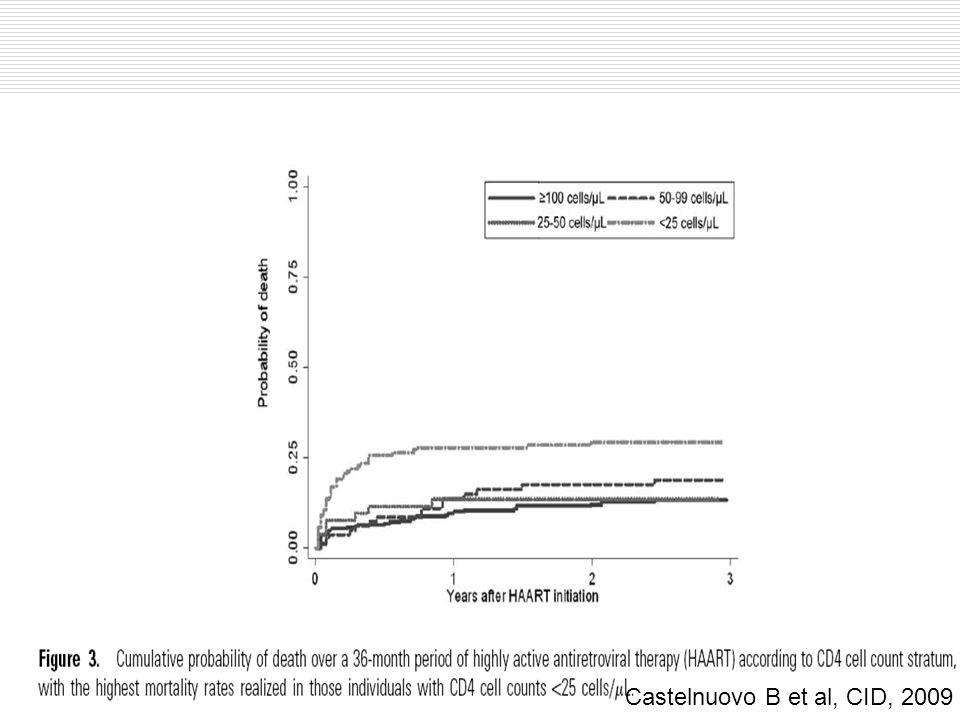
Castelnuovo B et al, CID, 2009

8
Second Line ARV in adults and children Renaud-Théry F, AIDS 2007

9
Cumulative proportion of patients needing 2 nd Line ARV Switch to 2d Line: mean 3% per year Renaud-Théry F, AIDS 2007

10
AIDS, 2009

11
Low performance of WHO criteria for the diagnosis of virological failure

12
CID, 2009

18
Smith AD et al, Lancet, 2009

21
Essais au SUD Essai DART « Big-Dart » REYADAK à Dakar« Small is beautiful » Essais PTME et Pédiatrie « Hit hard, hit early »

22
IAS July 2009 MRC/UVRI Uganda Research Unit on AIDS, Entebbe, Uganda TASO, Uganda University of Zimbabwe, Harare, Zimbabwe Joint Clinical Research Centre, Kampala, Uganda Infectious Diseases Institute, Makerere University, Uganda MRC Clinical Trials Unit, UK Imperial College, UK DFID, UK GlaxoSmithKline Gilead Sciences Boehringer-Ingelheim Abbott Rockefeller Foundation MRC, UK DART partners Support:

23
IAS July 2009 Survival 0.90 0.87 0.08 0.92 0.90 0.18 0.95 0.94 0.55 012345 0.0 0.2 0.4 0.6 0.8 1.0 Proportion alive Years from enrolment Entebbe Cohort (Uganda): pre-ART 1996- 2000, median CD4 75 at enrolment: 57.7/100 PY DART LCM:2.2/100 PY CDM:2.9/100 PY
: pre-ART , median CD4 75 at enrolment: 57.7/100 PY DART LCM:2.2/100 PY CDM:2.9/100 PY")
24
IAS July 2009 Resource allocation 6.7 million adults and children in Sub-Saharan Africa were estimated to need ART in December 2007 –only 2.2 million were receiving ART Global economic crisis is threatening programme funding Using DART to help resource allocation –what could be achieved in an ART programme with $1,000,000 over 5 years...

25
IAS July 2009 21 271 35 366 0 100 200 300 400 Number of patients LCM: TREAT 292CDM: TREAT 401 (extra 109) treated, alivetreated, died For $1,000,000 over 5 years Mean cost/patient: LCM $3,425, CDM $2,493 Assuming cost of patients not treated is $0. Based on difference in life-years from CEA.

26
IAS July 2009 Survival 0.90 0.87 0.08 0.92 0.90 0.18 0.95 0.94 0.55 012345 0.0 0.2 0.4 0.6 0.8 1.0 Proportion alive Years from enrolment Entebbe Cohort: pre-ART 1996- 2000, median CD4 75 at enrolment: 57.7/100 PY DART LCM:2.2/100 PY CDM:2.9/100 PY

27
IAS July 2009 36 73 21 271 35 366 0 100 200 300 400 Number of patients LCM: TREAT 292CDM: TREAT 401 (extra 109) treated, alivetreated, died not treated, diednot treated, alive For $1,000,000 over 5 years Mean cost/patient: LCM $3,425, CDM $2,493 Total deaths 94 from Entebbe Cohort data Total deaths 35 Assuming cost of patients not treated is $0. Based on difference in life-years from CEA.

28
IAS July 2009 11 23 26 341 35 366 0 100 200 300 400 Number of patients LCM: TREAT 367CDM: TREAT 401 (extra 34) Excluding routine toxicity tests in LCM Mean cost/patient: LCM $2,726, CDM $2,493 Total deaths 49 treated, alivetreated, died not treated, diednot treated, alive from Entebbe Cohort data Total deaths 35 Assuming cost of patients not treated is $0. Based on difference in life-years from CEA.

29
Impact of « not-switching » on survival Risk of death Switching pts vs no Switching = 3.3 [1.6-6.8]Ive P et al, CROI, 2009
![Impact of « not-switching » on survival Risk of death Switching pts vs no Switching = 3.3 [ ]Ive P et al, CROI, 2009](http://images.slideplayer.fr/2/504623/slides/slide_29.jpg "Impact of « not-switching » on survival Risk of death Switching pts vs no Switching = 3.3 [ ]Ive P et al, CROI, 2009")
30
Impact of « not-switching » on survival Risk of death Switching pts vs no Switching = 3.3 [1.6-6.8]Ive P et al, CROI, 2009
![Impact of « not-switching » on survival Risk of death Switching pts vs no Switching = 3.3 [ ]Ive P et al, CROI, 2009](http://images.slideplayer.fr/2/504623/slides/slide_30.jpg "Impact of « not-switching » on survival Risk of death Switching pts vs no Switching = 3.3 [ ]Ive P et al, CROI, 2009")
32
Evaluation of didanosine/lamivudine and atazanavir QD first line regimen in HIV-1 infected adults in Senegal IMEA 031 trial 0 20 40 60 80 100 BL412243648 Weeks % VL < 400 c/ml % VL < 50 c/ml % 0 20 40 60 80 100 BL412243648 Weeks % VL < 400 c/ml % VL < 50 c/ml % 0 20 40 60 80 100 BL412243648 Weeks % VL < 400 c/ml % VL < 50 c/ml % 0 20 40 60 80 100 BL412243648 Weeks % VL < 400 c/ml % VL < 50 c/ml % 0 20 40 60 80 100 BL412243648 Weeks % VL < 400 c/ml % VL < 50 c/ml %

33
Les Cohortes au Nord

35
Nature 2009 Hunt, JID 2009

37
Les Essais au Nord

38
Stratégies abandonnées Traitement tardif (< 200/mm3) Combinaisons initiales: En quadrithérapie IN+INN+IP En épargne de nucléosidiques par IP+INN ?? Traitements intermittents à cycles longs Interruptions programmées chez patients avec CD4 < 500/mm3 Initiation par nucléosidiques seuls Intensification simple (« Add on ») Immunothérapie non spécifique par IL2 Vaccinothérapie avec candidats-vaccins actuels
 Immunothérapie non spécifique par IL2 Vaccinothérapie avec candidats-vaccins actuels.")
39
Premières lignes dARV

40
Première ligne: IP vs NNRTI

41
EFV vs LPV/r chez les patients naïfs à CD4+ < 200 : HIV-1 RNA <50 copies/mL à S48 0 20 80 100 016 32 48 Week 82440 Efavirenz (n = 95) LPV/RTV (n = 94) Nombre de Pts avec ARN VIH < 50 copies/mL EFV 29 70 68 67 LPV 8 53 56 50 70.5% 53.2% 0 20 40 60 80 100 HIV-1 RNA < 50 copies/mL (%) 79% 49% 64% 57% P = 0.012 P = 0.15 EFV LPV/ RTV n = 42 45 53 49 50 cell/mm 3 > 50 cell/mm 3 EFV supérieur à LPV/RTV: Δ 17% (CI 95%: 3.5% to 31.0%; P =.017) HIV-1 RNA < 50 copies/mL (%) Selon les CD4 à BL 60 40 Madero JS, et al. IAC 2008. Abstract TUAB0104.

44
Patients naïfs: Etudes en cours ou prochaines avec molécules disponibles MERIT: CBV+EFV vs CBV+MVC COL11429: ABC/3TC + RAL APILOT-1:TDF/FTC+rATV vs rATV+MVC NEAT: TDF/FTC+rDRV vs RAL+rDRV CCTG589: rLPV+RAL vs Atripla ACTG A5262: rDRV+RAL Inv08: rLPV+RAL Merck072 RADAR: rDRV+RAL vs TDF/FTC+rDRV ANRS Optimal:Haart vs Haart + MVC chez pts CD4<200 A009: TDF/FTC + rLPV vs TDF/FTC+RAL M10-336 PROGRESS: TDF/FTC+ rLPV vs TDF/FTC+RAL GS001: TDF/FTC + rLPV vs TDF/FTC+RAL RAN: TDF/FTC + RAL vs TDF/FTC+rATV AI 424-376: TDF/FTC+rATV vs RAL+ATV bid ADARC 07-01: TDF/FTC+rATV ±RAL/MVC lors PI ANRS Optiprim: TDF/FTC+rDRV+RAL+MVC vs TDF/FTC+rDRV lors PI ClinicalTrials.gov

Présentations similaires
















 vs EFV Etude MERIT.>")



 and associated factors in HIV-infected patients,>")

