Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
VACCIN HAEMOPHILUS HiB
Cours International français de Vaccinologie CIFV 2014 Philippe REINERT Créteil Paris XII

2
Caractéristiques des souches d’H. influenzae
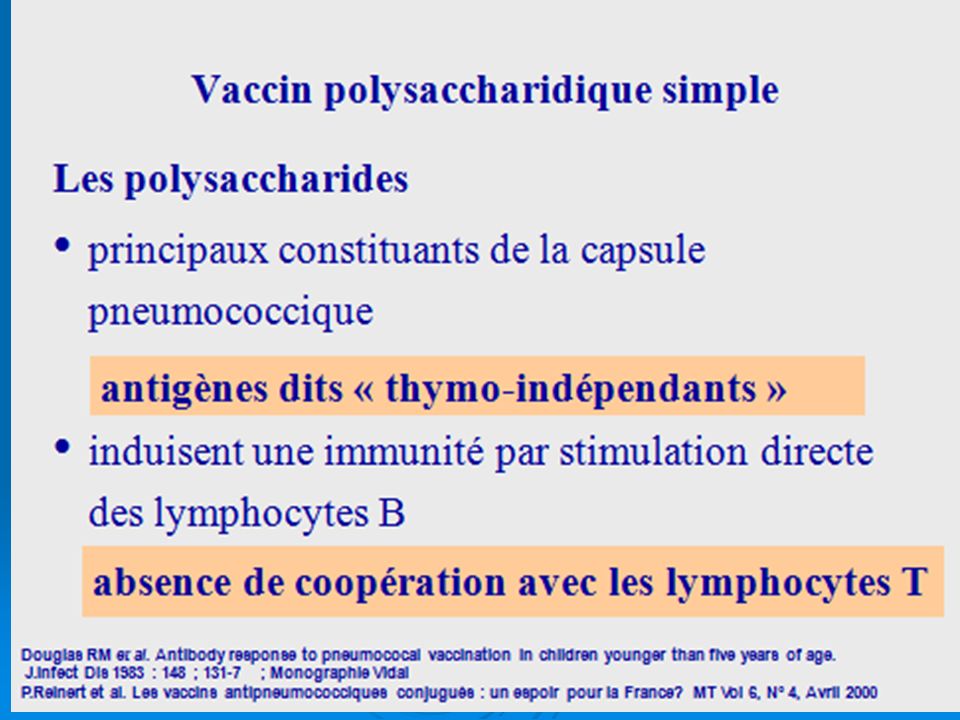
Non capsulé Infections locales Haemophilus influenzae Type a, c, d, e, f Rare Capsulé INFECTIONS INVASIVES Méningite pneumonie épiglottite septicémie chez les jeunes enfants de moins de 5 ans H.influenzae STRAIN CHARACTERISTICS 95% of invasive H. influenzae infections are due to Hib. Majority of invasive Hib infections occur before the age of 5 years, particularly in infants. Non capsulated strains are mainly responsible for localized and non invasive infections. Invasive infections due to other types than type b are rare. H. influenzae is a non specific microorganism: it causes various invasive infections which also might be caused by other pathogens. These infections are all medical emergencies. Hib might also cause localized infections such as otitis media or conjunctivis but these are not common. References: 2 WHO. Position paper on Hib vaccines. WHO web site: 4 Plotkin S. Haemophilus influenzae vaccines. VACCINES, 3rd edition. 1999; Type b Plotkin S. Vaccine, 3rd ed. 1999; OMS, “Position Paper” sur les vaccins Hib

3
Caractéristiques des souches
AGE CIBLE POUVOIR PATHOGENE Capsulée Infections invasives méningite, pneumonie septicémie, épiglottite Jeunes enfants 95% moins de 5 ans type b Capsulées types a, c, d, e, f Jeunes enfants Infections invasives mais rares H.influenzae STRAIN CHARACTERISTICS 95% of invasive H. influenzae infections are due to Hib. Majority of invasive Hib infections occur before the age of 5 years, particularly in infants. Non capsulated strains are mainly responsible for localized and non invasive infections. Invasive infections due to other types than type b are rare. H. influenzae is a non specific microorganism: it causes various invasive infections which also might be caused by other pathogens. These infections are all medical emergencies. Hib might also cause localized infections such as otitis media or conjunctivis but these are not common. References: 2 WHO. Position paper on Hib vaccines. WHO web site: 4 Plotkin S. Haemophilus influenzae vaccines. VACCINES, 3rd edition. 1999; Infections locales : bronchite, otite, sinusite, conjonctivite Enfants Adultes Non capsulées Plotkin S. Vaccine, 3rd ed. 1999; OMS, “Position Paper” sur les vaccins Hib

4
Transmission et portage
Transmission par les sécrétions respiratoires Portage le plus souvent asymptomatique Concerne 3 à 5 % des enfants Jusqu’à 50 % des enfants dans les populations vivant en promiscuité La forte concentration des sujets porteurs conduit à une probabilité plus élevée de maladie invasive TRANSMISSION AND CARRIAGE Before infection, Hib is first found in the upper respiratory tract Hib carriage is most of the times asymptomatic Hib transmission is easy (with salivary secretions and droplets) High carriage rate is associated with a higher probability of invasive disease. Carriage rates are low under the age of 6 months of life and reach a maximum between 3 and 5 years. In crowded conditions, or Hib disease in a closed population, carriage rate may be substantially higher Référence: 6 Barbour et al. Conjugate vaccines and the carriage of Haemophilus influenzae type b. Emerg Infect Dis, 1996; 2(3): Barbour. Em Inf Dis, 1996, 2 (3):
 High carriage rate is associated with a higher probability of invasive disease. Carriage rates are low under the age of 6 months of life and reach a maximum between 3 and 5 years. In crowded conditions, or Hib disease in a closed population, carriage rate may be substantially higher. Référence: 6 Barbour et al. Conjugate vaccines and the carriage of Haemophilus influenzae type b. Emerg Infect Dis, 1996; 2(3): Barbour. Em Inf Dis, 1996, 2 (3):")
5
MENINGITE à HiB Installation progressive+++ -fièvre -céphalées
-vomissements -photophobie -irritabilité+troubles du sommeil RAIDEUR DE LA NUQUE DIFFICULTE D’UN DIAGNOSTIC PRECOCE

6
PNEUMOPATHIES Fièvre élevée Polypnée Toux++
Radiologie: foyer systématisé images diffuses

7
AUTRES LOCALISATIONS Epiglottite ( 2 à 7 ans) Dyspnée laryngée majeure
Aggravée par le décubitus Mortalité:élevée Arthrites Cellulites Pleurésies

8
ANTIBIOTHERAPIE Ampicilline, AMOXICILLINE Chloramphénicol
Céphalosporines de 3ème génération Résistance à l’AMOXICILLINE de plus en plus fréquente

9
IMMUNITE NATURELLE (Enfants - 1990) (%) (%) (n = 290) (mois) 100 25 80
20 60 15 Incidence de la méningite à Hib 40 10 % d'anticorps 20 5 (mois) 0 à 2 2 à 4 4 à 6 6 à 8 > 48 8 à 10 10 à 12 12 à 18 18 à 24 24 à 48 Tall F. et coll., Arch Pédiatr. (1994) 1, 1
 0 à 2. 2 à 4. 4 à 6. 6 à 8. > à à à à à 48. Tall F. et coll., Arch Pédiatr. (1994) 1,")
10
IMMUNITE NATURELLE AU BURKINA FASO
(Enfants ) Chaque mère est protégée Les enfants âgés de 12 à 24 mois ne sont pas protégés Incidence de la méningite à Hib Enfants de moins de 5 ans : 61,5 / Enfants de moins d'1 an : 239,2 / Tall F. et coll., Arch Pédiatr. (1994) 1, 2
 Chaque mère est protégée. Les enfants âgés de 12 à 24 mois ne sont pas protégés. Incidence de la méningite à Hib. Enfants de moins de 5 ans : 61,5 / Enfants de moins d 1 an : 239,2 / Tall F. et coll., Arch Pédiatr. (1994) 1,")
11
Pathogénécité Méningite Epiglottite Arthrite Ostéomyélite Cellulite
Colonisation pharyngée Bactériémie Barrière hémato-méningée SNC Sang Pharynx Hib Réponse bactéricide Méningite Elimination des souches non capsulées d’H. influenzae PHYSIOPATHOLOGY Colonization is the result of adherence to nasopharyngeal epithelial cells and systemic infection is the result of the invasion of pharyngeal epithelium. The capsule, made up of PRP, is FUNDAMENTAL to the Hib virulence: it protects Hib against phagocytosis by polynuclear neutrophils and macrophages. it enables Hib to develop in blood and cause invasive infections (always secondary to Hib bacteremia). Invasive disease occurs when no antibody response is observed (young age, or any other risk factor), and can result in meningitis, osteomyelitis, cellulitis… Meningitis occurs when bacteremia is > 105/ml blood. Reference: 5 Borderon. Haemophilus influenzae : colonisation et infection. Arch Pediatr, 1995; 2 (3): protection capsulaire du PRP Poumons Epiglottite Arthrite Ostéomyélite Cellulite pneumonie Borderon JC, Arch de Ped, 1995; 2(3) :
. Invasive disease occurs when no antibody response is observed (young age, or any other risk factor), and can result in meningitis, osteomyelitis, cellulitis… Meningitis occurs when bacteremia is > 105/ml blood. Reference: 5 Borderon. Haemophilus influenzae : colonisation et infection. Arch Pediatr, 1995; 2 (3): protection capsulaire du PRP. Poumons. Epiglottite. Arthrite. Ostéomyélite. Cellulite. pneumonie. Borderon JC, Arch de Ped, 1995; 2(3) :")
12
Facteurs de risque HOTE ENVIRONNEMENT Age Fréquentation d’une garderie
Taille du foyer ou promiscuité Statut socio-économique HOTE Age Absence d’allaitement Maladie sous-jacente Facteurs génétiques Ethnicité Antécédent d’infection RISK FACTORS Age: The most important epidemiological feature of invasive Hib disease is the age related risk. In populations with a high incidence of disease, the age incidence is shifted to younger children. Case control studies have proven that breast-feeding is associated with reduced risk of disease. Although the mechanism is unknown, it may be the result of immune factors present in human milk. Race and ethnicity : high incidence has been described in Native American populations or between caucasians and afro-americans. But the hypothesis that these differences in incidence are due to genetically determined differences is unproven. Underlying disease : several hematological and immunological disorders are associated with increased risk for Hib disease. An antecedent of viral respiratory infection could alter mucosal immunity but difficulties in conducting propsective studies with appropriate controls have made it difficult to verify this hypothesis. Socioeconomic factors : the interplay of factors that affect exposure to Hib organism : large household size, crowding, increased population density or others, such as low familly income or low parental education level. Reference: 4 Plotkin S. Haemophilus influenzae vaccines. VACCINES, 3rd edition. 1999; AGENT Infectiosité Capacité invasive Virulence Plotkin S. Vaccine, 3rd ed. 1999;

13
Méningite à Hib / 100.000 enfants < 5 ans
Taux d’incidence Hib Méningite à Hib / enfants < 5 ans 530 32 8-27 10 40-60* 5-43** 16-31 HIB INCIDENCE RATE Invasive Hib disease occurs endemically and is not reliably reported nationally. Nevertheless, a number of population-based studies conducted during the past 30 years have made it possible to define the incidence. The isolation of Hib from a sterile body site is the basis for case detection. But not all the children have cultures performed or culture may be negative owing to prior antimicrobial therapy. For these reasons, even the most carefully conducted surveillance study inevitably underestimates the true incidence of disease. Variations usually are smaller within than between regions. No estimates are avaible from India or China or from newly independent states of the former Soviet Union. In Asia, data are available only from the wealthier countries. Epidemiological studies are currently ongoing References: 3 Salisbury. Summary statement: the first international conference on Haemophilus influenzaae type b in Asia. Ped J Infect Dis, 1998; 17 (9), Suppl: S93-S95. 4 Plotkin S. Haemophilus influenzae vaccines. VACCINES, 3rd edition. 1999; 33 Levine. Pediatr Infect Dis J, 1998, 17 (Suppl): S95-113 29 Peltola et al. Haemophilus influenzae type b disease and vaccination in Latin America and the Caribbean. PIDJ 1997; 16(8): 780-7 50-60 35 25* Levine et Al., PIDJ 1998; 17(9) : S95-113 Salisbury et Al., PIDJ 1998; 17(9) : S93-95 Plotkin, Vaccine, 3rd ed. 1999 Peltola, PIDJ 1997; 16(8) : 780-7 * populations autochtones = 150 à 250 ** En Asie, le taux est difficile à estimer
, Suppl: S93-S95. 4 Plotkin S. Haemophilus influenzae vaccines. VACCINES, 3rd edition. 1999; Levine. Pediatr Infect Dis J, 1998, 17 (Suppl): S Peltola et al. Haemophilus influenzae type b disease and vaccination in Latin America and the Caribbean. PIDJ 1997; 16(8): * Levine et Al., PIDJ 1998; 17(9) : S Salisbury et Al., PIDJ 1998; 17(9) : S Plotkin, Vaccine, 3rd ed Peltola, PIDJ 1997; 16(8) : * populations autochtones = 150 à 250. ** En Asie, le taux est difficile à estimer.")
14
Épidémiologie d'Haemophilus influenzae de type B MENINGITE AU BURKINA FASO
(Enfants < 15 ans à 1990) Pneumocoque Hib Méningocoque Autres (n = 514) CONSEQUENCES 40 % 10 % 4 % Séquelles graves Décès Pneumocoque 55,0 % 5,1 % Hib 21,7 % 14,1 % Méningocoque 17,0 % 0,0 % 47 % Tall F. et coll. Méd. Mal. Infect ; 22 : 3
 Pneumocoque. Hib. Méningocoque. Autres. (n = 514) CONSEQUENCES. 40 % 10 % 4 % Séquelles graves. Décès. Pneumocoque. 55,0 % 5,1 % Hib. 21,7 % 14,1 % Méningocoque. 17,0 % 0,0 % 47 % Tall F. et coll. Méd. Mal. Infect ; 22 :")
15
Séquelles de la méningite (Etats-Unis)
Séquelles dans 28% des méningites Hib Décès dans 3 à 8 % des cas Séquelles observées : perte auditive dans 20% des cas trouble du langage dans 15 % des cas retard mental dans 11 % des cas retard du développement moteur dans 7% des cas crises d’épilepsie dans 5 % des cas MENINGITIS SEQUELAE In addition to its considerable mortality rate, Hib is a major threat to children who survive. Meningitis can be difficult to recognize at onset. Progression may be so rapid between respiratory infection and signs of meningitis, that it is probable that seizures or serious lethargy have occured by the time diagnostic symptoms have appeared. Long term disability after Hib meningitis is common, even when the mortality is low. Up to 30 % survivors develop sequelae that range from mild hearing loss to severe neurologic damage and mental retardation. Reference: 39 Sell. Haemophilus influenzae type b meningitis: manifestation and long-term sequalae. Pediatr Infect Dis J, 1987; 6: Sell. Ped Infect Dis J, 1987;6:

16
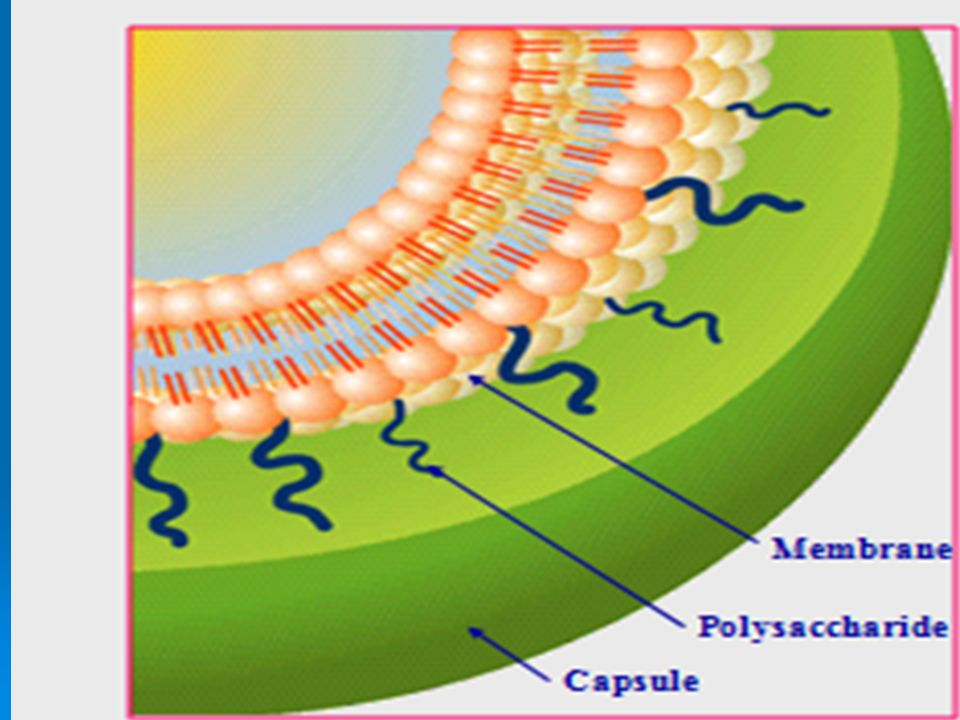
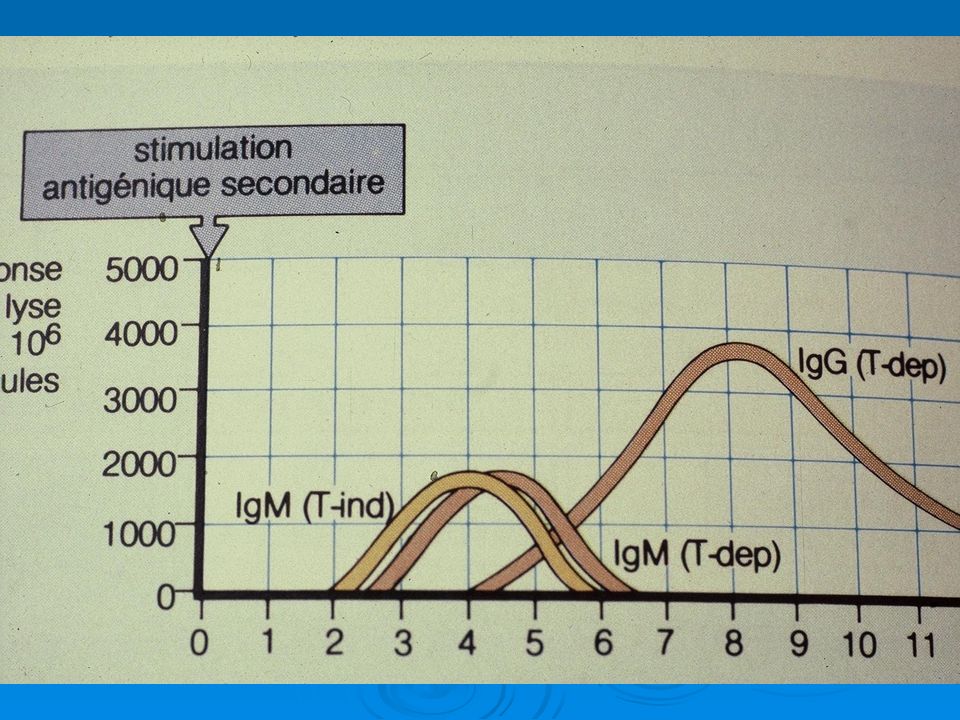
VACCINS Vaccin capsulaire polysaccharidique PRP:histoire d’un échec!!!
Vaccin conjugué à une protéine Tétanique,diphtérique ou du méningocoque LA CONJUGAISON: LA REVOLUTION EN VACCINOLOGIE !!!

21
V. Capsulaires V. Diphtérique V. Tétanique

26
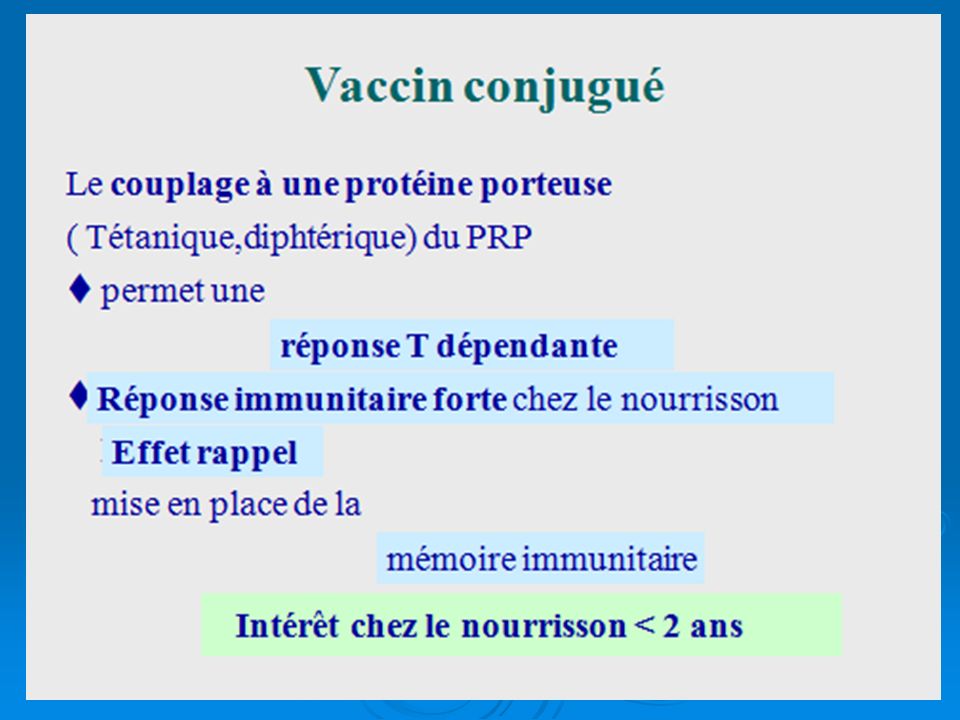
CONJUGAISON EN RESUME Immunogénicité avant 1 an
Réponse anticorps élevée et prolongée Effet Rappel Diminution(ou disparition) du portage pharyngé= effet altruiste
 du portage pharyngé= effet altruiste.")
27
UN VACCIN ALTRUISTE Les enfants vaccinés protègent les enfants non vaccinés Après vaccination, le portage pharyngé d’Hib disparaît: donc plus de contagion

29
ETUDES CLINIQUES Vaccins polysaccharidiques Vaccins conjugués

31
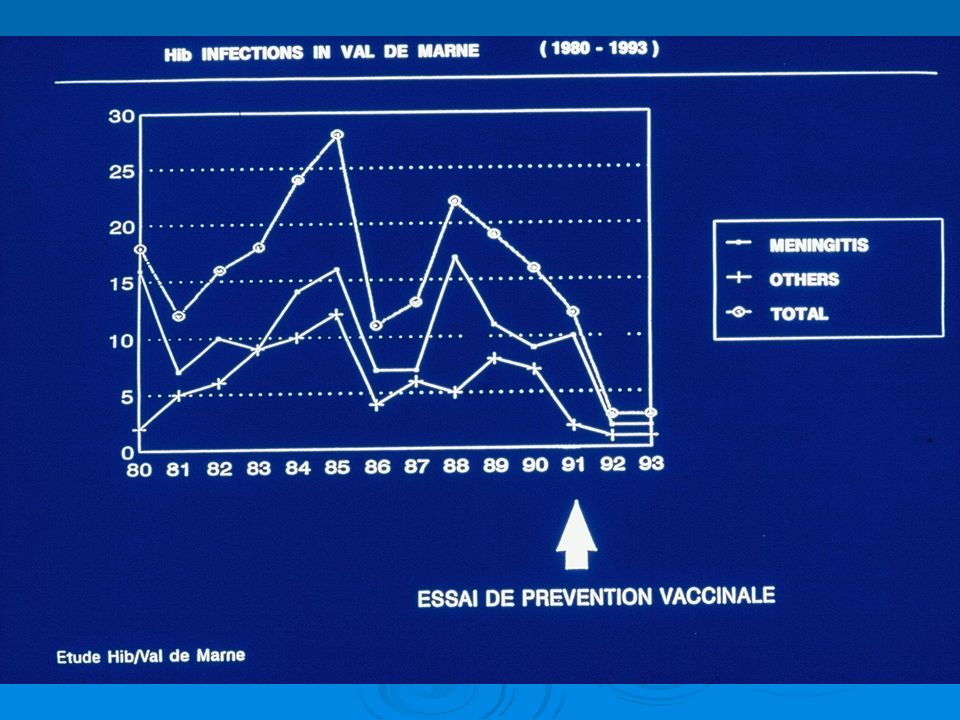
France Etude d’intervention , 1992
enfants vaccinés avec Act-HIBR ou PENTAct-HIB® dans le groupe contrôle Act-HIB EFFICACY IN FRANCE: INTERVENTION STUDY From April 1991 to December 1993, an intervention study was conducted in a district near Paris (Val de Marne). Before 1992, the median yearly incidence was 18 cases in this district. 45,000 children were enrolled, among whom 22,400 received Act-HIB™ or PENTAct-HIB™ and were compared to a non Hib vaccinated control group The results of vaccination with Act-HIB™ or PENTAct-HIB™ are: No case of Hib meningitis in the vaccinated group 3 cases of Hib meningitis in the non-vaccinated group The vaccination with Act-HIB™ or PENTAct-HIB™ had a protective effect on the non-vaccinated population. (This is certainly due to a decrease in the nasopharyngeal carriage of Hib). Act-HIB (even in combination) induces community protection. During years 1996 and 1997, the observation of Hib infections in France has shown a dramatic decrease of type b-meningitis, probably due to the impact of Hib vaccine. References: 13 Boucher et al. Essai De Prévention Des Infections Graves À Haemophilus Influenzae Type B Et Essai De Tolérance, Après Vaccination PRP-T, Dans Le Département Du Val-de-Marne. Arch Pédiatr, 1996; 3: 40 Dabernat et al. Activité du Centre National de Référence des Haemophilus influenzae, années : le déclin du type b. Méd Mal Infect, 1998; 28:940-6. Aucun cas d’infection Hib dans le groupe vacciné 3 cas /an en 1992 et 1993 dans le groupe non-vacciné Boucher, Arch. Pédiatr 1996;3:
. Before 1992, the median yearly incidence was 18 cases in this district. 45,000 children were enrolled, among whom 22,400 received Act-HIB™ or PENTAct-HIB™ and were compared to a non Hib vaccinated control group. The results of vaccination with Act-HIB™ or PENTAct-HIB™ are: No case of Hib meningitis in the vaccinated group. 3 cases of Hib meningitis in the non-vaccinated group. The vaccination with Act-HIB™ or PENTAct-HIB™ had a protective effect on the non-vaccinated population. (This is certainly due to a decrease in the nasopharyngeal carriage of Hib). Act-HIB (even in combination) induces community protection. During years 1996 and 1997, the observation of Hib infections in France has shown a dramatic decrease of type b-meningitis, probably due to the impact of Hib vaccine. References: 13 Boucher et al. Essai De Prévention Des Infections Graves À Haemophilus Influenzae Type B Et Essai De Tolérance, Après Vaccination PRP-T, Dans Le Département Du Val-de-Marne. Arch Pédiatr, 1996; 3: Dabernat et al. Activité du Centre National de Référence des Haemophilus influenzae, années : le déclin du type b. Méd Mal Infect, 1998; 28: Aucun cas d’infection Hib dans le groupe vacciné. 3 cas /an. en 1992 et 1993 dans le groupe non-vacciné. Boucher, Arch. Pédiatr 1996;3:")
33
Royaume-Uni Efficacité d’Act-HIB®
Sur enfants 1200 1000 infections attendues 800 infections observées 600 Nombre de cas 400 99.1 % 97.3 % 94.7 % 200 A follow-up was made during 3 years between Oct and 1995. Immunization schedule was months with PRP-T. Vaccine failures were registered in order to evaluate efficacy of PRP-T. The estimated overall efficacy for 3 doses of PRP-T was 98.1% (95% CI %). A high level of efficacy has been demonstrated with very narrow confidence limits, a degree of precision only possible because of the large size of the population under surveillance. A gradual fall in the efficacy of 3 doses as infants approach the age of 3 years has been shown, with protection remaining reassuringly high at about 95% . The occurrence of herd immunity has resulted in reduced transmission so even the minority of unvaccinated children are protected. This led to the conclusion that a 3 dose schedule may be enough, but only if high vaccination coverage (>90%) is achieved. Reference: 20 Booy et al. Vaccine failures after primary immunization with Haemophilus influenzae type-b conjugate vaccine without booster dose. Lancet, 1997; 349: 5-11 12-23 24-35 âge (mois) Efficacité du Act-HIB® ( mois) = 98.1 % (97.3 % %) Booy, Lancet, 1997; 349:
. A high level of efficacy has been demonstrated with very narrow confidence limits, a degree of precision only possible because of the large size of the population under surveillance. A gradual fall in the efficacy of 3 doses as infants approach the age of 3 years has been shown, with protection remaining reassuringly high at about 95% . The occurrence of herd immunity has resulted in reduced transmission so even the minority of unvaccinated children are protected. This led to the conclusion that a 3 dose schedule may be enough, but only if high vaccination coverage (>90%) is achieved. Reference: 20 Booy et al. Vaccine failures after primary immunization with Haemophilus influenzae type-b conjugate vaccine without booster dose. Lancet, 1997; 349: âge (mois) Efficacité du Act-HIB® ( mois) = 98.1 % (97.3 % %) Booy, Lancet, 1997; 349:")
34
SUEDE Programme National 1992 - 1994
incidence de la méningite ( / 100,000) Act-HIB® 40 30 0-4 ans > 5 ans 20 Tous âges 10 Act-HIB was introduced in June 1992 and has dominated the market with 93 % market share. Schedule of months 2 regions considered : 1st region : before ( ) : incidence of infections 0-4 years = 30.1/ 100,000; after vaccination (1993) incidence was 8.4/100,000 with only 41,900 / 100,000 doses given 2nd region : before incidence = 27.5/ ; after = 7.3/100,000, with 46,600/100,000 doses. In 1993, 48.8% children 0-4 years were vaccinated, more than 95% of them with Act-HIB. In 1994, 63% were vaccinated > 95% with Act-HIB. In 1994 in children 0-4 years a 92% decrease in meningitis was observed and, compared with the pre-vaccination area, the number of bacteraemia cases decreased by 83%. References: 25 Garpenholt et al. Epiglottitis in Sweden before and after introduction of vaccination against Haemophilus influenzae type b. Pediatr Infect Dis J, 1999;18: 26 Garpenholt et al. The impact of Haemophilus influenzae type b vaccination in Sweden. Scand J Infect Dis, 1996; 28: 1987 1988 1989 1990 1991 1992 1993 1994 Diminution de 92 % en 2 ans dans les méningites Hib de 0 à 4 ans Couverture vaccinale de 48.8% en 1993, 63 % en 1994 (0 à 4 ans) O Garpenholt, Scand. J. Infect. Dis., 1996; 28: O Garpenholt, PIDJ, 1999; 18(6): 490-3
 Act-HIB® ans. > 5 ans. 20. Tous âges. 10. Act-HIB was introduced in June 1992 and has dominated the market with 93 % market share. Schedule of months. 2 regions considered : 1st region : before ( ) : incidence of infections 0-4 years = 30.1/ 100,000; after vaccination (1993) incidence was 8.4/100,000 with only 41,900 / 100,000 doses given. 2nd region : before incidence = 27.5/ ; after = 7.3/100,000, with 46,600/100,000 doses. In 1993, 48.8% children 0-4 years were vaccinated, more than 95% of them with Act-HIB. In 1994, 63% were vaccinated > 95% with Act-HIB. In 1994 in children 0-4 years a 92% decrease in meningitis was observed and, compared with the pre-vaccination area, the number of bacteraemia cases decreased by 83%. References: 25 Garpenholt et al. Epiglottitis in Sweden before and after introduction of vaccination against Haemophilus influenzae type b. Pediatr Infect Dis J, 1999;18: Garpenholt et al. The impact of Haemophilus influenzae type b vaccination in Sweden. Scand J Infect Dis, 1996; 28: Diminution de 92 % en 2 ans dans les méningites Hib de 0 à 4 ans. Couverture vaccinale de 48.8% en 1993, 63 % en 1994 (0 à 4 ans) O Garpenholt, Scand. J. Infect. Dis., 1996; 28: O Garpenholt, PIDJ, 1999; 18(6):")
35
GAMBIE Etude d’efficacité, 03/93 - 10/95
Act-HIB® + DTP 2 / 3 / 4 mois d’âge Groupe recevant Act-HIB® 21.490 Contrôles 21.358 0 pneumonie Hib * 1 infection Hib * 10 pneumonies Hib * 19 infections Hib * EFFICACY STUDY IN GAMBIA A double blind randomized trial carried out in children. Children who presented with signs of invasive Hib infection were investigated by lumbar puncture, chest radiograph or percutaneous lung aspirate. Children were followed between 5 and 36 months. Efficacy Act-HIB has an excellent efficacy in a high-risk population. Efficacy of 3 doses for the prevention of all invasive Hib disease was 95%. For the prevention of pneumonia, the efficacy of 2 or more doses was 100 %. Reference: 16 Mulholland et al. Randomised trial of Haemophilus influenzae type-b tetanus protein conjugate for prevention of pneumonia and meningitis in Gambian infants. Lancet, 1997; 349(9060): Après 3 doses Efficacité de 100 % pour les pneumonies Hib confirmées IC [55-100] Efficacité de 95 % pour la maladie Hib IC [67-100] *Hib isolé par culture cellulaire Mulholland K, Lancet, 1997; 349(9060):
: Après 3 doses. Efficacité de 100 % pour les pneumonies Hib confirmées IC [55-100] Efficacité de 95 % pour la maladie Hib IC [67-100] *Hib isolé par culture cellulaire. Mulholland K, Lancet, 1997; 349(9060):")
36
EFFICACITE COMPAREE DES VACCINS
N° of Vaccine Country Schedule ( months) Efficacy subjects US (88) 20 800 2-4-6 14 100 % after 3 doses 84% overall HbOC Finland (88) 50 000 4-6 18 97 % PRP-OMP US Navajo 5 000 2 - 4 95% US * 10 000 2-4-6 14 No case Finland 97 000 4-6 18 100 % CONJUGATE VACCINE EFFICACY TRIALS HbOC 2 prospective studies show that 2 or 3 doses of HbOC provide protection. PRP-OMP PRP-OMP was evaluated in a randomized double blind, placebo controlled trial in a Navajo Indian population. One vaccine failure occurred in a 15 1/2 months old child who received 2 doses, and another in a 7 months old child who received a single dose at 6 months. PRP-T 2 double-blind studies in US : in North Carolina, more than children participated, with no case in vaccinated children and in California no case were reported in more than cihldren. PRP-T was also tested in UK, Finland, Chile and recently in a high risk population : Gambia References: 1 Plotkin. Haemophilus influenzae vaccines. VACCINE, 3rd edition 4. MMWR, 1993;42(RR-13): 1-16. 14 Booy et al . Efficacy of Haemophilus influenzae type b conjugate vaccine PRP-T. Lancet, 1994;344: 15 Lagos et al. Large scale, postlicensure, selective vaccination of Chilean infants with PRP-T conjugate vaccine: practicality and effectiveness in preventing invasive Haemophilus influenzae type b infections. Pediatr Infect Dis J, 1996; 15: UK 27 000 2-3-4 95 % PRP-T Chile 71 000 2-4-6 91,7 % in meningitis 80 % in pneumonia Gambia 42 000 2-3-4 95 % all infections 100% in pneumonia *US study using PRP-T was stopped in because of licensure of HbOC. Results from discontinued study showing PRP-T was effective, it was licensed in 1993 for infant use. Plotkin S, Vacccine, 3rd ed MMWR, 1993;42(RR-13): 1-16.
 Efficacy. subjects. US (88) % after 3 doses. 84% overall. HbOC. Finland (88) % PRP-OMP. US Navajo % US * No case. Finland % CONJUGATE VACCINE EFFICACY TRIALS. HbOC. 2 prospective studies show that 2 or 3 doses of HbOC provide protection. PRP-OMP. PRP-OMP was evaluated in a randomized double blind, placebo controlled trial in a Navajo Indian population. One vaccine failure occurred in a 15 1/2 months old child who received 2 doses, and another in a 7 months old child who received a single dose at 6 months. PRP-T. 2 double-blind studies in US : in North Carolina, more than children participated, with no case in vaccinated children and in California no case were reported in more than cihldren. PRP-T was also tested in UK, Finland, Chile and recently in a high risk population : Gambia. References: 1 Plotkin. Haemophilus influenzae vaccines. VACCINE, 3rd edition. 4. MMWR, 1993;42(RR-13): Booy et al . Efficacy of Haemophilus influenzae type b conjugate vaccine PRP-T. Lancet, 1994;344: Lagos et al. Large scale, postlicensure, selective vaccination of Chilean infants with PRP-T conjugate vaccine: practicality and effectiveness in preventing invasive Haemophilus influenzae type b infections. Pediatr Infect Dis J, 1996; 15: UK % PRP-T. Chile ,7 % in. meningitis. 80 % in. pneumonia. Gambia % all infections. 100% in. pneumonia. *US study using PRP-T was stopped in 1990 because of licensure of HbOC. Results from discontinued study. showing PRP-T was effective, it was licensed in 1993 for infant use. Plotkin S, Vacccine, 3rd ed MMWR, 1993;42(RR-13):")
37
QUESTIONS APRES 25 ANS D’EXISTENCE
Quel est le meilleur schéma vaccinal? Echecs Emergence de nouveaux sérotypes? Devenir des anticorps chez l’adolescent et l’adulte? Interactions antigéniques Schémas simplifiés

38
PROBLEMES EN 2000 (Angleterre)
Recrudescence d’infections invasives,malgrè une CV>85% Adultes++ Enfants EXPLICATIONS: Pas de rappel après un an Taux d’anticorps diminués chez l’adulte Moins bonne immunogénicité si associé au Coq acellulaire

40
REPONSE A CES QUESTIONS
Réintroduction du vaccin à germes entiers:abandon rapide devant la mauvaise tolérance Rappel à 16/18 mois(schéma français) RESULTATS(2003) Amélioration de l’efficacité vaccinalle… Mc Vernon BMJ
 RESULTATS(2003) Amélioration de l’efficacité vaccinalle… Mc Vernon BMJ")
41
INCIDENCE SUR 5 ANS(2009-2012 (U.K)
106 infections invasives 0.06/ contre 0.6/ (1985) Adultes:73% Pneumonie:56% Comorbidité:77% ECHECS VACCINAUX: Vaccination complète:2 !!! Incomplète: 7 Epiglottite: 19 cas ,dont 13 adultes S.Collins CID Sept
 Adultes:73% Pneumonie:56% Comorbidité:77% ECHECS VACCINAUX: Vaccination complète:2 !!! Incomplète: 7 Epiglottite: 19 cas ,dont 13 adultes S.Collins CID Sept")
42
INCIDENCE France 1987-2008 Début vaccination:1993
:0.9/ :0.09/ DIMINUTION:96%!!! <3 mois diminution de 12 à 0.4/ >15 ans diminution de 12 à0.4/ NON VACCINES=EFFET TROUPEAU >64 ans:augmentation de 2 à 2.4/ S.Georges Epidemiol.Infect

43
ECHECS Expérience anglaise
Prématurés Schéma : mois sans rappels majorité des échecs entre 2 et 4 ans( 96 méningites entre 1992 et 1999) Rappel à mois depuis 2003 SA. Silfverdal Lancet 2003 :
 Rappel à mois depuis SA. Silfverdal. Lancet 2003 :")
44
DEVENIR DES ANTICORPS 98% des enfants ont des anticorps protecteurs vers 5 ans: infections inapparente à Hib,immunité croisée? Mais après vaccination( antigène artificiel)? A 5 ans GMT> 1mcgr/ml 100% en UK (Heath JAMA 2000) A 7 ans: de 1,5 à 2,8 microgr/ml (témoins: 1,3)(Claesson) Adolescents,anciens vaccinés taux double(Garner) Mais émergence se méningites à Hib chez l’adulte en 1994(Mac Vernon) Anticorps passés de 1,29 à 0,70 de 1991 à ?
 A 5 ans GMT> 1mcgr/ml 100% en UK (Heath JAMA 2000) A 7 ans: de 1,5 à 2,8 microgr/ml (témoins: 1,3)(Claesson) Adolescents,anciens vaccinés taux double(Garner) Mais émergence se méningites à Hib chez l’adulte en 1994(Mac Vernon) Anticorps passés de 1,29 à 0,70 de 1991 à 1994")
45
VACCINS COMBINES: AVANTAGES ET RISQUES
Amélioration de la couverture vaccinale Simplification Moindre coût Mais risques d’interaction antigénique

46
Impact de l’introduction des combinaisons vaccinales en France
HEXAVAC DTCPHib -HB 2002 DT-Coq TETRACOQ DTC-P 1965 PENTACOQ DTCP -Hib 1992 100000 10000 Nombre de cas 1000 100 10 Ce graphe, utilisant une échelle logarithmique, montre l’impact de l’introduction d’un vaccin sur l’incidence de la maladie. L’introduction d’un vaccin dans une combinaison diminue de façon significative l’incidence de la maladie. 1 1950 1953 1956 1959 1962 1965 1968 1971 1974 1977 1980 1983 1986 1989 1992 1995 1998 2001 Polio (1958) T décès (1936) D (1937) Coq (1948) M. à Hib (1992) HB (1981) (année d’introduction de la vaccination) D’après : BEH 46-47/00 (Polio) ; 28/93,17/01 (T) ;num.spécial Fév.98 (D) ; 19/90, 18/01 (C) ; 47/87, 15/99 (M à Hib) et MASSARI V. et al. European Journal of Epidemiology 1998; 14: PATEY O. et DELLION S. Rev Med interne 1999; 20: Secrétariat d’état à la santé. Dossier de presse 1998
 T décès (1936) D (1937) Coq (1948) M. à Hib (1992) HB (1981) (année d’introduction de la vaccination) D’après : BEH 46-47/00 (Polio) ; 28/93,17/01 (T) ;num.spécial Fév.98 (D) ; 19/90, 18/01 (C) ; 47/87, 15/99 (M à Hib) et MASSARI V. et al. European Journal of Epidemiology 1998; 14: PATEY O. et DELLION S. Rev Med interne 1999; 20: Secrétariat d’état à la santé. Dossier de presse")
47
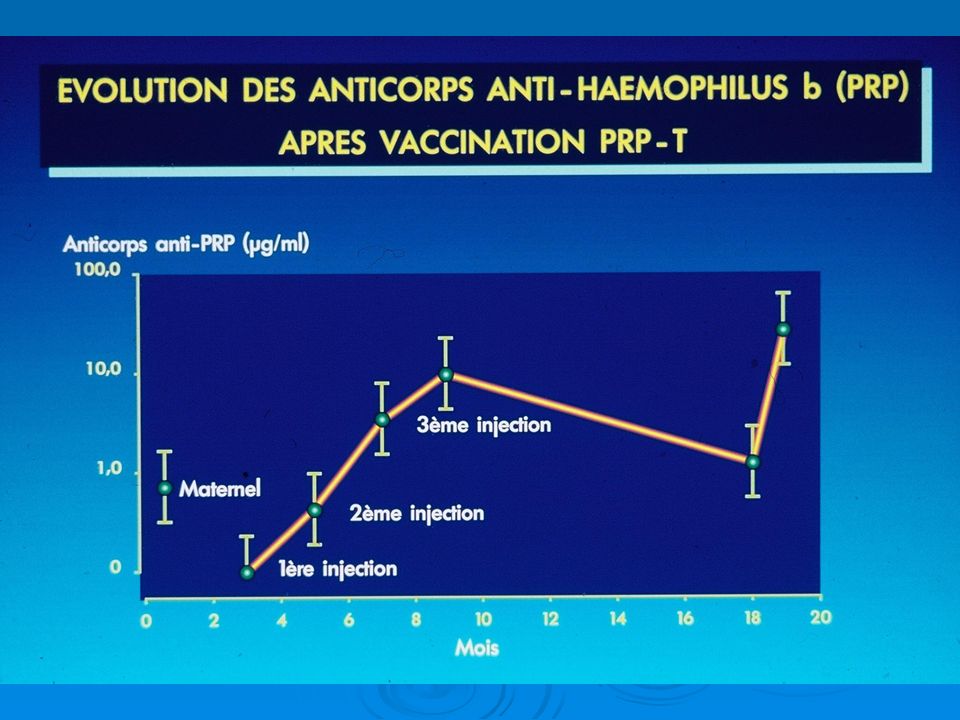
EFFET INHIBITEUR DU VACCIN COQUELUCHEUX ACELLULAIRE
INTERFERENCE IMMUNE Ac anti-PRP après 3 doses (PV) (GMT g/ml) Administration Combinée Simultanée Schmitt DTaP/Hib Schmitt DTaP-HB/Hib Eskola DTaP-IPV/Hib
 (GMT g/ml) Administration Combinée Simultanée. Schmitt DTaP/Hib. Schmitt DTaP-HB/Hib. Eskola DTaP-IPV/Hib.")
48
OU PLUTOT EFFET ADJUVANT DU VACCIN COQUELUCHEUX CLASSIQUE!!!
Etude comparée des taux d’anticorps anti-haemophilus B après vaccination DT polioCoq acellulaire à DTPolio Coq germes entiers: GMT 3 fois plus élevée à 18 mois dans le lot Coq germes entiers A 5 ans GMT identiques > 1 mcgr/ml) Southern J Clin. Vaccine Oct 2007
 Southern J Clin. Vaccine Oct")
49
CONSEQUENCE CLINIQUE? En Allemagne qui n’utilise que les vaccins coquelucheux acellulaires combinés au vaccin haemophilus, il n’y a pas eu de recrudescence d’infections invasives à Haemophilus b Conséquence:tous les pays occidentaux sont passés au vaccin coquelucheux acellulaire( abandon du vaccin germes entiers)
")
50
DERNIERES DONNEES Epidémiologie INDE
nouveaux cas /an pneumonies++ méningites décès Introduction du vaccin pentavalent liquide(certains états) Verma R Hum. Vaccin.Immunother Apr 9;(7)
 Verma R Hum. Vaccin.Immunother Apr 9;(7)")
51
LE POINT EN 2014 OMS:fait partie du PEVD…. Mais
Peu d’enfants reçoivent 3 doses: Efficacité:1 dose 59% 2 doses 92% 3 doses 93% CALENDRIER VACCINAL Français 2013 2,4, 11 mois (efficacité identique au schéma 2,3,4 + rappel à 18 mois) LE POINT EN 2014
 LE POINT EN")
52
POURQUOI LE VACCIN HiB EST UNIQUE !!!!
Disparition totale de l’Haemophilus b du pharynx chez le vacciné Pas d’émergence de nouvelles souches capsulées, virulentes dans le pharynx Emergence de souches non typables(hémocultures) surtout chez l’immunodéprimé ? Persistance de l’immunité chez l’adulte (alors qu’ Hib ne circule plus)Immunité croisée avec des entérobactéries intestinales
 surtout chez l’immunodéprimé Persistance de l’immunité chez l’adulte (alors qu’ Hib ne circule plus)Immunité croisée avec des entérobactéries intestinales.")
53
Merci de votre attention !
Documents Pr E. Caumes, photos G. Lecso, D. Richard-Lenoble, M. Danis,…

Présentations similaires












 Biomarqueurs IHC (n = 412) Séquençage (n = 418) 200 patients évaluables pour les facteurs pronostiques cliniques et biologiques Comparaison.>")









