Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Nouveaux Antiplaquettaires, Nouveaux Risques?
Template _1 4/17/ :28 AM Nouveaux Antiplaquettaires, Nouveaux Risques? Poitiers le 19 septembre 2009 Institut de Cardiologie – Inserm 937 Pitié-Salpêtrière University Hospital 75013 Paris

2
Traitements antiagrégants en France
Traitement-années (millions) traitements-années Aspirine à faible dose Clopidogrel traitements-années Rapport AFSSAPS juillet 2005, Données GERS 2
 traitements-années. Aspirine à faible dose. Clopidogrel traitements-années. Rapport AFSSAPS juillet 2005, Données GERS. 2.")
3
Platelet Activation Mechanisms
ASPIRIN C18886 x 5HT 5HT Thromboxane TICLOPIDINE CLOPIDOGREL PRASUGREL Coagulation Collagen ADP ADP ADP A 2 x ATP ATP SCH530348 Thrombin GPVI 5HT 2A P2Y TP a 1 P2X ACTIVE METABOLITE PAR4 1 PAR1 x Dense granule AZD6140 CANGRELOR PLATELET P2Y 12 Thrombin generation ACTIVATION Amplification Shape change Alpha granule x x Aggregation a IIb b 3 a b a b IIb 3 Fibrinogen IIb 3 Coagulation factors Inflammatory mediators GP IIb/IIIa ANTAGONISTS Storey RF. Curr Pharm Des. 2006;12:

4
Une success Story 4

5
Clopidogrel vs Ticlopidine on 30-day MACE
Trial n Odds ratios & 95% CI Clop. Ticl. CLASSICS 1,020 1.3% 0.9% TOPPS 941 2.6% 3.5% Müller 700 3.1% 2.0% CCF 2,369 5.7% 8.9% Lenox Hill 2,565 2.4% 3.8% Mayo 2,827 0.6% 1.6% N. Memorial 1,378 0.8% 2.2% S. Illinois 875 2.1% 1.4% Wash. Hosp. 844 2.0% 0.5% Wessex 361 2.3% 5.3% 0.50 (0.40, 0.61) p = 0.001 Overall 13,880 2.0% 4.0% 10 0.1 1 Clopidogrel better Ticlopidine better Bhatt DL et al. J Am Coll Cardiol 2002;39:9–14
 p = Overall. 13, % 4.0% Clopidogrel better. Ticlopidine better. Bhatt DL et al. J Am Coll Cardiol 2002;39:9–14.")
6
Plavix Robust Clinical Research Program More than 100,000 patients in the clinical program… .... and more than 70 million of patients treated to date Ongoing Trials Indication in STEMI patients CURRENT Published Trials ACTIVE ACTIVE CASPAR CASPAR CASPAR CHARISMA CHARISMA CHARISMA CHARISMA Indication in UA/NSTEMI patients COMMIT CCS2 COMMIT CCS2 COMMIT CCS2 COMMIT CCS2 COMMIT CCS2 Indication in patients after MI, IS, or with established PAD CLARITY CLARITY CLARITY CLARITY CLARITY CLARITY CARESS CARESS CARESS CARESS CARESS CARESS CARESS MATCH MATCH MATCH MATCH MATCH MATCH MATCH MATCH CREDO CREDO CREDO CREDO CREDO CREDO CREDO CREDO CREDO CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE 1996 2000 2001 2002 2004 2004 2005 2005 2006 2007 2009 2009 Publication Date Expected Date of Results
 CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CURE (PCI-CURE) CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CLASSICS. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE. CAPRIE Publication Date. Expected Date of Results.")
7
Primary Outcome (Stroke, MI, non-CNS Systemic Embolism, Vascular Death)
1000 patients treated for 3 years: Prevent 28 strokes (17 fatal or disabling) and 6 myocardial infarctions Cost 20 (non-stroke) major bleeds (3 fatal)
 and 6 myocardial infarctions. Cost 20 (non-stroke) major bleeds (3 fatal)")
8
Indications 8

9
Maladie Coronaire Stable
Poursuivre l’aspirine à faibles doses (75 à 162 mg/j)(Grade 1A). Il est suggéré de le poursuivre indéfiniment (Grade 2C) Si maladie coronaire symptomatique= associer aspirine (75–100mg/j) et clopidogrel (75 mg/j) [Grade 2B] Si DES, apirine (75–100mg/j) plus clopidogrel (75 mg/j pour au moins 12 mois) [Grade 1A pour 3 à 4 mois; Grade 1B pour 4 à 12 mois]. Après 1 an, poursuivre l’association indéfiniment en l’absence de saignement et si bonne tolérance (Grade 2C) (CHEST 2008; 133:71S–105S) *risque annuel de décès/AVC/IDM >10%, c'est-à-dire ceux ayant une maladie coronaire tritronculaire avec de multiples stents, les diabétiques avec petits vaisseaux, ceux ayant récidivé sous monothérapie antiagrégante, ceux ayant une localisation extracoronaire symptomatique
(Grade 1A). Il est suggéré de le poursuivre indéfiniment (Grade 2C) Si maladie coronaire symptomatique= associer aspirine (75–100mg/j) et clopidogrel (75 mg/j) [Grade 2B] Si DES, apirine (75–100mg/j) plus clopidogrel (75 mg/j pour au moins 12 mois) [Grade 1A pour 3 à 4 mois; Grade 1B pour 4 à 12 mois]. Après 1 an, poursuivre l’association indéfiniment en l’absence de saignement et si bonne tolérance (Grade 2C) (CHEST 2008; 133:71S–105S) *risque annuel de décès/AVC/IDM >10%, c est-à-dire ceux ayant une maladie coronaire tritronculaire avec de multiples stents, les diabétiques avec petits vaisseaux, ceux ayant récidivé sous monothérapie antiagrégante, ceux ayant une localisation extracoronaire symptomatique.")
10
Bénéfice Clinique Net après 1 an de bithérapie
Aspirine seul TS: 0.5% Décès, IDM, AVC (TS exclus): 4% Saignement majeur: 0.5% Dual OAT (aspirin and clopidogrel) TS: 0.35% Décès, IDM, AVC (TS exclus): 3% Saignement majeurr: 0.6% 5% 4%
: 4% Saignement majeur: 0.5% Dual OAT (aspirin and clopidogrel) TS: 0.35% Décès, IDM, AVC (TS exclus): 3% Saignement majeurr: 0.6% 5% 4%")
11
Les Enjeux Pratiques non Résolus
La résistance aux AAP La place des nouveaux Interruption de la bithérapie

12
Interruption prématurée
12

13
But : éliminer l’interruption prématurée des AAP
Chez les patients chez qui on suspecte une mauvaise compliance au plavix la première année, éviter le stent actif En cas de chirurgie programmée la première année, éviter le stent actif L’éducation sur la compliance et le risque d’interruption prématurée est une priorité Les tutelles doivent être mises en garde sur le risque d’interruption prématuré, en particulier le coût ne doit pas être une cause d’arrêt prématuré Différer toute intervention jusqu’à au moins 1 an après le mise en place d’un stent actif et 1 mois en cas de stent nu En cas de stent actif, poursuivre aspirine et reprende clopidogrel le plus rapidement Circulation 2007; 115

14
Discontinuation of Single/Dual OAT
Background—Antiplatelet therapy is often discontinued in patients with drug-eluting stents who are undergoing surgical procedures. However, discontinuation of antiplatelet therapy is an important risk factor for late stent thrombosis. Our objective was to examine the safety of short-term discontinuation of antiplatelet therapy. Methods and Results—We systematically searched Medline for reported cases of late stent thrombosis and very late stent thrombosis published between January 2001 and July We restricted our search to Academic Research Consortium– defined definite cases. We identified 161 cases of late stent thrombosis or very late stent thrombosis from 84 articles (79 from case reports, 61 from registries, and 21 from randomized clinical trials). Patients had a mean age of years, and 88% were male. A total of 19 cases occurred in patients who were receiving dual antiplatelet therapy at the time of the event. If patients stopped both antiplatelet agents simultaneously, the median time to event was 7 days. If patients had previously stopped a thienopyridine with no ill effect and subsequently stopped acetylsalicylic acid, the median time to event was also 7 days from the time of acetylsalicylic acid cessation. If the thienopyridine was stopped but acetylsalicylic acid was maintained, the median time to event was 122 days. Among the 48 patients who stopped both agents, 36 cases (75%) occurred within 10 days. Among the 94 patients who discontinued a thienopyridine but continued acetylsalicylic acid, only 6 cases (6%) occurred within 10 days. Conclusion—If acetylsalicylic acid therapy is maintained, short-term discontinuation of a thienopyridine may be relatively safe in patients with drug-eluting stents. (Circulation. 2009;119: ) 161 cases of late or very late stent thrombosis (84 articles) Eisenberg et al. Circulation In press
. Patients had a mean age. of years, and 88% were male. A total of 19 cases occurred in patients who were receiving dual antiplatelet therapy at the time of the event. If patients stopped both antiplatelet agents simultaneously, the median time to event was 7 days. If patients had previously stopped a thienopyridine with no ill effect and subsequently stopped acetylsalicylic acid, the median time to event was also 7 days from the time of acetylsalicylic acid cessation. If the thienopyridine was stopped but acetylsalicylic acid was maintained, the median time to event was 122 days. Among the 48 patients who stopped both agents, 36 cases (75%) occurred within 10 days. Among the 94 patients who discontinued a thienopyridine but continued acetylsalicylic acid, only 6 cases (6%) occurred within 10 days. Conclusion—If acetylsalicylic acid therapy is maintained, short-term discontinuation of a thienopyridine may be relatively. safe in patients with drug-eluting stents. (Circulation. 2009;119: ) 161 cases of late or very late stent thrombosis (84 articles) Eisenberg et al. Circulation In press.")
15
Discontinuation of Single/Dual OAT
Background—Antiplatelet therapy is often discontinued in patients with drug-eluting stents who are undergoing surgical procedures. However, discontinuation of antiplatelet therapy is an important risk factor for late stent thrombosis. Our objective was to examine the safety of short-term discontinuation of antiplatelet therapy. Methods and Results—We systematically searched Medline for reported cases of late stent thrombosis and very late stent thrombosis published between January 2001 and July We restricted our search to Academic Research Consortium– defined definite cases. We identified 161 cases of late stent thrombosis or very late stent thrombosis from 84 articles (79 from case reports, 61 from registries, and 21 from randomized clinical trials). Patients had a mean age of years, and 88% were male. A total of 19 cases occurred in patients who were receiving dual antiplatelet therapy at the time of the event. If patients stopped both antiplatelet agents simultaneously, the median time to event was 7 days. If patients had previously stopped a thienopyridine with no ill effect and subsequently stopped acetylsalicylic acid, the median time to event was also 7 days from the time of acetylsalicylic acid cessation. If the thienopyridine was stopped but acetylsalicylic acid was maintained, the median time to event was 122 days. Among the 48 patients who stopped both agents, 36 cases (75%) occurred within 10 days. Among the 94 patients who discontinued a thienopyridine but continued acetylsalicylic acid, only 6 cases (6%) occurred within 10 days. Conclusion—If acetylsalicylic acid therapy is maintained, short-term discontinuation of a thienopyridine may be relatively safe in patients with drug-eluting stents. (Circulation. 2009;119: ) Eisenberg et al. Circulation In press
. Patients had a mean age of years, and 88% were male. A total of 19 cases occurred in patients who were receiving dual antiplatelet therapy at the time of the event. If patients stopped both antiplatelet agents simultaneously, the median time to event was 7 days. If patients had previously stopped a thienopyridine with no ill effect and subsequently stopped acetylsalicylic acid, the median time to event was also 7 days from the time of acetylsalicylic acid cessation. If the thienopyridine was stopped but acetylsalicylic acid was maintained, the median time to event was 122 days. Among the. 48 patients who stopped both agents, 36 cases (75%) occurred within 10 days. Among the 94 patients who discontinued a thienopyridine but continued acetylsalicylic acid, only 6 cases (6%) occurred within 10 days. Conclusion—If acetylsalicylic acid therapy is maintained, short-term discontinuation of a thienopyridine may be relatively. safe in patients with drug-eluting stents. (Circulation. 2009;119: ) Eisenberg et al. Circulation In press.")
16
Aspirin Compliance Cuisset el al. Am H Journal In Press
noncompliance was investigated. One hundred ninety patients with a history of myocardial infarction were evaluated using arachidonic acid–stimulated light aggregometry at 3 different time points: while receiving their usual daily aspirin, after not receiving aspirin for 7 days, and 2 hours after the observed ingestion of aspirin 325 mg. At the first time point, 17 patients (9%) failed to show aspirin inhibition of platelet aggregation, but 2 hours after observed aspirin ingestion, aspirin inhibition was observed in all but 1 patient. Cuisset el al. Am H Journal In Press
 failed to show aspirin inhibition of platelet aggregation, but 2 hours after observed aspirin ingestion, aspirin. inhibition was observed in all but 1 patient. Cuisset el al. Am H Journal In Press.")
17
Interruption après 1 an 17

18
Primary Endpoint (MI/Stroke/CV Death) in Patients with Previous MI, IS, or PAD “CAPRIE-like Cohort”
RRR: 17.1 % [95% CI: 4.4%, 28.1%] p=0.01 Primary outcome event rate (%) 2 4 6 8 10 Months since randomization 12 18 24 30 Clopidogrel + ASA 7.3 % Placebo + ASA 8.8 % N=9,478 A post-hoc analysis of patients (n=9478) with a previous MI, stroke, or PAD (similar to the entry criteria for the CAPRIE trial) showed a significant 17.1% RRR in favor of clopidogrel plus ASA over ASA alone Bhatt DL et Al., JACC 2007 .
 Months since randomization Clopidogrel + ASA. 7.3 % Placebo + ASA. 8.8 % N=9,478. A post-hoc analysis of patients (n=9478) with a previous MI, stroke, or PAD (similar to the entry criteria for the CAPRIE trial) showed a significant 17.1% RRR in favor of clopidogrel plus ASA over ASA alone. Bhatt DL et Al., JACC")
19
Long-term Bleeding Risk?
Placebo + ASA Clopidogrel + ASA Hazard function per day 15 60 135 270 450 630 810 Days since randomization Bhatt DL et al. J Am Coll Cardiol 2007;49:1982–1988. 19

20
KM from Time of Discontinuation to first Event* Placebo vs Clopidogrel
*Primary Efficacy Endpoint (death/MI/Stroke) Average time from drug discontinuation to primary endpoint was 228 days (95% CI ) 100 90 80 70 60 ----Clopidogrel Placebo (9) First event could be prior to discontinuation though. From my calculation, 153 (70 out of 194 for clopidogrel and 83 out of 211 for placebo) of the 405 events in the withdrawers group occurred on or before permanent discontinuation. These are subgroups defined based on a post-randomization (study drug treatment) event. It is a non-randomized comparison that could certainly be biased by treatment effect. TingFei: do you confirm these numbers? Where do they come from? When I see the diverging curves all the way to end of FU , I think it reflects what we say : a high risk profile of this population. We would need KM curves starting at study drug cessation to answer your question precisely. log-rank test, p=0.029 clopidogrel was an independent correlate for survival (HR 0.75; 95% CI , p=0.016) Arch Cardiovasc Dis Jun-Jul;102(6-7):485-96
 Average time from drug discontinuation to primary endpoint was 228 days (95% CI ) Clopidogrel. Placebo. (9) First event could be prior to discontinuation though. From my calculation, 153 (70 out of 194 for clopidogrel and 83 out of 211 for placebo) of the 405 events in the withdrawers group occurred on or before permanent discontinuation. These are subgroups defined based on a post-randomization (study drug treatment) event. It is a non-randomized comparison that could certainly be biased by treatment effect. TingFei: do you confirm these numbers Where do they come from When I see the diverging curves all the way to end of FU , I think it reflects what we say : a high risk profile of this population. We would need KM curves starting at study drug cessation to answer your question precisely. log-rank test, p= clopidogrel was an independent correlate for survival (HR 0.75; 95% CI , p=0.016) Arch Cardiovasc Dis Jun-Jul;102(6-7):")
21
Conlcusions Bithérapie indéfiniment chez tous (principe de précaution)
Monothérapie après 1an chez la majorité Arrêt clopidogrel ? (principe économique) Arrêt aspirine ? (principe de réalisme) « A la carte » (principe de bon sens) Multitronculaires Multistentés Petites artères Post infarctus Diabètiques SAT ou nouvel évènement ischémique Polyvasculaires … Aide à la décision ARCTIC; ISAR-SAFE 21
 Arrêt aspirine (principe de réalisme) « A la carte » (principe de bon sens) Multitronculaires. Multistentés. Petites artères. Post infarctus. Diabètiques. SAT ou nouvel évènement ischémique. Polyvasculaires. … Aide à la décision ARCTIC; ISAR-SAFE. 21.")
22
La résistance: un enjeu
22

23
Effect of 900mg of Clopidogrel LD
The ALBION trial (Assessment of the Best Loading Dose of Clopidogrel to Blunt Platelet Activation, Inflammation and Ongoing Necrosis) RELOAD Study (“REload with cLOpidogrel before coronary Angioplasty in subjects treated long term with Dual antiplatelet therapy”)” Inhibition of RPA 4 hours after the first reloading dose Maximum Inhibition of Platelet Aggregation (ADP 20 µmol/L) Circulation ;118(12):
 RELOAD Study. ( REload with cLOpidogrel before coronary Angioplasty in subjects. treated long term with Dual antiplatelet therapy ) Inhibition of RPA 4 hours after the. first reloading dose. Maximum Inhibition of Platelet Aggregation. (ADP 20 µmol/L) Circulation ;118(12):")
24
Buonamici, J Am Coll Cardiol 2007;49:2312-7
The RECLOSE Study: 6 Month Outcomes After DES Implantation Stratified By Post-Plavix ADP-mediated Platelet Reactivity p<0.001 p<0.001 p<0.001 Non-responders defined as >70% aggregation by LTA 12 hours after 600-mg plavix load Buonamici, J Am Coll Cardiol 2007;49:2312-7 24

25
« VASP-Guided » PCI after a first 600mg LD of clopidogrel
Each LD by 35 to 49% suboptimal response 14% patients remained suboptimal responders Average LD 1600 mg J Am Coll Cardiol 2008;51:1404–11

26
Benefit of High Loading Dose vs Standard Loading Dose
Death and MI within the first month of PCI Study or subcategory High loading Standard loading Peto OR n/N 95% CI Year 01 Randomized trials ALBION 2/ /35 1.03 [0.09, 11.50] 2006 ARMYDA-2 5/ /129 0.35 [0.14, 0.87] 2005 CLEAR PLATELETS 1/ /60 0.36 [0.05, 2.61] Cuisset et al 7/ /146 0.46 [0.19, 1.09] Gurbel et al 0/ /138 ISAR-CHOICE 0/ /20 Muller et al 0/ /10 2001 Subtotal (95% CI) 0.42 [0.23, 0.75] Total events: 15 (High loading), 34 (Standard loading) Test for heterogeneity: Chi² = 0.75, df = 3 (P = 0.86), I² = 0% Test for overall effect: Z = 2.93 (P = 0.003) 02 Non-randomized studies Angiolillo et al 0/ /27 2004 Seyfarth et al 0/ /21 2003 Wolfram et al 13/ /126 1.28 [0.44, 3.74] Total events: 13 (High loading), 4 (Standard loading) Test for heterogeneity: not applicable Test for overall effect: Z = 0.45 (P = 0.66) Total (95% CI) 0.54 [0.32, 0.90] Total events: 28 (High loading), 38 (Standard loading) Test for heterogeneity: Chi² = 3.94, df = 4 (P = 0.41), I² = 0% Test for overall effect: Z = 2.36 (P = 0.02) 0.1 0.2 0.5 1 2 5 10 Favours high loading Favours low loading Aucune augmentation du risque d’hémorragie majeure ou mineure (p=0.55 et p=0.98). Interaction significative entre le taux d’événement ischémique et le bénéfice clinique des fortes doses de charge (p=0.005), suggérant que plus le risque est élevé et plus l’intérêt de forte de charge est important
 [0.23, 0.75] Total events: 15 (High loading), 34 (Standard loading) Test for heterogeneity: Chi² = 0.75, df = 3 (P = 0.86), I² = 0% Test for overall effect: Z = 2.93 (P = 0.003) 02 Non-randomized studies. Angiolillo et al. 0/23 0/ Seyfarth et al. 0/11 0/ Wolfram et al. 13/319 4/ [0.44, 3.74] Total events: 13 (High loading), 4 (Standard loading) Test for heterogeneity: not applicable. Test for overall effect: Z = 0.45 (P = 0.66) Total (95% CI) [0.32, 0.90] Total events: 28 (High loading), 38 (Standard loading) Test for heterogeneity: Chi² = 3.94, df = 4 (P = 0.41), I² = 0% Test for overall effect: Z = 2.36 (P = 0.02) Favours high loading. Favours low loading. Aucune augmentation du risque d’hémorragie majeure ou mineure (p=0.55 et p=0.98). Interaction significative entre le taux d’événement ischémique et le bénéfice clinique des fortes doses de charge (p=0.005), suggérant que plus le risque est élevé et plus l’intérêt de forte de charge est important.")
27
La thrombose de stent : situation complexe
Facteurs multiples Risque de récidive Prévalence de la résistance élevée Thombose de stent sous clopidogrel Efficacité du Prasugrel Circulation Jun 2;119(21):2854-7
:")
28
La résistance: les causes
28

29
Sources de Variabilité de la Réponse aux Médicaments
Dose Prescrite Non-observance Erreur d’administration Dose administrée Absorption Distribution Elimination Facteurs pathologiques et physiologiques Facteurs environnementaux Facteurs génétiques Pharmacocinétique Concentration au site d’action Récepteur Effecteur Pharmacodynamique Effet Déterminisme génétique du métabolisme des médicaments

30
Clopidogrel metabolism
N Cl O OCH3 Esterases ~85% Inactive Metabolites CYP2C19 CYP1A2 CYP2B6 S N Cl O OCH3 Figure 1. Roles in Clopidogrel Activity of Proteins with Known Genetic Polymorphisms. Intestinal absorption of the prodrug clopidogrel is limited by an intestinal efflux pump P-glycoprotein coded by the ABCB1 gene. The majority of the prodrug is metabolized into inactive metabolites by ubiquitous esterases. The minority is bioactivated by various cytochrome P450 (CYP) isoforms into active metabolites. These metabolites irreversibly antagonize the adenosine diphosphate (ADP) receptor (coded by the P2RY12 gene), which in turn inactivates the fibrinogen receptor (the glycoprotein [GP] IIb/IIIa receptor coded by the ITGB3 gene) involved in platelet aggregation. CYP3A4 CYP2C19 CYP2C9 CYP2B6 O OCH3 N HOOC HS Cl N Engl J Med 2008
 isoforms into active metabolites. These metabolites irreversibly antagonize the adenosine diphosphate (ADP) receptor (coded by the P2RY12 gene), which in turn inactivates the fibrinogen receptor (the glycoprotein [GP] IIb/IIIa receptor coded by the ITGB3 gene) involved in platelet aggregation. CYP3A4. CYP2C19. CYP2C9. CYP2B6. O. OCH3. N. HOOC. HS. Cl. N Engl J Med")
31
CYP2C19*2 681 G A *1 (sauvage) *2 (muté) Exon 4 Intron 4 Exon 5
Épissage aberrant Perte de 40bp dans l’exon 5 Décalage du cadre de lecture Codon stop prématuré Exon 4 Exon 5 Exon 4 Exon 5 Protéine complète et fonctionnelle Protéine tronquée et non-fonctionnelle

32
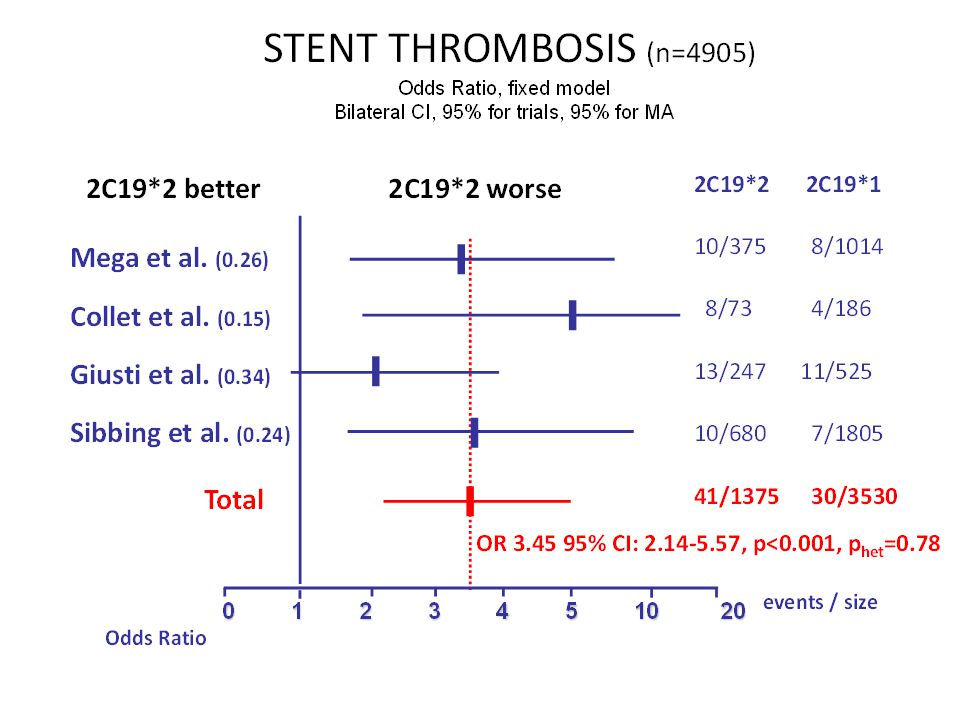
Stent thrombosis3.31 [1.05-10.47]; p=0.04
AFIJI Registry (STEMI<45yrs, n=259) death/non fatal MI /urgent revascularization 1.0 0.0 0.8 0.7 0.6 0.5 CYP 2C19 *1/*1 *1/*2 or *2/*2 HR=3.66; 95%CI ( ) p=0.0005 Stent thrombosis3.31 [ ]; p=0.04 years *1/*1 *1/*2 *2/*2 11/186 (5.9%) 13/64 (20.3%) 2/9 (22.2%)
![Stent thrombosis3.31 [ ]; p=0.04](http://slideplayer.fr/slide/5043479/16/images/32/Stent+thrombosis%EF%83%A03.31+%5B+%5D%3B+p%3D0.04.jpg "AFIJI Registry (STEMI<45yrs, n=259) death/non fatal MI /urgent revascularization CYP 2C19. *1/*1. *1/*2 or *2/*2. HR=3.66; 95%CI ( ) p= Stent thrombosis3.31 [ ]; p= years. *1/*1. *1/*2. *2/*2. 11/186 (5.9%) 13/64 (20.3%) 2/9 (22.2%)")
34
Risk of Adverse Outcomes Associated With Concomitant Use of Clopidogrel and Proton Pump Inhibitors Following Acute Coronary Syndrome 0.7 0.6 0.5 0.4 0.3 0.1 Neither clopi nor PPI PPI without clopi Clopi+PPI Clopi without PPI Death or Rehosp for ACS % Context Prior mechanistic studies reported that omeprazole decreases the platelet inhibitory effects of clopidogrel, yet the clinical significance of these findings is not clear. Objective To assess outcomes of patients taking clopidogrel with or without a proton pump inhibitor (PPI) after hospitalization for acute coronary syndrome (ACS). Design, Setting, and Patients Retrospective cohort study of 8205 patients with ACS taking clopidogrel after discharge from 127 Veterans Affairs hospitals between October 1, 2003, and January 31, Vital status information was available for all patients through September 30, 2006. Main Outcome Measures All-cause mortality or rehospitalization for ACS. Results Of 8205 patients taking clopidogrel after discharge, 63.9% (n=5244) were prescribed PPI at discharge, during follow-up, or both and 36.1% (n=2961) were not prescribed PPI. Death or rehospitalization for ACS occurred in 20.8% (n=615) of patients taking clopidogrel without PPI and 29.8% (n=1561) of patients taking clopidogrel plus PPI. In multivariable analyses, use of clopidogrel plus PPI was associated with an increased risk of death or rehospitalization for ACS compared with use of clopidogrel without PPI (adjusted odds ratio [AOR], 1.25; 95% confidence interval [CI], ). Among patients taking clopidogrel after hospital discharge and prescribed PPI at any point during follow-up (n=5244), periods of use of clopidogrel plus PPI (compared with periods of use of clopidogrel without PPI) were associated with a higher risk of death or rehospitalization for ACS (adjusted hazard ratio, 1.27; 95% CI, ). In analyses of secondary outcomes, patients taking clopidogrel plus PPI had a higher risk of hospitalizations for recurrent ACS compared with patients taking clopidogrel without PPI (14.6% vs 6.9%; AOR, 1.86 [95% CI, ]) and revascularization procedures (15.5% vs 11.9%; AOR, 1.49 [95% CI, ]), but not for all-cause mortality (19. % vs 16.6%; AOR, 0.91 [95% CI, ]). The association between use of clopidogrel plus PPI and increased risk of adverse outcomes also was consistent using a nested case-control study design (AOR, 1.32; 95% CI, ). In addition, use of PPI without clopidogrel was not associated with death or rehospitalization for ACS among patients not taking clopidogrel after hospital discharge (n=6450) (AOR, 0.98; 95% CI, ). Conclusion Concomitant use of clopidogrel and PPI after hospital discharge for ACS was associated with an increased risk of adverse outcomes than use of clopidogrel without PPI, suggesting that use of PPI may be associated with attenuation of benefits of clopidogrel after ACS. AOR=1.25; 95% CI ( ) Period since discharge in days JAMA. 2009;301(9):
 after hospitalization for acute coronary syndrome (ACS). Design, Setting, and Patients Retrospective cohort study of 8205 patients with ACS taking clopidogrel after discharge from 127 Veterans Affairs hospitals between October 1, 2003, and January 31, Vital status information was available for all patients through September 30, Main Outcome Measures All-cause mortality or rehospitalization for ACS. Results Of 8205 patients taking clopidogrel after discharge, 63.9% (n=5244) were prescribed PPI at discharge, during follow-up, or both and 36.1% (n=2961) were not prescribed PPI. Death or rehospitalization for ACS occurred in 20.8% (n=615) of patients taking clopidogrel without PPI and 29.8% (n=1561) of patients taking clopidogrel plus PPI. In multivariable analyses, use of clopidogrel plus PPI was associated with an increased risk of death or rehospitalization for ACS compared with use of clopidogrel without PPI (adjusted odds ratio [AOR], 1.25; 95% confidence interval [CI], ). Among patients taking clopidogrel after hospital discharge and prescribed PPI at any point during follow-up (n=5244), periods of use of clopidogrel plus PPI (compared with periods of use of clopidogrel without PPI) were associated with a higher risk of death or rehospitalization for ACS (adjusted hazard ratio, 1.27; 95% CI, ). In analyses of secondary outcomes, patients taking clopidogrel plus PPI had a higher risk of hospitalizations for recurrent ACS compared with patients taking clopidogrel without PPI (14.6% vs 6.9%; AOR, 1.86 [95% CI, ]) and revascularization procedures (15.5% vs 11.9%; AOR, 1.49 [95% CI, ]), but not for all-cause mortality (19. % vs 16.6%; AOR, 0.91 [95% CI, ]). The association between use of clopidogrel plus PPI and increased risk of adverse outcomes also was consistent using a nested case-control study design (AOR, 1.32; 95% CI, ). In addition, use of PPI without clopidogrel was not associated with death or rehospitalization for ACS among patients not taking clopidogrel after hospital discharge (n=6450) (AOR, 0.98; 95% CI, ). Conclusion Concomitant use of clopidogrel and PPI after hospital discharge for ACS. was associated with an increased risk of adverse outcomes than use of clopidogrel without PPI, suggesting that use of PPI may be associated with attenuation of benefits of. clopidogrel after ACS. AOR=1.25; 95% CI ( ) Period since discharge in days. JAMA. 2009;301(9):")
35
What We Do Not Know, Precisely
Platelet resistance (low response on a functional test) Genetic resistance (2C19*2) Clinical Resistance (thrombotic event)
 Genetic resistance. (2C19*2) Clinical Resistance. (thrombotic event)")
36
PHAO 2008 ARCTIC (Essai n° P080403)- Promoteur AP-HP
Assessment with a double Randomization of 1) a monitoring-adjusted antiplatelet treatment vs. a Common antiplatelet Treatment for DES implantation, and 2) Interruption vs. Continuation of double antiplatelet therapy one year after stenting Randomisation avant implantation d’un stent actif Groupe 1 : Bras Monitoré -Evaluation systématique de la réponse biologique à l’aspirine et au clopidogrel avant la mise en place de l’endoprothèse active. 2-Adaptation du traitement antiplaquettaire chez les hypo-répondeurs au moment de l’angioplastie 3-Réévaluation chez tous les patients à J30±3 de la réponse au traitement antiplaquettaire oral et ajustement du de la dose d’entretien Groupe 2 : Bras Conventionnel - Pas d’évaluation de la réponse biologique au traitement antiplaquettaire - La stratégie antiplaquettaire orale est laissée à la discrétion de l’investigateur en fonction des pratiques habituelles Evaluation du critère primaire de jugement tous les 6 mois (6 jusqu’à 18 mois) Toute cause de mortalité Infarctus du myocard Toute revascularisation urgente Thrombose de stent nécessitant une revascularisation ou non AVC ischémique nécessitant une nouvelle hospilisation PHAO 2008 ARCTIC (Essai n° P080403)- Promoteur AP-HP
 a monitoring-adjusted antiplatelet treatment vs. a Common antiplatelet Treatment for DES implantation, and 2) Interruption vs. Continuation of double antiplatelet therapy one year after stenting. Randomisation avant implantation d’un stent actif. Groupe 1 : Bras Monitoré. -Evaluation systématique de la réponse biologique à l’aspirine et au clopidogrel avant la mise en place de l’endoprothèse active. 2-Adaptation du traitement antiplaquettaire chez les hypo-répondeurs au moment de l’angioplastie. 3-Réévaluation chez tous les patients à J30±3 de la. réponse au traitement antiplaquettaire oral et ajustement du de la dose d’entretien. Groupe 2 : Bras Conventionnel. - Pas d’évaluation de la réponse biologique au traitement antiplaquettaire. - La stratégie antiplaquettaire orale est laissée à la discrétion de l’investigateur en fonction des pratiques habituelles. Evaluation du critère primaire de jugement tous les 6 mois (6 jusqu’à 18 mois) Toute cause de mortalité. Infarctus du myocard. Toute revascularisation urgente. Thrombose de stent nécessitant une revascularisation ou non. AVC ischémique nécessitant une nouvelle hospilisation. PHAO 2008 ARCTIC (Essai n° P080403)- Promoteur AP-HP.")
37
Algorithme d’ajustement de la dose
Patient prévu pour angioplastie élective avec DES et prétraité par aspirine et clopidogrel (pratiques locales) et randomisés dans le “bras monitoring” VerifyNow avant PCI : TM-Aspirin &Clopidogrel ARU≥550 (cartouche ASA) %inh≤15% ou PRU≥235 ( cartouche P2Y12) Recharge avec 500 mg ASA doses d’entretien au choix Inhibiteurs de la GPIIb/IIIa + recharge en clopidogrel ( mg) et dose d’entretien à 150 mg J30 TM-Aspirin & Clopidogrel tous les patients ARU≥550 (cartouche ASA) %inh≤15% ou PRU≥235(cartouche P2Y12) Aspirine à 200 mg et fractionner clopidogrel sans limite supérieure 37
 et randomisés dans le bras monitoring VerifyNow avant PCI : TM-Aspirin &Clopidogrel. ARU≥550 (cartouche ASA) %inh≤15% ou PRU≥235 ( cartouche P2Y12) Recharge avec 500 mg ASA. doses d’entretien au choix. Inhibiteurs de la GPIIb/IIIa + recharge en clopidogrel ( mg) et dose d’entretien à 150 mg. J30 TM-Aspirin & Clopidogrel tous les patients. ARU≥550 (cartouche ASA) %inh≤15% ou PRU≥235(cartouche P2Y12) Aspirine à 200 mg et fractionner. clopidogrel sans limite supérieure. 37.")
38
Les nouveaux 38

39
Biotransformation and mode of action

40
Platelet Aggregation at 4 hours
100 90 300mg ISAR-CHOICE – Von Beckerhat et al .Circulation 2005 ALBION – Montalescot et al. JACC 2007 RELOAD – Collet et al. Circulation 2008 DIPSERSE 2 – Storey et al. JACC 2007 PRINCIPLE TIMI-44 – Wiviot et al. Circulation 2007 80 600mg 70 900mg 60 50 10mg 40 90mg 60mg 30 180mg CURE CURRENT PLATO 20 TRITON 10 Clopidogrel Ticagrelor Prasugrel

41
Study Design, Flow and Compliance
25,087 ACS Patients (UA/NSTEMI 70.8%, STEMI 29.2%) Planned Early (<24 h) Invasive Management with intended PCI Ischemic ECG Δ (80.8%) or ↑cardiac biomarker (42%) Randomized to receive (2 X 2 factorial): CLOPIDOGREL: Double-dose (600 mg then150 mg/d x 7d then 75 mg/d) vs Standard dose (300 mg then 75 mg/d) ASA: High Dose ( mg/d) vs Low dose ( mg/d) Angio 24,769 (99%) No PCI 7,855 (30%) PCI 17,232 (70%) No Sig. CAD 3,616 CABG 1,809 CAD 2,430 Compliance: Clop in 1st 7d (median) 7d d d d Efficacy Outcomes: CV Death, MI or stroke at day 30 Stent Thrombosis at day 30 Safety Outcomes: Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup: PCI v No PCI Complete Followup 99.8%
 Planned Early (<24 h) Invasive Management with intended PCI. Ischemic ECG Δ (80.8%) or ↑cardiac biomarker (42%) Randomized to receive (2 X 2 factorial): CLOPIDOGREL: Double-dose (600 mg then150 mg/d x 7d then 75 mg/d) vs Standard dose (300 mg then 75 mg/d) ASA: High Dose ( mg/d) vs Low dose ( mg/d) Angio 24,769 (99%) No PCI 7,855 (30%) PCI 17,232 (70%) No Sig. CAD 3,616. CABG 1,809. CAD 2,430. Compliance: Clop in 1st 7d (median) 7d 7 d 2 d 7d. Efficacy Outcomes: CV Death, MI or stroke at day 30. Stent Thrombosis at day 30. Safety Outcomes: Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup: PCI v No PCI. Complete Followup 99.8%")
42
PLATO study design NSTE-ACS (moderate-to-high risk) STEMI (if primary PCI) Clopidogrel-treated or -naive; randomised within 24 hours of index event (N=18,624) Clopidogrel If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor 180 mg loading dose, then 90 mg bid maintenance; (additional 90 mg pre-PCI) 6–12-month exposure Primary endpoint: CV death + MI + Stroke Primary safety endpint: Total major bleeding PCI = percutaneous coronary intervention; ASA = acetylsalicylic acid; CV = cardiovascular; TIA = transient ischaemic attack
 Clopidogrel. If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor. 180 mg loading dose, then. 90 mg bid maintenance; (additional 90 mg pre-PCI) 6–12-month exposure. Primary endpoint: CV death + MI + Stroke. Primary safety endpint: Total major bleeding. PCI = percutaneous coronary intervention; ASA = acetylsalicylic acid; CV = cardiovascular; TIA = transient ischaemic attack.")
43
TRITON R 100% 99% PLATO R 81% 64.3% CURRENT R 99% 70% n= 13,608
Prasugrel LD 60mg + MD 10mg TRITON R Angiograpy PCI n= 13,608 100% 99% Clopidogrel LD 300mg + MD 75mg Ticagrelor 180mg + MD 90mgx2 PLATO R Angiograpy PCI n= 18,624 81% 64.3% Clopidogrel LD 300mg + MD 75mg Clopidogrel LD 600mg (16%) Clopidogrel LD 600mg + MD 150mg CURRENT R Angiograpy PCI n= 25,087 99% 70% Clopidogrel LD 300mg + MD 75mg
 Clopidogrel LD 600mg + MD 150mg. CURRENT. R. Angiograpy. PCI. n= 25, % 70% Clopidogrel LD 300mg + MD 75mg.")
44
Baseline and index event characteristics
CURE (n=12,562) TRITON (n=13,608) PLATO (n=18,624) CURRENT (n=25,087) Median age, years 64.2 61.0 62.0 - Women, % 38.5 26 28.4 24.5 CV risk factors, % Habitual smoker Hypertension Dyslipidaemia Diabetes mellitus BMI 60.8 59 na 22.6 38 64 56 23 28 35.8 65.4 46.6 25.0 27 37 22.2 History, % Myocardial Infarction Percutaneous coronary intervention Coronary-artery bypass grafting 32.2 17.7* * 18 13.1 7.5 20.5 13.3 6.0 Clinical Presentation % Unstable angina or NSTEMI STEMI TIMI Risk Score >3 TIMI Risk Score >5 74.9 25.1 33.3 74 62.3 37.7 44.6 20.6 70.8 29.2 ECG at entry, % Persistent ST-segment elevation ST-segment depression 42.2 37.6 51.0 Troponin-I positive (all population) % Troponin-I positive (UA or NSTEMI) % 25.3 ? 85.7 81.0 40
 TRITON. (n=13,608) PLATO. (n=18,624) CURRENT. (n=25,087) Median age, years Women, % CV risk factors, % Habitual smoker. Hypertension. Dyslipidaemia. Diabetes mellitus. BMI na History, % Myocardial Infarction. Percutaneous coronary intervention. Coronary-artery bypass grafting * * Clinical Presentation % Unstable angina or NSTEMI. STEMI. TIMI Risk Score >3. TIMI Risk Score > ECG at entry, % Persistent ST-segment elevation. ST-segment depression Troponin-I positive (all population) % Troponin-I positive (UA or NSTEMI) %")
45
Study medication CURE (n=12,562) TRITON (n=13,608) PLATO (n=18,624)
CURRENT (n=25,087) Start of randomised treatment Time after start of chest pain, h, median - 11.3 Compliance, % Premature discontinuation of study drug Premature discontinuation of control 23.4 21.5 Concomitent antithrombotic, % Clopidogrel in hospital before randomisation Loading dose of clopidogrel ≥ 600mg Study-drug administration before PCI GP IIbIIIa Inhibitor 25.5 54.5 46.1 16.6 ? * 26.6 ? 28.6 Invasive procedures at index hospitalisation, % Planned invasive treatment Coronary angiography PCI during index hospitalisation Cardiac surgery 100 99 2.5 72.0 81.5 61.0 4.5 70 10
 Start of randomised treatment. Time after start of chest pain, h, median Compliance, % Premature discontinuation of study drug. Premature discontinuation of control Concomitent antithrombotic, % Clopidogrel in hospital before randomisation. Loading dose of clopidogrel ≥ 600mg. Study-drug administration before PCI. GP IIbIIIa Inhibitor * Invasive procedures at index hospitalisation, % Planned invasive treatment. Coronary angiography. PCI during index hospitalisation. Cardiac surgery")
46
Benefits of Antiplatelet Therapy in ACS
are Greater in Patients Undergoing PCI Relative Risk Reduction PCI No PCI CURE: Clopidogrel 300/75 mg v Placebo (CVD/MI) 30%1 19%2 STEMI: Clopidogrel 300/75 mg v Placebo (CVD/MI) 46%3 9%4 TRITON: Prasugrel v Clopidogrel 300/75mg (CVD/MI/Stroke) 19%5 Not evaluated PLATO : Ticagrelor v Clopidogrel 300/75mg (CVD/MI/Stroke) 16%6 15%*NS CURRENT : Clopidogrel 600/150 v 300/75mg (CVD/MI/Stroke) 15%7 deleterious ?+17%*p=0.14 1. Mehta SR, et al. Lancet 2001; 358(9281): 2. Fox KAA, et al. Circulation 2004;110:1202-8 3. Sabatine MS, et al. JAMA 2005; 294(10): 4. Chen ZM Lancet 2005;366: 4. Boersma E et al. Lancet 2002; 359:189 5. Wiviott S et al. N Engl J Med ; 357: 2001–15. 6. Wallentin L et al. N Engl J Med 2009 7. Metha et al. presented at the ESC09
 30%1. 19%2. STEMI: Clopidogrel 300/75 mg v Placebo (CVD/MI) 46%3. 9%4. TRITON: Prasugrel v Clopidogrel 300/75mg (CVD/MI/Stroke) 19%5. Not evaluated. PLATO : Ticagrelor v Clopidogrel 300/75mg (CVD/MI/Stroke) 16%6. 15%*NS. CURRENT : Clopidogrel 600/150 v 300/75mg (CVD/MI/Stroke) 15%7. deleterious +17%*p= Mehta SR, et al. Lancet 2001; 358(9281): Fox KAA, et al. Circulation 2004;110: Sabatine MS, et al. JAMA 2005; 294(10): Chen ZM Lancet 2005;366: Boersma E et al. Lancet 2002; 359: Wiviott S et al. N Engl J Med ; 357: 2001– Wallentin L et al. N Engl J Med Metha et al. presented at the ESC09.")
47
Primary endpoint = CV Death / MI / Stroke 12-15 months
TRITON and PLATO Primary endpoint = CV Death / MI / Stroke months 15 12.1 9.9 Prasugrel 10mg Clopidogrel 75mg HR 0.81 ( ) p=0.0004* 9.8 11.7 Ticagrelor 90mg x2 HR 0.84 (0.77–0.92) p=0.0003* 10 Endpoint (%) 5 30 60 90 180 270 360 450 days
 p=0.0004* Ticagrelor 90mg x2. HR 0.84 (0.77–0.92) p=0.0003* 10. Endpoint (%) days.")
48
TRITON, PLATO and CURRENT EARLY CV Death / MI / Stroke (30days)
8 7.1% (Clopidogrel 75 TRITON) 5.6% 5.6% (Prasugrel TRITON) Prasugrel 60mg + 10mg 4.7% HR 0.77 (95% CI 0.67–0.88), p<0.001* Clopidogrel 75mg vs Prasugrel 10mg - 23% Clopidogrel 300mg + 75mg 6 Ticagrelor 180mg + 90mg x2 4.8 % (Ticagrelor PLATO) 5.4 % (Clopidogrel 75 PLATO) HR 0.88 (95% CI 0.77–0.95), p=0.045* Clopidogrel 75mg vs Ticagrelor 90mg x2 - 12% Clopidogrel 600mg + 150mg 4.2 % (Clopidogrel 150 CURRENT) 4.4 % (Clopidogrel 75 CURRENT) HR 0.96 (95% CI ), p=0.47 Clopidogrel 75mg vs Clopidogrel 150mg - 4% 4 Cumulative incidence (%) 2 10 20 30 days
 5.6% 5.6% (Prasugrel TRITON) Prasugrel 60mg + 10mg. 4.7% HR 0.77 (95% CI 0.67–0.88), p<0.001* Clopidogrel 75mg vs. Prasugrel 10mg. - 23% Clopidogrel 300mg + 75mg. 6. Ticagrelor 180mg + 90mg x % (Ticagrelor PLATO) 5.4 % (Clopidogrel 75 PLATO) HR 0.88 (95% CI 0.77–0.95), p=0.045* Clopidogrel 75mg vs. Ticagrelor 90mg x % Clopidogrel 600mg + 150mg. 4.2 % (Clopidogrel 150 CURRENT) 4.4 % (Clopidogrel 75 CURRENT) HR 0.96 (95% CI ), p=0.47. Clopidogrel 75mg vs. Clopidogrel 150mg. - 4% 4. Cumulative incidence (%) days.")
49
LATE CV Death / MI / Stroke (30- 360 days)
TRITON and PLATO LATE CV Death / MI / Stroke ( days) Clopidogrel 75mg Prasugrel 10mg 8 6.9 6.6 6 Ticagrelor 90mg x2 5.6 5.3 Cumulative incidence (%) 4 HR 0.80 (95% CI 0.70–0.91), p=0.003* (TRITON) 2 HR 0.80 (95% CI 0.70–0.91), p< (PLATO) 31 90 150 210 270 330 390 450
 Clopidogrel 75mg. Prasugrel 10mg Ticagrelor 90mg x Cumulative incidence (%) 4. HR 0.80 (95% CI 0.70–0.91), p=0.003* (TRITON) 2. HR 0.80 (95% CI 0.70–0.91), p<0.001 (PLATO)")
50
All cause Mortality (12-15 months)
9 Ticagrelor Clopidogrel 150 Clopidogrel 75 Prasugrel p=NS p=0.62 p<0.001 8 -9% - 5% -22% 7 6.2 5.9 5.8 6 4.5 K-M estimated rate 5 p=0.6 3.2 4 - 4% 3.0 3 2.2 2.1 2 ASA only 1 TRITON PLATO CURE CURRENT 30 days and CV deaths only ! 360 days 450 days 360 days

51
Stent Thrombosis (12-15 months)
2.4% vs 1.1% (142/68) 2.3% vs 1.6% (199 vs 136) Hazard Ratio 2.8% vs 2.1 (158/118) Significant reductions both with BMS, DES Significant reductions in early and late stent thromboses
 2.3% vs 1.6% (199 vs 136) Hazard Ratio. 2.8% vs 2.1. (158/118) Significant reductions both with BMS, DES. Significant reductions in early and late stent thromboses.")
52
Safety = TIMI Major Non-CABG Bleeds (12-15 months)
9 Ticagrelor Clopidogrel 150 Clopidogrel 75 Prasugrel 8 7 6 p=0.001* p=0.03* p=0.025* K-M estimated rate 5 +27% +25% +22% 3.7 30 days ! 4 2.7 2.8 3 2.4 2.2 1.8 2 1.04 0.95 ASA only 1 TRITON PLATO CURE CURRENT 360 days 450 days 360 days

53
Safety = (12-15 months) Fatal Bleeds Intracranial Bleeds +0% +75% +0%
9 Ticagrelor Clopidogrel 150 Clopidogrel 75 Prasugrel 8 7 6 Fatal Bleeds Intracranial Bleeds K-M estimated rate 5 4 p=NS p=0.002* p=0.66 p=0.74 p=0.06 +0% +75% +0% +0% +33% 3 2 1 0.4 0.3 0.2 0.1 ? TRITON PLATO CURE TRITON PLATO CURE 450 days

54
Safety = Life-threatening Bleeds (12-15 months)
9 Ticagrelor Clopidogrel 150 Clopidogrel 75 Prasugrel 8 p=0.7 +0% 7 5.8 5.8 6 p=0.01* p=0.13 K-M estimated rate 5 +19% +55% 4 DEFINITION Rate of CABG! 3 2.2 Pour PLATO = CABG + non CABG patients Pour les autres CURE et TRITON = les CABG patients étaient-ils inclus ? 1.8 2 1.4 1 0.9 TRITON PLATO CURE 360 days 450 days 360 days

55
Le futur proche 55

56
Les Enjeux Pratiques du Futur
Le switch Le préhospitalier La place des anti-IIb/IIIa? Le NSTEMI Les sujets fragiles Les coûts

57
The ACAPULCO Study * * p = 0.003 vs. clopidogrel 900 mg
A Randomized, Double-Blind, Crossover Study Comparing the Pharmacodynamic Response in Subjects with Acute Coronary Syndrome Receiving 14 Days of 10-mg Maintenance Dose Prasugrel versus 14 Days of 150-mg Maintenance Dose Clopidogrel After Using a 900-mg Loading Dose of Clopidogrel to Reduce Ongoing Platelet Activation Maximal Platelet Aggregation (%) (20 µM ADP) Pre-LD Post-LD Visit 3 (day 15) Visit 4 (day 29) Clopidogrel 150 mg Prasugrel 10 mg * * p = vs. clopidogrel 900 mg (n = 32) Prasugrel Clopidogrel n = 19 Clopidogrel Prasugrel n = 18 10 20 30 40 50 60 70 80 90 Clopidogrel 900 mg p = 0.016 p = 0.001
 (20 µM ADP) Pre-LD. Post-LD. Visit 3 (day 15) Visit 4 (day 29) Clopidogrel 150 mg. Prasugrel 10 mg. * * p = vs. clopidogrel 900 mg. (n = 32) Prasugrel Clopidogrel. n = 19. Clopidogrel Prasugrel. n = Clopidogrel 900 mg. p = p =")
58
Net Clinical Benefit Bleeding Risk Subgroups
Post-hoc analysis Risk (%) Yes + 37 Prior Stroke / TIA -16 No Pint = 0.006 -1 >=75 Age Pint = 0.18 -16 < 75 < 60 kg +3 Wgt >=60 kg Pint = 0.36 -14 -13 OVERALL 0.5 1 2 Prasugrel Better Clopidogrel Better HR
 Yes Prior Stroke / TIA No. Pint = >=75. Age. Pint = < 75. < 60 kg. +3. Wgt. >=60 kg. Pint = OVERALL Prasugrel Better. Clopidogrel Better. HR.")
59
Days From Randomization
TRITON-TIMI 38: Patients Age<75 and Weight ≥60 and no history of TIA/stroke Hazard Ratio, 0.745 (95% CI, ) P<0.001 11% Clopidogrel Endpoint (%) 8.4% Prasugrel Hazard Ratio, 1.240 (95% CI, ) P=0.170 Q8145 and Q8146 Prasugrel 1.95% 1.50% Clopidogrel 30 90 180 270 360 450 Days From Randomization CI=confidence interval
 P< % Clopidogrel. Endpoint (%) 8.4% Prasugrel. Hazard Ratio, (95% CI, ) P= Q8145 and Q8146. Prasugrel. 1.95% 1.50% Clopidogrel Days From Randomization. CI=confidence interval.")
60
Net Clinical Benefit after 1 year
Aspirin alone ST: 0.5% Death, MI, stroke (ST not considered): 4% Major bleed: 0.5% Dual OAT (aspirin and clopidogrel) ST: 0.35% Death, MI, stroke (ST not considered): 3% Major bleed: 0.6% Dual OAT (apirin and prasugrel) ST: 0.20% Death, MI, stroke (ST not considered): 2.5% Major bleed: 0.8% 5% 4% 3.5%
: 4% Major bleed: 0.5% Dual OAT (aspirin and clopidogrel) ST: 0.35% Death, MI, stroke (ST not considered): 3% Major bleed: 0.6% Dual OAT (apirin and prasugrel) ST: 0.20% Death, MI, stroke (ST not considered): 2.5% Major bleed: 0.8% 5% 4% 3.5%")
Présentations similaires




 % de la.>")



 1-IEC 2-B Bloquant 3-ARA 2 4-Anti-aldostérone.>")

en péri-opératoire>")








