Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Fermeture d’appendice auriculaire
S. Armero Service Pr Paganelli

2
Indication reconnue en France
ACFA + facteurs de risque thromboembolique et contre indication à ce traitement (hémorragie digestive majeure, AVC hémorragique).
.")
3
Protect-AF trial 800 patients Randomisation: 2:1
Suivi avec ETT à 45j, 6 mois et 1 an. 87% d’arrêt de la warfarin Critère primaire d’efficacité: - AVC, Décés, embols systémique Critère primaire de sécurité: Migration de la prothèse Tamponade Saignement Resultats: Critère primaire: -Reduction significative du risque de 32% (4.9%→3%=) 1 Conclusion: - Réduction du risque d’AVC, non infériorité sur le critère primaire Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial David R Holmes, Vivek Y Reddy, Zoltan G Turi, Shephal K Doshi, Horst Sievert, Maurice Buchbinder, Christopher M Mullin, Peter Sick, for the PROTECT AF Investigators Lancet 2009; 374: 534–42 Summary Background In patients with non-valvular atrial fi brillation, embolic stroke is thought to be associated with left atrial appendage (LAA) thrombi. We assessed the efficacy and safety of percutaneous closure of the LAA for prevention of stroke compared with warfarin treatment in patients with atrial fibrillation. Methods Adult patients with non-valvular atrial fi brillation were eligible for inclusion in this multicentre, randomised non-inferiority trial if they had at least one of the following: previous stroke or transient ischaemic attack, congestive heart failure, diabetes, hypertension, or were 75 years or older. 707 eligible patients were randomly assigned in a 2:1 ratio by computer-generated randomisation sequence to percutaneous closure of the LAA and subsequent discontinuation of warfarin (intervention; n=463) or to warfarin treatment with a target international normalised ratio between 2·0 and 3·0 (control; n=244). Effi cacy was assessed by a primary composite endpoint of stroke, cardiovascular death, and systemic embolism. We selected a one-sided probability criterion of non-inferiority for the intervention of at least 97·5%, by use of a two-fold non-inferiority margin. Serious adverse events that constituted the primary endpoint for safety included major bleeding, pericardial eff usion, and device embolisation. Analysis was by intention to treat. This study is registered with Clinicaltrials.gov, number NCT Findings At 1065 patient-years of follow-up, the primary effi cacy event rate was 3·0 per 100 patient-years (95% credible interval [CrI] 1·9–4·5) in the intervention group and 4·9 per 100 patient-years (2·8–7·1) in the control group (rate ratio [RR] 0·62, 95% CrI 0·35–1·25). The probability of non-inferiority of the intervention was more than 99·9%. Primary safety events were more frequent in the intervention group than in the control group (7·4 per 100 patient-years, 95% CrI 5·5–9·7, vs 4·4 per 100 patient-years, 95% CrI 2·5–6·7; RR 1·69, 1·01–3·19). Interpretation The efficacy of percutaneous closure of the LAA with this device was non-inferior to that of warfarin therapy. Although there was a higher rate of adverse safety events in the intervention group than in the control group, events in the intervention group were mainly a result of periprocedural complications. Closure of the LAA might provide an alternative strategy to chronic warfarin therapy for stroke prophylaxis in patients with non-valvular atrial fibrillation. Holmes DR: ACC & i2 Summit 2009 Holmes et al., Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with AF: a randomized non-inferiority trial, Lancet 2009; 374: 534–42
 1. Conclusion: - Réduction du risque d’AVC, non infériorité sur le critère primaire. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. David R Holmes, Vivek Y Reddy, Zoltan G Turi, Shephal K Doshi, Horst Sievert, Maurice Buchbinder, Christopher M Mullin, Peter Sick, for the. PROTECT AF Investigators. Lancet 2009; 374: 534–42. Summary. Background In patients with non-valvular atrial fi brillation, embolic stroke is thought to be associated with left atrial appendage (LAA) thrombi. We assessed the efficacy and safety of percutaneous closure of the LAA for prevention of stroke compared with warfarin treatment in patients with atrial fibrillation. Methods Adult patients with non-valvular atrial fi brillation were eligible for inclusion in this multicentre, randomised non-inferiority trial if they had at least one of the following: previous stroke or transient ischaemic attack, congestive heart failure, diabetes, hypertension, or were 75 years or older. 707 eligible patients were randomly assigned in a 2:1 ratio by computer-generated randomisation sequence to percutaneous closure of the LAA and subsequent discontinuation of warfarin (intervention; n=463) or to warfarin treatment with a target international normalised ratio between 2·0 and 3·0 (control; n=244). Effi cacy was assessed by a primary composite endpoint of stroke, cardiovascular death, and systemic embolism. We selected a one-sided probability criterion of non-inferiority for the intervention of at least 97·5%, by use of a two-fold non-inferiority margin. Serious adverse events that constituted the primary endpoint for safety included major bleeding, pericardial eff usion, and device embolisation. Analysis was by intention to treat. This study is registered with Clinicaltrials.gov, number NCT Findings At 1065 patient-years of follow-up, the primary effi cacy event rate was 3·0 per 100 patient-years (95% credible interval [CrI] 1·9–4·5) in the intervention group and 4·9 per 100 patient-years (2·8–7·1) in the control group (rate ratio [RR] 0·62, 95% CrI 0·35–1·25). The probability of non-inferiority of the intervention was more than 99·9%. Primary safety events were more frequent in the intervention group than in the control group (7·4 per 100 patient-years, 95% CrI 5·5–9·7, vs 4·4 per 100 patient-years, 95% CrI 2·5–6·7; RR 1·69, 1·01–3·19). Interpretation The efficacy of percutaneous closure of the LAA with this device was non-inferior to that of warfarin therapy. Although there was a higher rate of adverse safety events in the intervention group than in the control group, events in the intervention group were mainly a result of periprocedural complications. Closure of the LAA might provide an alternative strategy to chronic warfarin therapy for stroke prophylaxis in patients with non-valvular atrial fibrillation. Holmes DR: ACC & i2 Summit Holmes et al., Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with. AF: a randomized non-inferiority trial, Lancet 2009; 374: 534–42.")
4
Device Event Rate (95% CI) Control Event Rate (95% CI)
Proof of Concept (2) PROTECT – AF: Updated Data (Bayesian sequential design) Primary Safety Results End Point Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort 48 8.7 ( ) 13 4.2 ( ) 2.08 ( ) Primary Efficacy Results End Point Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort 20 3.4 ( ) 16 5.0 ( ) 0.68 ( ) All Stroke, HS, and IS by Intervention End Point Device Event Rate (95% CI) Control Event Rate (95% CI) Relative Risk (95% CI) All Stroke 2.6 ( ) 3.5 (1.7 – 5.7) 0.74 (0.36 – 1.76) IS 2.4 (1.3 – 3.9) 1.6 (0.5 – 3.1) 1.53 (0.654 – 5.43) HS 0.2 ( ) 1.9 (0.7 – 3.7) 0.09 (0.00 – 0.45) Holmes, i2 Summit - Protect AF Trial - Intermediate-Term Outcome , J. Am. Coll. Cardiol. 2010;55;A181.E1698
 PROTECT – AF: Updated Data (Bayesian sequential design) Primary Safety Results. End Point. Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort ( ) ( ) 2.08 ( ) Primary Efficacy Results. End Point. Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort ( ) ( ) 0.68 ( ) All Stroke, HS, and IS by Intervention. End Point. Device Event Rate (95% CI) Control Event Rate (95% CI) Relative Risk (95% CI) All Stroke. 2.6 ( ) 3.5 (1.7 – 5.7) 0.74 (0.36 – 1.76) IS. 2.4 (1.3 – 3.9) 1.6 (0.5 – 3.1) 1.53 (0.654 – 5.43) HS. 0.2 ( ) 1.9 (0.7 – 3.7) 0.09 (0.00 – 0.45) Holmes, i2 Summit - Protect AF Trial - Intermediate-Term Outcome , J. Am. Coll. Cardiol. 2010;55;A181.E1698.")
6
3 Serious pericardial effusions
Pericardial tamponade treated by surgical intervention and device was found to have embolized on TEE at D86 and retrieved in the cath lab from the descending aorta Cardiac perforation treated by pericardiocentesis Pericardial effusion not intervened, pt died at D22 (NYHA III, CHADS2>5: AF/VT -> LV failure) 3 Device Embolizations (all in first series of cases, prior to retraining) 2 – Surgery, pts died after surgery (1: myocardiac failure, post perfusion, 1: retroperitioneal) 1 – Snared and new device implanted 5 Thrombus: After 30 days 1 After 66 days 1 After 6 months 3
 3 Device Embolizations (all in first series of cases, prior to retraining) 2 – Surgery, pts died after surgery (1: myocardiac failure, post perfusion, 1: retroperitioneal) 1 – Snared and new device implanted. 5 Thrombus: After 30 days 1. After 66 days 1. After 6 months 3.")
7
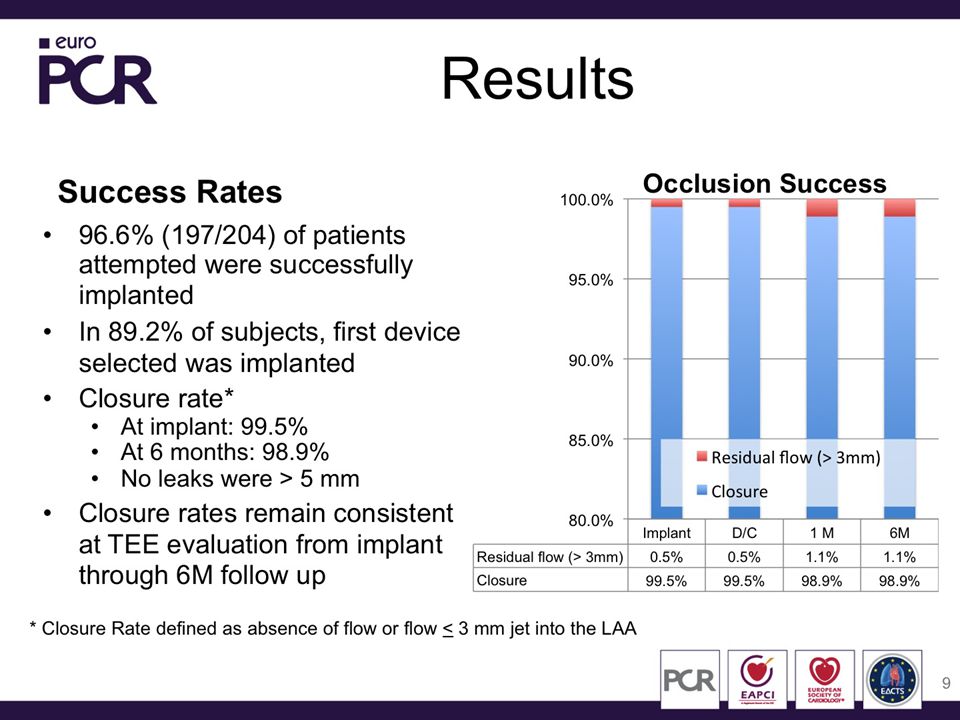
The estimated stroke rate is a per patient calculation wherein each patient serves as his own control; versus the CHADS 2 score (GAGE) Despite the fact that these data are not from a randomized clinical cohort, the relative risk reduction is quite meaningful and consistent with other publications (PLAATO OSTERMAYER-2005, BLOCK, and Watchman ASAP – REDDY, HRS, Late Breaking 2012)
")
9
Technique Procédure de cardiologie interventionnelle échoguidée par voie veineuse femorale (puis trans-septal) Occlusion par prothèse autoexpendable en nitinol adapatée à la mesure angio et ETO de l’auricule Vérification par angio et ETO de l’efficacité de la fermeture

10
Cas clinique M. B Homme 71 ans ACFA CHADS VASC >2
Actd AVC Hémorragique 2006 Actd Pontage aortocoronaire 1995 puis ACT+ Stent Fdr Cv: Diabète, Dyslipidémie, Tabac sevré

14
Prothèse larguée en ETO

15
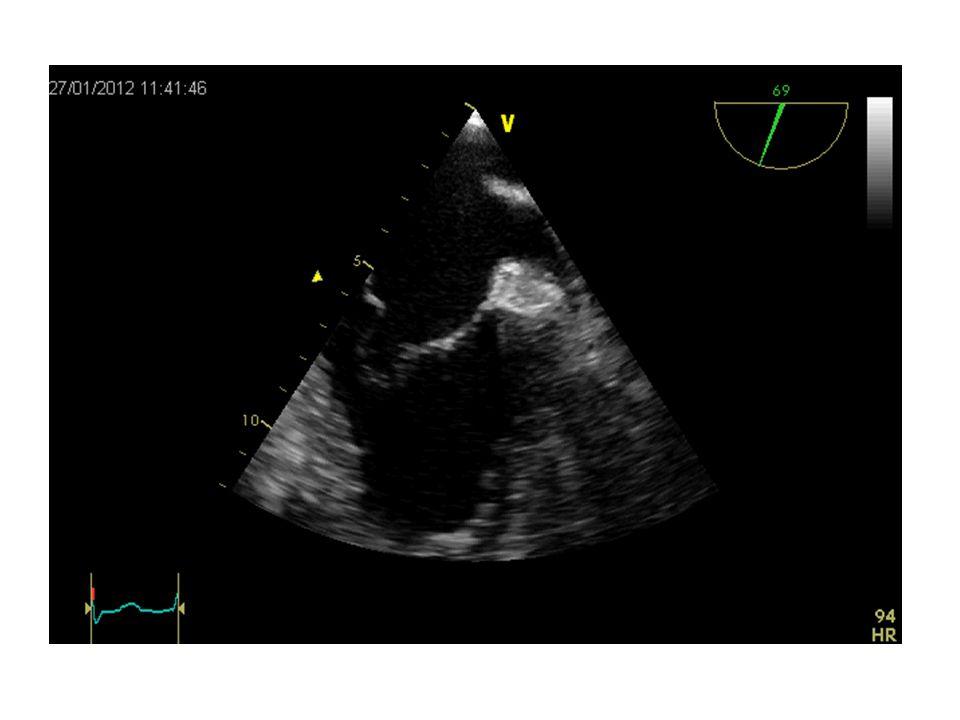
Ôpacification de l’appendice auriculaire à l’aide d’un pic tail

16
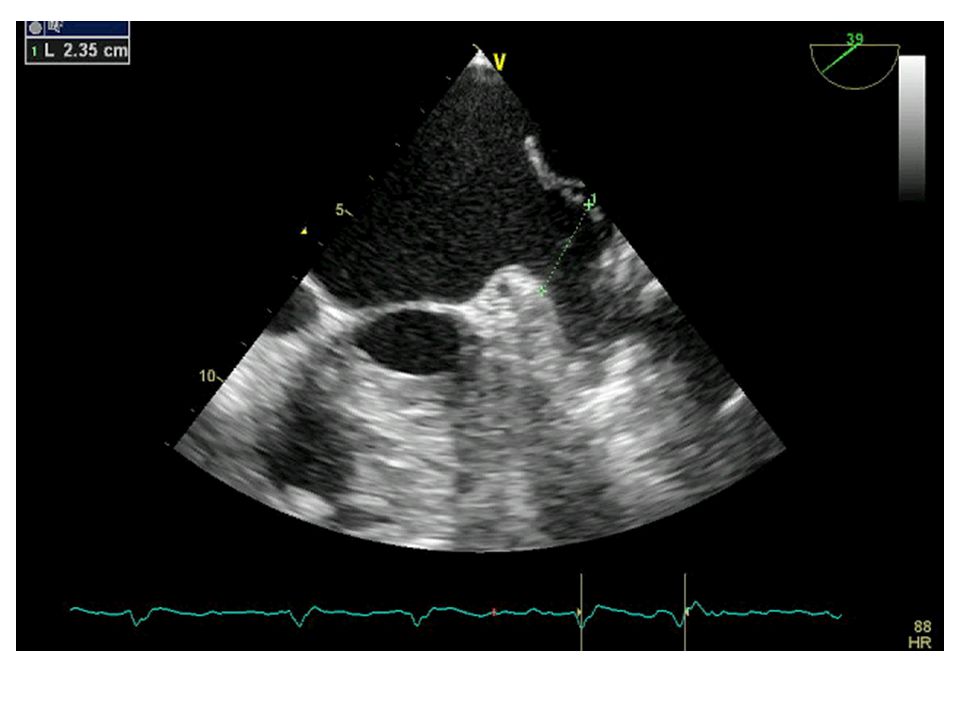
Premier positionnement
Prothèse implantée trop profondement

17
2eme positionnement prothèse encore positionnée de manière trop profonde (Waist)
")
18
Meilleur positionnement

19
Prothèse larguée

20
Conclusion Technique intéressante chez les patients à haut rique ischémique et à haut rique hémorragique

Présentations similaires













 versus CLB + rituximab (R)>")


>")
>")


