Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
DESC REANIMATION MEDICALE Février 2008 A.Gentilhomme
Pronostic des PAVM DESC REANIMATION MEDICALE Février 2008 A.Gentilhomme

2
Fréquence PAVM complique 8 à 28 % des sujets ventilés
Am J Med 1981,Haley ,Nosocomial infections in US hospitals Am J Infect Control 1999,NNIS

3
Fréquence de survenue 3%/J de J0 à J5 2%/J de J5 à J10 1%/J après J10
Ann Intern Med 1998,Brun Buisson,Incidence and risk factor of VAP…

4
Allonge la durée de séjour
de 22 jours en USI de 25 jours à l’hôpital Crit Care Med ,2003,Kollef,Outcome and attributable cost of VAP among intensive care units patients in a suburban medical center

5
Durée de séjour Crit Care Med ,2003,Kollef,Outcome and attributable
cost of VAP among intensive care units patients in a suburban medical center

6
Mortalité La plus élevée parmi celles des infections nosocomiales
American thoracic society 1995,HAP in adults:diagnosis,assessment of severity,initial antimicrobial therapy and preventive strategy

7
Mais variable selon les études Am J Respir Crit Care Med,2002,Chastre

8
Mortalité attribuable
Définition: % de DC évités en l’absence de PAVM 1/3 à 1/2 des DC dus à la PAVM Am J Respir Crit Care Med 1996.American thoracic society.HAP in adults..

9
Mortalité attribuable
Mortalité patient USI avec VAP = 2 à 10 fois mortalité patient USI sans VAP 50% DC si VAP(+) vs 4% si VAP (-) Arch internmed 1974,Stevens,pneumonia in an intensive care unit .30 month experience
 vs 4% si VAP (-) Arch internmed 1974,Stevens,pneumonia in an intensive care unit .30 month experience.")
10
PAVM: facteur indépendant de mortalité OUI! 5/8
Am J Respir Crit Care Med 2002,State of the Art

11
PAVM :facteur indépendant de mortalité? NON 3/8
(108 patients appariés 39PAV ds chq grpe) Anesthesiology 2001,Papazian, Is VAP an independent risk factor for death?
 Anesthesiology 2001,Papazian, Is VAP an independent risk factor for death")
12
Discordance car.. L’apparition de la PAVM et la mortalité sont multi-facteurs dépendantes Le diagnostic certain de PAVM reste difficile à poser BIAIS / Mortalité attribuable?…

13
Tout d’abord la gravité du terrain
Favorise l’émergence de la PAVM et son issue fatale

14
. Chest 1988,Torres A, Nosocomial pneumonia.
A multivariate analysis of risk and prognosis .

15
Ensuite l’apparition tardive
Chest 1995,Kollef,the effect of late-onset VAP in determining mortality.

16
Puisque souvent correlée ..
à la présence de pathogènes à haut risque de mortalité idem

17
Puis l’antibiothérapie
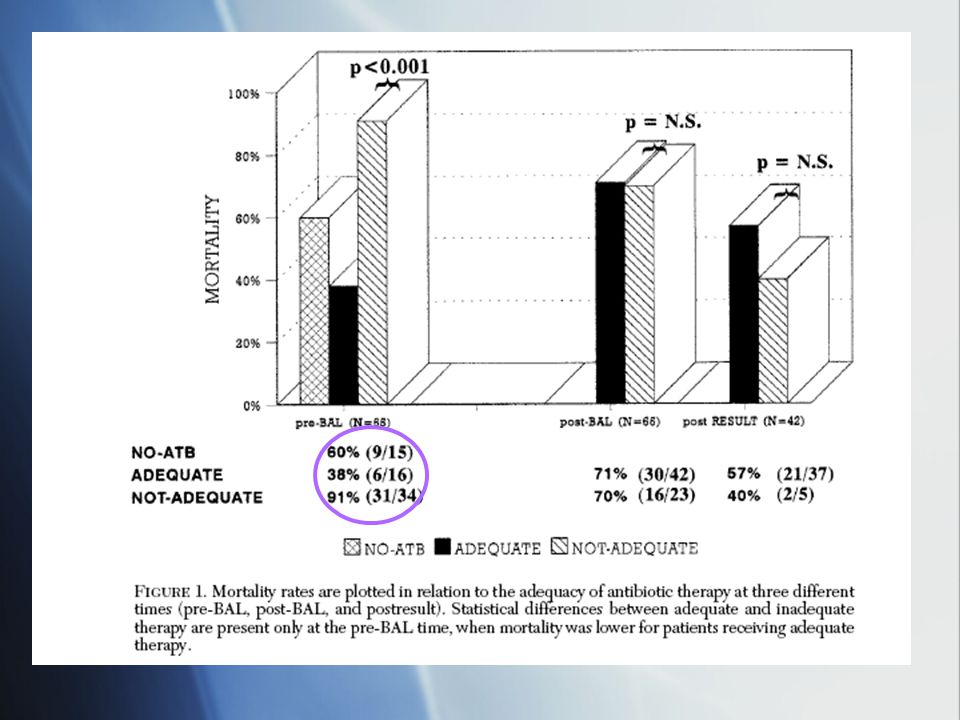
Antibiothérapie empirique pré-LBA Mortalité: - 38% si antibiothérapie adaptée - 91% si inadaptée - 60% si absence Chest 1997,Luna, Impact of BAL on the outcome of VAP

19
Car… Une antibiothérapie empirique inadaptée augmente la mortalité

20
En… Sélectionnant des bactéries résistantes
Am J Respir crit care med 1998,Chastre,VAP caused by potentially drug-resistant bacteria

21
Et plus particulierement…
Pseudomonas Aeruginosa Chest 1996,Croust,VAP due to Ps.Aeruginosa

22
Mais aussi.. Acinetobacter 50 % de mortalité
Chest 2006 clinical characteristics and treatment

23
Et.. SAMR 15 à 30% de mortalité Crit Care Med 2007,Chastre, Early predictors for infection recurrence and death in patients with ventilator-associated pneumonia Chest 2006 clinical characteristics and treatment

24
Mortalité et pathogènes Chest 2006 clinical characteristics and treatment

25
A noter.. Chest 2006, Kollef,Clinical Characteristic and..
Mortalité similaire dans les groupes ou antibiothérapie empirique initiale = carbapeneme,ureidopenicilline, quinolone =30% Mortalité moindre dans le groupe vancomycine 19,1% Chest 2006, Kollef,Clinical Characteristic and..

26
Kollef Chest 2006 Kollef Chest 2006

27
Par ailleurs… Ne diminue pas la mortalité
Int Care Med 2001,Dupont,Impact of appropriateness of initail antibiotic therapy on the outcome of VAP Int Care Med 2001,Dupont,Impact of appropriateness of initail antibiotic therapy on the outcome of VAP

28
…l’antibiothérapie initiale adaptée
Ne diminue pas significativement la mortalité Mais diminue uniquement la durée de séjour Controversée par autres études (Chest 1997, Luna)
")
29
De plus.. Adapter l’antibiothérapie aux résultats du LBA ne modifie pas la mortalité!
Mortalité antibiothérapie adaptée secondairement aux résultats du LBA = Mortalité antibiothérapie empirique inadaptée Chest 1997 Impact of BAL data on the therapy and outcome of VAP

30
Chest 1997,Luna,Impact of BAL on the outcome of VAP

31
Mortalité=f(temps)? Chest 2006, Kollef
 Chest 2006, Kollef")
32
Les « golden hours »? NON Pas de différence significative de mortalité entre une antibiothérapie adaptée instaurée à <H24 ou >H24 Kollef Chest 2006

33
Serait il trop tard? NON!

34
Kollef Chest 2006

35
On note que Désescalade AB mortalité 17%
Pas de modification AB mortalité 23,7% Escalade AB mortalité 42,6% Pour un taux de mortalité globale de 25,1% dans l’étude Kollef Chest 2006

36
On peut penser que .. Si l’antibiothérapie initiale adaptée a peu d’influence sur la mortalité , il serait important d’identifier d’autres facteurs de risque de mortalité

37
Facteurs de gravité Sexe féminin Age >60 ans BGN non fermentant
SAMR Score de gravité élevé au moment de l’apparition de la PAVM Crit Care Med 2007,Chastre,Early predictors for infection recurrence and death in patients with VAP

38
Et.. D’étudier l’effet de la durée de l'antibiothérapie

39
Pas de différence de morbi-mortalité
JAMA 2003,Chastre,Comparaison of 8vs 15 Days of antibiotic therapy for VAP in adults

40
Il faut donc prendre en compte
La gravité initiale de la pathologie sous jacente Le moment d’apparition de la PAVM dans l’HDLM /Le type de pathogène Les caractéristiques du patient Car la PAVM n’est probablement un facteur de risque indépendant de mortalité que chez les patients moyennement graves ou avec un pathogène à haut risque

41
CONCLUSION Nombreuses études discordantes au niveau des résultats
Étudier le patient dans sa globalité En identifiant les facteurs de risque Instaurer une Antibiothérapie empirique à large spectre adéquate autant que faire se peut! Pratiquer une désescalade antibiotique ASAP

Présentations similaires