Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Adénopathies métastatiques
Jean-Pascal Machiels Cliniques Universitaires Saint-Luc Université Catholique de Louvain

2
Adénopathie cervicale
Mr H., 62 ans Tuméfaction cervicale droite

3
Anamnèse AP: Consommation tabagique>40 UAP
Infarctus mésentérique avec péritonite traités chirurgicalement Ulcère gastrique Coma éthylique

4
Depuis 5 mois: masse cervicale gauche indolore
Pas d’AEG ou de symptômes B Signale des lourdeurs épigastriques Pas de traitement au domicile

5
Examen clinique Paramètre nx Souffle syst. 2/6 au FM
Crépitants base pulm. gauche Abdomen: sp Masse mal délimitée indolore non inflammatoire au niveau cervical droit

6
Biologie Normale CEA=8.3 ng/ml (N<3)
")
7
RX thorax normale

8
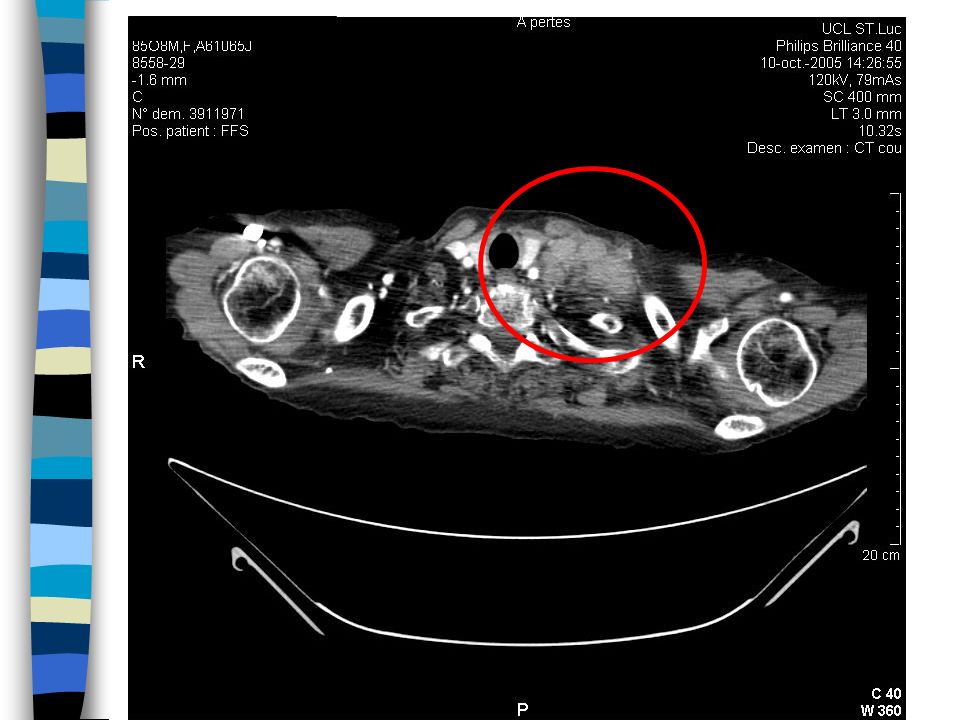
Echographie cervicale
Nombreux ggl le long du SCM (dont certains>2 cm d’axe). Un d’entre eux semble infiltrer le muscle. Certains ggl sont partiellement nécrotiques.
. Un d’entre eux semble infiltrer le muscle. Certains ggl sont partiellement nécrotiques.")
9
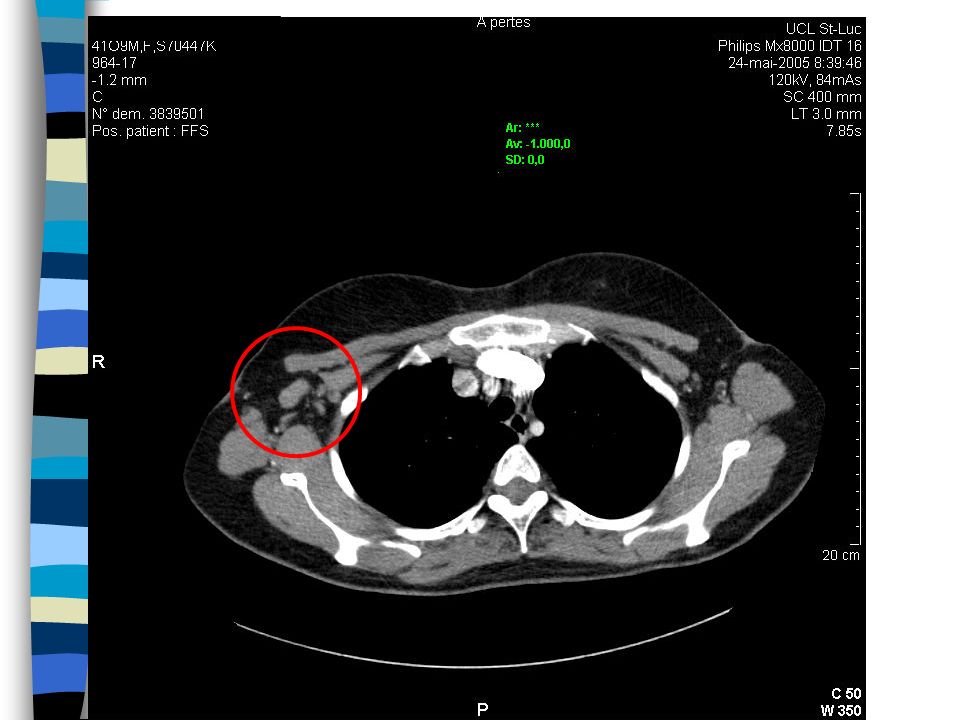
Scanner thoraco-abdominal
Présence de ggl médiastinaux. Au niveau abdo: thrombose de l’artère mésentérique sup avec suppléance via l’arcade de Riolan. Présence de ggl rétropéritonéaux, mésentériques, inguinaux et iliaques, infracm.

11
PET Scanner Adénopathies hypermétaboliques cervicales gauches

12
Fibroscopie ORL Sp à part une compression extrinsèque du pharynx au niveau de sa paroi postérieure à droite

13
Fibroscopie normale Gastroscopie normale

14
Quelle mise au point complémentaire?

15
Exérèse chirurgicale Carcinome peu différencié d’origine indéterminée au niveau cervical droite

16
Evaluation and Management of the Patient with a Neck Mass

17
General Considerations
Patient age Pediatric (0 – 15 years): 90% benign Young adult (16 – 40 years): similar to pediatric Late adult (>40 years): “rule of 80s” Location Congenital masses: consistent in location Metastatic masses: key to primary lesion
: 90% benign. Young adult (16 – 40 years): similar to pediatric. Late adult (>40 years): rule of 80s Location. Congenital masses: consistent in location. Metastatic masses: key to primary lesion.")
18
Differential Diagnosis

19
Diagnostic Steps History Physical Examination
Developmental time course Associated symptoms (dysphagia, otalgia, voice) Personal habits (tobacco, alcohol) Previous irradiation or surgery Physical Examination Complete head and neck exam (visualize & palpate) Emphasis on location, mobility and consistency
 Personal habits (tobacco, alcohol) Previous irradiation or surgery. Physical Examination. Complete head and neck exam (visualize & palpate) Emphasis on location, mobility and consistency.")
20
Empirical Antibiotics
Inflammatory mass suspected Two week trial of antibiotics Follow-up for further investigation

21
Diagnostic Tests Fine needle aspiration biopsy (FNAB)
Computed tomography (CT) Magnetic resonance imaging (MRI) Ultrasonography Radionucleotide scanning
 Magnetic resonance imaging (MRI) Ultrasonography. Radionucleotide scanning.")
22
Fine Needle Aspiration Biopsy
Standard of diagnosis Indications Any neck mass that is not an obvious abscess Persistence after a 2 week course of antibiotics Small gauge needle Reduces bleeding Seeding of tumor – not a concern No contraindications (vascular ?)
")
23
Fine Needle Aspiration Biopsy

24
Computed Tomography Distinguish cystic from solid Extent of lesion
Vascularity (with contrast) Detection of unknown primary (metastatic) Pathologic node (lucent, >1.5cm, loss of shape) Avoid contrast in thyroid lesions
 Detection of unknown primary (metastatic) Pathologic node (lucent, >1.5cm, loss of shape) Avoid contrast in thyroid lesions.")
25
Magnetic Resonance Imaging
Similar information as CT Better for upper neck and skull base Vascular delineation with infusion

26
Ultrasonography Less important now with FNAB
Solid versus cystic masses Congenital cysts from solid nodes/tumors Noninvasive (pediatric)
")
27
Radionucleotide Scanning
Salivary and thyroid masses Location – glandular versus extra-glandular Functional information FNAB now preferred for for thyroid nodules Solitary nodules Multinodular goiter with new increasing nodule Hashimoto’s with new nodule

28
Primary Tumors Thyroid mass Lymphoma Salivary tumors Lipoma
Carotid body and glomus tumors Neurogenic tumors

29
Lymphoma More common in children and young adults
Up to 80% of children with Hodgkin’s have a neck mass Signs and symptoms Lateral neck mass only (discrete, rubbery, nontender) Fever Hepatosplenomegaly Diffuse adenopathy
 Fever. Hepatosplenomegaly. Diffuse adenopathy.")
30
Lymphoma FNAB – first line diagnostic test
If suggestive of lymphoma – open biopsy Full workup – CT scans of chest, abdomen, head and neck; bone marrow biopsy

31
Salivary Gland Tumors Enlarging mass anterior/inferior to ear or at the mandible angle is suspect Benign Asymptomatic except for mass Malignant Rapid growth, skin fixation, cranial nerve palsies

32
Salivary Gland Tumors

33
Carotid Body Tumor Rare in children Pulsatile, compressible mass
Mobile medial/lateral not superior/inferior Clinical diagnosis, confirmed by angiogram or CT No biopsy !!! Treatment Irradiation or close observation in the elderly Surgical resection for small tumors in young patients Hypotensive anesthesia Preoperative measurement of catecholamines

34
Carotid Body Tumor

35
Lipoma Soft, ill-defined mass Usually >35 years of age Asymptomatic
Clinical diagnosis – confirmed by excision

36
Lipoma

37
Congenital and Developmental Mass
Epidermal and sebaceous cysts Branchial cleft cysts Thyroglossal duct cyst Vascular tumors

38
Epidermal and Sebaceous Cysts

39
Branchial Cleft Cysts Most common as smooth, fluctuant mass underlying the SCM Skin erythema and tenderness if infected Treatment Initial control of infection Surgical excision, including tract May necessitate a total parotidectomy (1st cleft)
")
40
Branchial Cleft Cysts

41
Inflammatory Disorders
Lymphadenitis Granulomatous lymphadenitis

42
Our Patient squamous cell carcinoma metastatic to cervical lymph nodes from an unknown primary site

43
Incidence Author # pts % Jungehulsing 723 3.7 Lefebvre 8,500 2.2
Martin 3, Randall Richard 5, Jungehulsing, 2000 Lefebvre, 1990 Martin, 1944 Randall, 2000 Richard, 1977

44
Diagnosis 7 series (n=797) 5% 12% 60% 22% 11% 13% Bataini, 1987
Coker, 1977 Jesse, 1972 Marcial-Vega, 1990 Maulard, 1992 Wang, 1990

45
Metastasis Location according to Various Primary Lesions

46
Nodal Mass Workup in the Adult
Panendoscopy FNAB positive with no primary on repeat exam FNAB equivocal/negative in high risk patient Directed Biopsy All suspicious mucosal lesions Areas of concern on CT/MRI None observed – nasopharynx, tonsil (ipsilateral tonsillectomy for jugulodigastric nodes), base of tongue and piriforms Synchronous primaries (10 to 20%)
, base of tongue and piriforms. Synchronous primaries (10 to 20%)")
47
Nodal Mass Workup in the Adult
Open excisional biopsy Only if complete workup negative including FNA Occurs in ~5% of patients Be prepared for a complete neck dissection Frozen section results (complete node excision) Inflammatory or granulomatous – culture Lymphoma or adenocarcinoma – close wound
 Inflammatory or granulomatous – culture. Lymphoma or adenocarcinoma – close wound.")
48
Biopsy-proven primary
Diagnosis 130 suspected H&N unknown primaries Unknown Primary Biopsy-proven primary 43% Unknown Primary Tonsillectomy PET-guided biopsy 5% 3% Clinical ex. CT/(NMR) Mendenhall, 1998
 Mendenhall,")
49
TNM/AJCC 1997 Staging N0: no regional node metastasis
Nx: regional nodes cannot be assessed N1: single ipsilateral node, ≤ 3 cm N2a: single ipsilateral node, > 3 cm and ≤ 6 cm N2b: multiple ipsilateral nodes, ≤ 6 cm N2c: controlateral or bilateral nodes, ≤ 6 cm N3: node > 6 cm AJCC, 1997

50
Treatment: survival 5 year survival median (min-max)
All patients (23 series, n=2,167) 38% (15-65) N stage (n=932) N1 58% (19-90) N2a 41% (15-87) N2b 40% (15-63) N2c-N3 21% (0-62) Treatment Surgery (n=439) 66% (65-86) Surgery + RxTh (n=856) 50% (28-63) RxTh ± excision (n=553) 37% (16-74)
 38% (15-65) N stage (n=932) N1 58% (19-90) N2a 41% (15-87) N2b 40% (15-63) N2c-N3 21% (0-62) Treatment. Surgery (n=439) 66% (65-86) Surgery + RxTh (n=856) 50% (28-63) RxTh ± excision (n=553) 37% (16-74)")
51
Treatment: incidence of subsequent
H&N primary Incidence of mucosal primary (min-max) Surgery (n=232) 24% (13-48) Neck RxTh (n=544) 13% (5-41) Neck+mucosa RxTh (n=1,431) 11% (0-48)
 Surgery (n=232) 24% (13-48) Neck RxTh (n=544) 13% (5-41) Neck+mucosa RxTh (n=1,431) 11% (0-48)")
52
Treatment: incidence of subseqent
H&N primary 100 RT neck+mucosa (n=224) 87% 80 (n.s.) RT neck only (n=26) 76% 60 Probability (%) 46% 40 Surgery (n=23) 20 1 2 3 4 5 Years after treatment Grau 1999
 87% 80. (n.s.) RT neck only (n=26) 76% 60. Probability (%) 46% 40. Surgery (n=23) Years after treatment. Grau")
53
Follow-up : emerging of primary tumors
277 pts treated with curative intend median follow-up of 64 months 55 emerging primaries: oropharynx 25% lung 25% esophagus 9% oral cavity 7% larynx 7% hypopharynx 5% nasopharynx 4% other 18% Grau 1999

54
Treatment Cervical neck dissection Postoperative radiation

55
Treatment: disease-free survival
100 80 RT neck+mucosa (n=224) 60 Probability (%) 46% 40 n.s. 32% RT neck only (n=26) 20 1 2 3 4 5 Years after treatment Grau 1999
 60. Probability (%) 46% 40. n.s. 32% RT neck only (n=26) Years after treatment. Grau")
56
Adénopathie rétropéritonéale
Mr T, 62 ans Délégué commercial, gymnastique régulière AP: ancien tabagique, pancréatite alcoolique suite à laquelle il a fortement réduit sa consommation, rhinite allergique, hernie inguinale droite opérée, notion de prostatite AF: père néo pancréatique (éthylotabagique), mère néo rénal, oncle paternel néo cérébral, frère cirrhose éthylique
, mère néo rénal, oncle paternel néo cérébral, frère cirrhose éthylique.")
57
Anamnèse Pas de plaintes particulières
Dans le cadre d’un check-up, découverte fortuite à l’écho abdo d’une structure hypoéchogène de 4.5 cm sur 4 cm para-aortique, non compressive. Prostate un peu majorée de volume

58
Examen clinique Paramètres normaux ACP normale Abdomen: sp
Microadénopathies cervicales

59
Biologie Bio de base normale
Augmentation modérée des gammaGT et phosph. alc Pas de SI LDH nles, leuco<co> nl, profil électrophorétique nl, bêta2µgb nle, coombs nég Sérologies virales sp SU nl

60
Scanner abdominal sup Masse para-aortique de 84x56x35 mm caudal par rapport à la veine rénale gauche, proche de l’aorte, dont l’aspect évoque un lymphome. Ggl à proximité. Plusieurs adénopathies de taille infracm mésentériques.

61
PET Scan Zone intensément hypermétabolique en para-aortique. Aucune autre lésion d’hyperfixation.

62
prélèvement sous contrôle radiologique
Conclusion: masse para-aortique a priori isolée? prélèvement sous contrôle radiologique

63
prélèvement chirurgical souhaitable
Ponction tc: l’histologie conclut à une suspicion morphologique de lymphome B à grandes cellules de type immunoblastique (agressif). L’immunohistochimie ne permet pas de préciser la nature de cette prolifération prélèvement chirurgical souhaitable (par voie laparotomique de préférence car proximité des gros vx)
. L’immunohistochimie ne permet pas de préciser la nature de cette prolifération. prélèvement chirurgical souhaitable. (par voie laparotomique de préférence car proximité des gros vx)")
64
Laparotomie exploratrice avec exérèse d’une masse de 10 cm para-aortique gauche
histologie

65
Histologie Séminome pur

66
Palpation testiculaire: tumeur testiculaire gauche!!!

67
Echographie testiculaire
Formation charnue hétérogène dans la moitié inférieure du testicule gauche, vascularisée Dosage d’alphaFP nl et de bêtaHCG un peu majoré à 0.37 U/ml

68
Orchidectomie gauche: séminome testiculaire pur
pT1pN3 stade IIc radiothérapie

69
Plus de 2 ans plus tard: rémission complète

70
Take-home message Adénopathies rétro-péritonéales
Palper les testicules!!

71
Evaluation and Management of the Patient with Abdominal lymphadenopathy

72
General Considerations
Tuberculosis Abdominal abcess Cancer: Gynecologycal cancer Lymphoma, Sarcoma, Digestive cancer Testicule

73
Our patient: take home message
Toujours palper les testicules en particulier chez les hommes jeunes devant des adénopathies abdominales

74
Testicular cancer Seminomatous versus non-seminomatous tumor
Tumor markers: Beta-HCG, alpha-foetoprotein = non-seminomatous tumor Diagnostic and follow-up Non-seminomatous: Yolk-sac Embryonic carcinoma Choriocarcinoma Teratoma

75
Testicular cancer Stage 1: limited testicules
Stage 2: abdominal adenopathies Stage 3: metastases Prognostic: excellent even in the present of metastases

76
Testicular cancer: treatment
Surgery: primary tumor teratoma Chemotherapy: Seminoma and non-seminoma tumors: highly chemosensitive Teratoma: chemoresistant Radiation Seminoma: if abdominal mass less than 5 cm

77
Adénopathie axillaire
Mme M., 50 ans Août 2003: adénopathie axillaire gauche

78
Anamnèse Antécédents personnels: G1P1, épisodes de malaises lipothymiques Pas d’antécédents familiaux Remarque sous sa douche une adénopathie axillaire gauche dure et non douloureuse Anamnèse: sans particularités Vient avec le scan du MT

79
Examen clinique Sans particularités En particulier au niveau des seins

80
Examen clinique Quelle mise au point? Sans particularités
En particulier au niveau des seins Quelle mise au point?

82
Ponction du ganglion axillaire
adénocarcinome

83
Mammographie: négative

84
PET scan: adénopathie axillaire gauche, foyer mammaire gauche relativement profond, pas d’autre lésion secondaire Ponction du nodule suspect du QII gauche paramédian: tableau cytologique de carcinome canalaire de grade III.

85
Intervention: quadrantectomie et curage axillaire, ramenant un CCI grade III de 12x11x10 mm, sans perméation lymphatique. Recoupes indemnes d’infiltration néoplasique. 9 ganglions axillaires dont un volumineux, au niveau duquel on retrouve du tissu tumoral métastatique correspondant au carcinome Absence de récepteurs aux oestrogènes, petite quantité de récepteurs à la progestérone, absence de surexpression du Cerb B2.

86
6 cures de FEC adjuvante, radiothérapie puis hormonothérapie par Nolvadex
Septembre 2005: patiente toujours en rémission complète

87
Evaluation and Management of the Patient with An Axillary Mass

88
General Considerations
Drainage from Arm, Thoracic wall, Breast In the absence of upper extremity lesions, cancer is frequently found N=31 (de andrade, 1996) 9 breast cancer (5 controlateral) 8 metastases The rest benign masses (ectopic breast, infections, …)
 9 breast cancer (5 controlateral) 8 metastases. The rest benign masses (ectopic breast, infections, …)")
89
Our Patient FNA Breast cancer: surgery, chemotherapy, radiotherapy

90
Axillary breast metastases with unknown primary
Prognostic similar than other breast cancer Mastectomy and axillar dissection and systemic treatment Axillary dissection, whole breast irradiation and systemic treatment can avoid mastectomy

91
Adénopathie sus-claviculaire
Mr K., 39 ans, ophtalmologue Sa femme remarque chez lui une masse sus-claviculaire gauche fixée, ferme, indolore Pas d’antécédents familiaux, pas d’antécédents personnels, pas de consommation éthylotabagique

92
Anamnèse Asthénie attribuée aux activités professionnelles importantes, perte de poids de 6 kgs en quelques mois, sudations nocturnes depuis 2 mois Prurit (ancien) Gastro et examen ORL il y a deux mois pour ingestion d’arête: sp Notion de syndrome inflammatoire détecté sur biologie il y a 2 mois (CRP à 2 et vs accélérée)
 Gastro et examen ORL il y a deux mois pour ingestion d’arête: sp. Notion de syndrome inflammatoire détecté sur biologie il y a 2 mois (CRP à 2 et vs accélérée)")
93
Anamnèse (suite) Notion de séjour prolongé en Afrique du Sud il ya 2 ans avec contact avec patients tbc mais a eu vaccin BCG et suivi régulier par RXTX

94
Examen clinique Paramètres normaux ACP normale
Abdomen: petite hernie ombilicale Masse sus-claviculaire gauche polycyclique, non inflammatoire, non douloureuse, ferme, fixée et mesurant environ 4x4 cm

95
Biologie SI modéré Hémogramme normal, leuco<co> nl
LDH normales, bêta2µgb nle GammaGT discrètement majorés (1.5xN) Séros IgM EBV, toxo, CMV, hép B et C, HIV négatives Status post-vaccinal pour l’hép B Séro Bartonella henselae négative Hypergammagb modérée, profil protéique nl
 Séros IgM EBV, toxo, CMV, hép B et C, HIV négatives. Status post-vaccinal pour l’hép B. Séro Bartonella henselae négative. Hypergammagb modérée, profil protéique nl.")
96
Quelle mise au point?

97
Echographie cervicale
Large formation ovalaire de 59x23x27 mm au dessus de l’origine des vx sous-clav gauches. Contenu partiellement hypoéchogène d’aspect nécrotique. 5 petites formations ggl plus petites sont notées au dessus de cette masse.

98
Echographie abdominale
Pas d’organomégalie ou d’adénomégalie

100
Scanner thoraco-abdominal
Adénopathie médiastinale péricentimétrique et masse sus-claviculaire gauche partiellement nécrotique

101
En conclusion: Biopsie ggl prévue sous AG+ PBMO
masse sus-claviculaire gauche ganglionnaire accompagnée d’une AEG avec symptômes B et d’un syndrome inflammatoire Biopsie ggl prévue sous AG+ PBMO

102
Résultats A l’analyse: la section révèle un aspect purulent
Cytologie et histologie du prélèvement ganglionnaire: image d’adénite granulomateuse (évoquant en 1ière hypothèse une mycobactérie) Immunophénotypage du ggl: cell. mortes
 Immunophénotypage du ggl: cell. mortes.")
103
Résultats (suite) Bactériologie: stérile, présence de staph coag nég dans ½ milieu d’enrichissement, Ziehl négatif, Auramine négatif
 Bactériologie: stérile, présence de staph coag nég dans ½ milieu d’enrichissement, Ziehl négatif, Auramine négatif.")
104
Résultats (suite) Ponction de MO: moëlle réactionnelle
Biopsie de MO: non contributive Immunophénotypage de la MO: sp hormis une inversion du rapport CD4/CD8

105
Résultats (suite) Culture BK: 11 jours après la mise en culture, développement de bacilles acido-alcoolorésistants de type Mycobacterium tuberculosis (sonde Accuprobe)
")
106
Evaluation and Management of the Patient with A Supraclavicular Mass

107
General Considerations
High risk of Malignancy : 34 to 50 % (particularly > 40y) Right supraclavicular: Mediastinum, lungs, esophagus Left supraclavicular Abdominal: stomach, pancreas, kidneys, testicules, Ovaries, prostate
 Right supraclavicular: Mediastinum, lungs, esophagus. Left supraclavicular. Abdominal: stomach, pancreas, kidneys, testicules, Ovaries, prostate.")
108
Evaluation and Management of the Patient with An Inguinal Mass

109
General Considerations
Lower extremity infection Sexually transmitted disease Cancer (descending order): Skin of the lower extremities, cervix, vulva, skin of the trunk, rectum, anus, penis
: Skin of the lower extremities, cervix, vulva, skin of the trunk, rectum, anus, penis.")
Présentations similaires