Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Avancées de la recherche vaccinale anti-VIH
Pr Yves Lévy Service d’Immunologie Clinique CHU Henri Mondor/AP-HP/UPEC INSERM U955 I would like to thank the organizers for this invitation. What I would like to do today is to discuss the rationale for the development of these approaches and to show you some new data. I will try also to discuss nen strategies aimed at targeting the viral reservoir. Controlling HIV infection continues to be a major challenge in both underdeveloped and developed countries. However, to find new ways to improve the reconsitution of the immune system beyonf becomes a new challenge. Given the increasing knowledge of mechanisms that allow control of HIV infection, several groups are focusing their efforts on the development of new appraoches.

2
Etat des lieux de l’avancée de l’épidémie
Environ 7000 nouvelles infections par jour

3
HISTORIQUE La recherche vaccinale: un processus lent
Vaccins Nombre d’années Typhoid 105 Pertussis 89 Polio 47 Rougeole 42 Hepatitis B 16 H. Influenza 92 HIV > 27 ans From H.Markel, NEJM, 2005

4
Recherche d’un vaccin anti-VIH: Historique
1987:1er essai de phase I : > 85 essais phase I/II avec > 30 candidats (>30 essais en cours) Pas d’effets secondaires, non toxique, un certain degré d’immunogenicité. 2003: Résultat du 1er essai phase III : Echec du 2é essai d’efficacité 2009: premier espoir The dynamic of HIV/AIDS vaccine research could be considered as successive dreams and nightmares, summarized on this slide on the history of the vaccine trials in humans with failure and very limited success up to now. This history started in 1987 with the first Phase 1 trial. Since then, more than 85 Phase I/II trials have been conducted with more than 30 candidates and more than 30 trials are still ongoing. They have shown that the candidates are safe and are at least partially immunogenic. In 2003, data of the 1st Phase II efficacy trial were reported, definitively proving that the recombinant gp120 used as a candidate in this trial was not protecting against the infection and was not even reducing viral replication. Since the AIDS conference in Bangkok two years ago, additional trials have been launched. Two efficacy trial are ongoing with data expected by and new ones will probably be conducted according to some encouraging data from Phase I/Iia trials. In addition, new vaccine candidates have been designed. Indeed, if we analyze the vaccine strategies that have been used up to now, there are (NEXT SLIDE)…
 Pas d’effets secondaires, non toxique, un certain degré d’immunogenicité. 2003: Résultat du 1er essai phase III : Echec du 2é essai d’efficacité. 2009: premier espoir. The dynamic of HIV/AIDS vaccine research could be considered as successive dreams and nightmares, summarized on this slide on the history of the vaccine trials in humans with failure and very limited success up to now. This history started in 1987 with the first Phase 1 trial. Since then, more than 85 Phase I/II trials have been conducted with more than 30 candidates and more than 30 trials are still ongoing. They have shown that the candidates are safe and are at least partially immunogenic. In 2003, data of the 1st Phase II efficacy trial were reported, definitively proving that the recombinant gp120 used as a candidate in this trial was not protecting against the infection and was not even reducing viral replication. Since the AIDS conference in Bangkok two years ago, additional trials have been launched. Two efficacy trial are ongoing with data expected by and new ones will probably be conducted according to some encouraging data from Phase I/Iia trials. In addition, new vaccine candidates have been designed. Indeed, if we analyze the vaccine strategies that have been used up to now, there are (NEXT SLIDE)…")
5
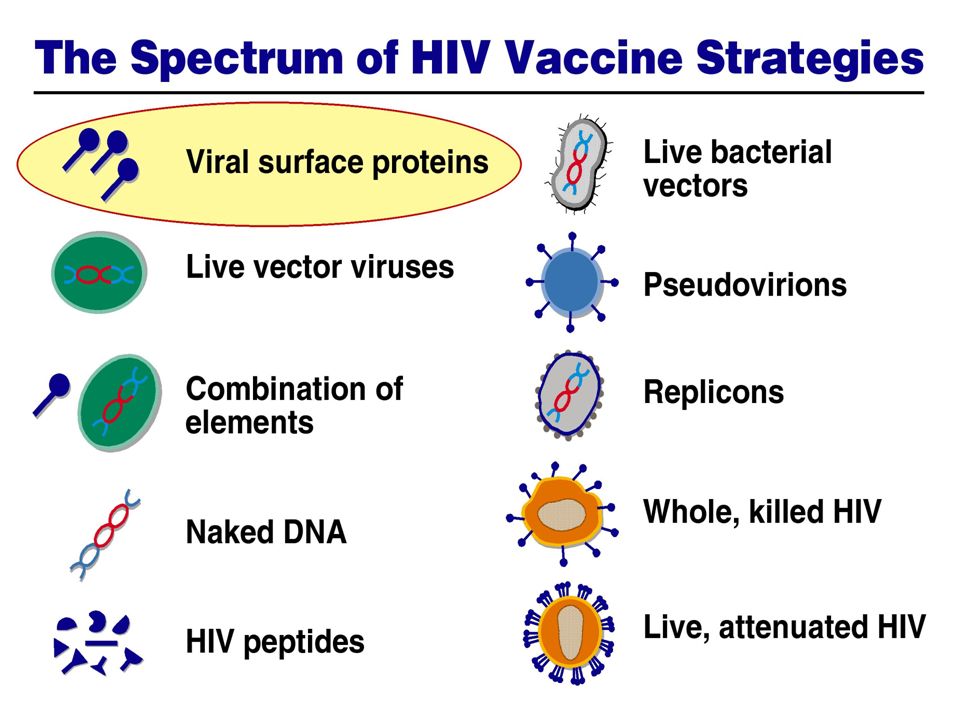
Stratégies vaccinales traditionnelles.
Des obstacles scientifiques non résolus.… Pourquoi? (The design of vaccine candidates has been)….. mostly empirical without enough scientific rationale. Why? Simply because to develop novel and rational strategies, we need to improve our knowledge on how vaccines work…
….. mostly empirical without enough scientific rationale. Why Simply because to develop novel and rational strategies, we need to improve our knowledge on how vaccines work…")
6
Obstacles Scientifiques (2)
Méconnaissances des mécanismes (ou, au moins des corrélats) de protection; Peu de concepts immunologiques nouveaux et applicables; Connaissance insuffisantes des mécanismes précoces impliqués dans l’initiation de notre défense immunitaire; Des obstacles spécifiques à l’infection VIH…. The second one is the lack of novel and applicable new concepts derived from fundamental immunology. The third one, which is indeed related to the second one, is our insufficient knowledge of the very complex cross-talk between components of the innate and adaptive immunity. This is a critical issue. However, this field is really moving fast and I am convinced that HIV/AIDS research will strongly benefit of the most recent and continuing progress in immunology. The fourth scientific gap is represented by key scientific challenges in HIV/AIDS that are presented on THE NEXT TWO SLIDES.
 de protection; Peu de concepts immunologiques nouveaux et applicables; Connaissance insuffisantes des mécanismes précoces impliqués dans l’initiation de notre défense immunitaire; Des obstacles spécifiques à l’infection VIH…. The second one is the lack of novel and applicable new concepts derived from fundamental immunology. The third one, which is indeed related to the second one, is our insufficient knowledge of the very complex cross-talk between components of the innate and adaptive immunity. This is a critical issue. However, this field is really moving fast and I am convinced that HIV/AIDS research will strongly benefit of the most recent and continuing progress in immunology. The fourth scientific gap is represented by key scientific challenges in HIV/AIDS that are presented on THE NEXT TWO SLIDES.")
7
Uninfected primary CD4+ lymphocyte

8
HIV-infected primary CD4+ lymphocyte

9
HIV-infected primary CD4+ lymphocyte

10
Simultaneous HIV cell-to-cell transfer through “polysynapses”
Jurkat Jurkat HIV Gag actin target cell

11
Diverse modes of HIV cell-to-cell transfer
Virological synapse Multiple contacts HIV Gag Actin Target cell HIV, protrusions, pseudopodia HIV along filopodia and nanotubes D. Rudnicka & N. Sol-Foulon

12
HIV Gag actin target cell

13
Rôle des réponses immunitaires au cours d’une vaccination anti virale
Anticorps vaccinaux PREVENTION DE L’INFECTION DE LA MAJORITE DES CELLULES QUELQUES CELLULES SONT INFECTÉES PUIS DETRUITES PAR LES LYMPHOCYTES T CD8+ Lymphocytes T CD8+ Induits par vaccins Beaucoup d’empirisme dans la réalisation des vaccins Seuls le dosage des anticorps est pris en compte pour apprécier efficacité vaccination

15
Echecs essais phase III
AIDSVAX 2003 Candidats vaccins Protéines gp 120 recombinantes Pays concernés Canada, Etats-Unis, Pays-Bas, Porto Rico Thaïlande Populations Sujets avec risque sexuel (Etats-Unis) 500 Toxicomanes (Thaïlande) 2500 15
 500. Toxicomanes (Thaïlande)")
16
Charge virale chez les patients infectés par le VIH durant l’essai
Candidats vaccins Adénovirus avec protéines gag, pol et nef Pays concernés Australie, Brésil, Canada, Etats-Unis, Haïti , Jamaïque, Pérou, Porto-Rico, République Dominicaine Populations Sujets à risque sexuel 3000 STEP 2007 Infections par le VIH Charge virale chez les patients infectés par le VIH durant l’essai

17
Essai Thaï Vaccine infections: 51 Placebo infections: 74 p = 0.039
Description de l’essai RV144: Essai de Phase III Trial associant Priming avec ALVAC-HIV (vCP1521 -Aventis Pasteur) Boost avec VaxGen gp120 B/E (AIDSVAX® B/E) Objectifs primaires Protection contre acquisition infection Etude désignée avec taux de protection attendu de 50% Diminution niveau charge virale Etude désignée pour détecter une diminution de 0.4 Log10 de la charge virale en cas de non protection Sponsors Surgeon General, US Army; IND is held by USAMMDA; USMHRP and USAMC-AFRIMS execute for Sponsor Candidats-Vaccins Prime: ALVAC-HIV 0, 1, 3, 6 mo (subtype B gag/pro; subtype E env) Boost: AIDSVAX B/E gp120 3, 6 mo (subtype B and E env) Phase clinique volontaires Phase IIb (Test of Concept, TOC) Trial Fin des enrôlements Decembre 2005 Dernière injection - Juillet 2006 Premières analyses - Septembre2009 Co-Development Partners Ministry of Public Health (MOPH), Thailand Mahidol University (VTC & DMU) Royal Thai Army National Institute of Allergy & Infectious Diseases (NIAID) Global Solutions in Infectious Diseases (VaxGen) sanofi pasteur Vaccine infections: 51 Placebo infections: 74 p = 0.039 Efficacy 31.2% Efficacy 95% CI: (1.7, 51.8) Efficacy OBF 95% CI: (1.1, 52.1)
 Boost avec VaxGen gp120 B/E (AIDSVAX® B/E) Objectifs primaires. Protection contre acquisition infection. Etude désignée avec taux de protection attendu de 50% Diminution niveau charge virale. Etude désignée pour détecter une diminution de 0.4 Log10 de la charge virale en cas de non protection. Sponsors. Surgeon General, US Army; IND is held by USAMMDA; USMHRP and USAMC-AFRIMS execute for Sponsor. Candidats-Vaccins. Prime: ALVAC-HIV 0, 1, 3, 6 mo (subtype B gag/pro; subtype E env) Boost: AIDSVAX B/E gp120 3, 6 mo (subtype B and E env) Phase clinique volontaires. Phase IIb (Test of Concept, TOC) Trial. Fin des enrôlements Decembre Dernière injection - Juillet Premières analyses - Septembre2009. Co-Development Partners. Ministry of Public Health (MOPH), Thailand. Mahidol University (VTC & DMU) Royal Thai Army. National Institute of Allergy & Infectious. Diseases (NIAID) Global Solutions in Infectious Diseases (VaxGen) sanofi pasteur. Vaccine infections: 51. Placebo infections: 74. p = Efficacy 31.2% Efficacy 95% CI: (1.7, 51.8) Efficacy OBF 95% CI: (1.1, 52.1)")
18
Diversifier les vecteurs vaccinaux
O HN HOOC H NH K Palmitoyl HIV peptide NYVAC (B/C) MVA (B) ADN LIPO5 Peptide-anti-DC Ad5
 MVA (B) ADN. LIPO5. Peptide-anti-DC. Ad5.")
20
DC + T lymphocyte

21
(Anti-DC Gag/Pol/Nef)
Programme vaccinal de l’ANRS 2007 2008 2009 2010 2011 2012 Nov. 2006 Juin 2007 Nov. 2007 VAC 18 (HIV LIPO-5) Recrutement (fin) vaccination (fin) VAC 20 (DNA/NYVAC) Collaboration Européenne EUROVACC VAC 21 (Phase 1) (DNA + LIPO-5) VAC 22 (Phase 2) (MVA + LIPO-5) Collaboration Internationale Baylor Institute INSERM VAC 23 (Anti-DC Gag/Nef) VAC 24 (Anti-DC Gag/Pol/Nef) COHVAC
 Recrutement (fin) vaccination (fin) VAC 20. (DNA/NYVAC) Collaboration. Européenne. EUROVACC. VAC 21 (Phase 1) (DNA + LIPO-5) VAC 22 (Phase 2) (MVA + LIPO-5) Collaboration. Internationale. Baylor Institute. INSERM. VAC 23. (Anti-DC Gag/Nef) VAC 24. (Anti-DC Gag/Pol/Nef) COHVAC.")
22
Poursuivre les essais de phases I/II chez l’Homme
Le réseau des volontaires de l’ANRS Faire "acte de candidature" auprès de l'ANRS Etre âgé de 21 à 54 ans Passer un examen médical et psychologique permet de déterminer qu’on est * séronégatif(ve) pour le VIH * en bonne santé * motivé(e) pour participer à un essai qui nécessite plusieurs mois de suivi * est à faible risque de contamination par le VIH La sélection des candidats s'effectue en tenant compte de deux critères principaux : * Un critère comportemental.. * Un critère psychologique et social. Marseille (I. Poizot-Martin) MP. Drogoul, F. Vion-Dury ,C .Farnarier Nantes (B. Bonnet) P. Morineau ,M. Audrain Paris Cochin (O. Launay) C .Desaint, Y. Henin Paris Mondor (JD. Lelièvre) C. Dumont, A Kontaratou Paris Tenon (G. Pialoux) L.Slama, C. Fontaine Toulouse (L. Cuzin) F. Balsarin, F. Nicot, J. Izopet
 pour le VIH. * en bonne santé. * motivé(e) pour participer à un essai qui nécessite plusieurs mois de suivi. * est à faible risque de contamination par le VIH. La sélection des candidats s effectue en tenant compte de deux critères principaux : * Un critère comportemental.. * Un critère psychologique et social. Marseille (I. Poizot-Martin) MP. Drogoul, F. Vion-Dury ,C .Farnarier Nantes (B. Bonnet) P. Morineau ,M. Audrain. Paris Cochin (O. Launay) C .Desaint, Y. Henin. Paris Mondor (JD. Lelièvre) C. Dumont, A Kontaratou. Paris Tenon (G. Pialoux) L.Slama, C. Fontaine. Toulouse (L. Cuzin) F. Balsarin, F. Nicot, J. Izopet.")
23
CONCLUSIONS La recherche vaccinale anti-VIH est le domaine où on peut espérer des progrès vertigineux au cours de ce 21ème siècle… SI.. I WOULD LIKE TO CONCLUDE BY SAYING THAT …. BUT, WE SHOULD KEEP IN MIND THAT…NEXT SLIDE Elle repose sur des données scientifiques solides de recherche fondamentale qui est et restera le ciment des progrès en recherches appliquées…

24
Trois autres éléments fondamentaux au succès de toute recherche…
Transparence Coopération Collaboration Au niveau international:

25
La recherche, une étape incontournable aux progès médicaux
Traitement Prévention Soins Recherche fondamentale et Clinique

26
Immunogénicité - Corrélats de protection
Lors du développement d’un vaccin on cherche à mettre en évidence son immunogénicité Plusieurs questions se posent: Quel est le marqueur immunologique permettant de prédire la protection? Quels sont les moyens dont on dispose permettant de mettre en évidence l’immunogénicité ? A t’on induit l’immunogénicité voulue avec le candidat vaccin?

Présentations similaires



v Programme de recherches Institut de Microbiologie et Maladies Infectieuses.>")
>")















