Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Comprendre la prévention des accidents vasculaires cérébraux liés à la fibrillation auriculaire
Michel D’Astous Cardiologue Centre hospitalier universitaire Dr Georges-L Dumont University Hospital Center

5
La fibrillation auriculaire
La fibrillation auriculaire (FA) est le trouble du rythme cardiaque le plus répandu On estime que 1 personne sur 4 âgée de 40 ans sera atteinte de fibrillation auriculaire Atrial fibrillation (AF) is the most common heart rhythm disturbance. The lifetime risk of developing Atrial fibrillation in individuals aged 40 is 25%. Reference Lloyd-Jones DM, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study.Circulation 2004;110: Atrial fibrillation image Avalable at fibrillation.html. Accessed January 18, Voies électriques normales Nœud sino-auriculaire (SA) Nœud atrioventriculaire (AV) Rythme sinusal normal Voies électriques anormales Fibrillation auriculaire Rythme normal FA FA = fibrillation auriculaire Lloyd-Jones, DM. et autres. Circulation, 110: , 2004
 est le trouble du rythme cardiaque le plus répandu. On estime que 1 personne sur 4 âgée de 40 ans sera atteinte de fibrillation auriculaire. Atrial fibrillation (AF) is the most common heart rhythm disturbance. The lifetime risk of developing Atrial fibrillation in individuals aged 40 is 25%. Reference. Lloyd-Jones DM, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study.Circulation 2004;110: Atrial fibrillation image Avalable at fibrillation.html. Accessed January 18, Voies électriques normales. Nœud sino-auriculaire (SA) Nœud atrioventriculaire (AV) Rythme sinusal normal. Voies électriques anormales. Fibrillation auriculaire. Rythme normal. FA. FA = fibrillation auriculaire. Lloyd-Jones, DM. et autres. Circulation, 110: ,")
6
ECG révélant la fibrillation auriculaire
This shows the main findings of ECG in atrial fibrillation: absence of P waves, irregularly irregular R-R intervals, and irregular fluctuations in baseline (notably in leads III and VI). Reference Conclusions principales : Absence d’ondes P Intervalles R-R irrégulièrement irréguliers Fluctuations irrégulières dans la ligne de base (plus remarquables dans les dérivations III et VI)
. Reference. Conclusions principales : Absence d’ondes P. Intervalles R-R irrégulièrement irréguliers. Fluctuations irrégulières dans la ligne de base (plus remarquables dans les dérivations III et VI)")
7
Classement de la fibrillation auriculaire
Terminologie Caractéristiques cliniques Parcours Premier événement (premier épisode détecté) Apparition symptomatique ou asymptomatique inconnue Réapparition ou non Paroxystique Arrêt spontané <7 jours et plus souvent <48 heures Récurrence Persistante Absence d’arrêt spontané : Durée de >7 jours ou cardioversion antérieure Permanente (« acceptée ») Absence d’arrêt, arrêt et rechute et aucune tentative de cardioversion Établissement Atrial fibrillation (AF) is considered recurrent when a patient develops two or more episodes. These episodes may be paroxysmal if they terminate spontaneously, defined by consensus as terminating within seven days, or persistent if the arrhythmia requires electrical or pharmacological cardioversion for termination. Successful termination of AF does not alter the classification of persistent AF in these patients. Longstanding AF (defined as over 1 year) not successfully terminated by cardioversion, or when cardioversion is not pursued, is classified as permanent. Without treatment, AF can result in some degree of disruption to the circulation of blood around the body. In some cases of AF, the degree of haemodynamic instability can represent a critical condition that requires immediate intervention. Reference Fuster v, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation--executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation). J Am Coll Cardiol 2006;48: Fuste, V. et autres. ACC/AHA/ESC 2006 guidelines, Journal of American College Cardiology, 48: , 2006.
 Apparition symptomatique ou asymptomatique inconnue. Réapparition ou non. Paroxystique. Arrêt spontané <7 jours et plus souvent <48 heures. Récurrence. Persistante. Absence d’arrêt spontané : Durée de >7 jours ou cardioversion antérieure. Permanente. (« acceptée ») Absence d’arrêt, arrêt et rechute et aucune tentative de cardioversion. Établissement. Atrial fibrillation (AF) is considered recurrent when a patient develops two or more episodes. These episodes may be paroxysmal if they terminate spontaneously, defined by consensus as terminating within seven days, or persistent if the arrhythmia requires electrical or pharmacological cardioversion for termination. Successful termination of AF does not alter the classification of persistent AF in these patients. Longstanding AF (defined as over 1 year) not successfully terminated by cardioversion, or when cardioversion is not pursued, is classified as permanent. Without treatment, AF can result in some degree of disruption to the circulation of blood around the body. In some cases of AF, the degree of haemodynamic instability can represent a critical condition that requires immediate intervention. Reference. Fuster v, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation--executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation). J Am Coll Cardiol 2006;48: Fuste, V. et autres. ACC/AHA/ESC 2006 guidelines, Journal of American College Cardiology, 48: ,")
8
La FA est une maladie évolutive
Durée de la FA Paroxystique Dépendante des déclenchers (Initiation) Reference Khan I.A. Int J Card 2003;87: Permanente Dépendante du substrat (Maintien) Importance relative Persistante 8 8 8 8 Khan, I.A. International Journal of Cardiology, 87: , 2003 8
 Reference. Khan I.A. Int J Card 2003;87: Permanente. Dépendante du substrat. (Maintien) Importance relative. Persistante Khan, I.A. International Journal of Cardiology, 87: ,")
9
Avant / Après Enlevez la saleté de vos chemises

10
Traitement de la FA 1 : Trouver une cause
2 : Contrôle de la fréquence cardiaque 3 : Contrôle du rythme vs la fréquence 4 : ASA vs anticoagulation

11
Traitement de la FA 1 : Trouver une cause
2 : Contrôle de la fréquence cardiaque 3 : Contrôle du rythme vs la fréquence 4 : ASA vs anticoagulation

12
Étiologie de la FA Nombreuses causes : Tenez compte de ce qui suit :
Hypertension Coronaropathies Cardiopathies valvulaires Myocardiopathies Traumatismes et infections pulmonaires ou cardiaques Hyperthyroïdie R/o FA isolée

13
Mon médecin a dit « Juste un verre d’alcool par jour
Mon médecin a dit « Juste un verre d’alcool par jour. » Je peux vivre avec ça.

14
Investigation de la FA Formule sanguine (FS), analyse rénale et vérification de la fonction hépatique ECG (hypertrophie ventriculaire gauche (HVG), ondes Q et intervalles QT) Ne pas omettre : La TSH L’échocardiogramme Dans certains cas : L’épreuve d’effort, la surveillance Holter, la radiographie pulmonaire et l’échocardiographie transoesophagienne (ETE)
, ondes Q et intervalles QT) Ne pas omettre : La TSH. L’échocardiogramme. Dans certains cas : L’épreuve d’effort, la surveillance Holter, la radiographie pulmonaire et l’échocardiographie transoesophagienne (ETE)")
15
Traitement de la FA 1 : Trouver une cause
2 : Contrôle de la fréquence cardiaque 3 : Contrôle du rythme vs la fréquence 4 : ASA vs anticoagulation

17
Je me méfie de ces stimulateurs cardiaques à piles.

18
Traitement de la FA 1 : Trouver une cause
2 : Contrôle de la fréquence cardiaque 3 : Contrôle du rythme vs la fréquence 4 : ASA vs anticoagulation

19
Prévention des AVC liés à la fibrillation auriculaire
- Mortalité chez les patients sous contrôle de la fréquence vs le rythme - L’étude AFFIRM Mortalité toute cause 30 25 Contrôle du rythme 20 Mortalité cumulative (%) Contrôle de la fréquence P=0,08 15 10 5 1 2 3 4 5 Années suivant la randomisation Randomisation des patients atteints de FA et à risque élevé d’AVC pour cardioversion et traitement à l’aide d’antiarythmisants afin de maintenir le rythme sinusal ou recours à des médicaments de contrôle de la fréquence L’utilisation d’anticoagulants a été recommandée mais non mandatée New England Journal of Medicine, 347: , 2002.
 Contrôle de la fréquence. P=0, Années suivant la randomisation. Randomisation des patients atteints de FA et à risque élevé d’AVC pour cardioversion et traitement à l’aide d’antiarythmisants afin de maintenir le rythme sinusal ou recours à des médicaments de contrôle de la fréquence. L’utilisation d’anticoagulants a été recommandée mais non mandatée. New England Journal of Medicine, 347: ,")
20
Prévention des AVC liés à la fibrillation auriculaire
- Mortalité chez les patients sous contrôle de la fréquence vs le rythme - L’étude AFFIRM Valeur de p <0,0001 0,0005 Rythme sinusal Utilisation d’antiarhythmisants Utilisation de la warfarine Utilisation de la digoxine A recent meta-analysis, which combined the results from the FASTER, CHARISMA, CARESS and MATCH studies add weight to the hypothesis that early treatment of patients with acute TIA or minor stroke with combination therapy will reduce the incidence of major adverse events. Again, these results would be considered hypothesis generating and need to be confirmed in a in a larger study. 0,5 1,0 1,5 2,0 Risque relatif New England Journal of Medicine, 347: , 2002.

21
Traitement de la FA 1 : Trouver une cause
2 : Contrôle de la fréquence cardiaque 3 : Contrôle du rythme vs la fréquence 4 : ASA vs anticoagulation

22
La fibrillation auriculaire - Un facteur de risque d’AVC majeur
Facteur de risque d’AVC indépendant – multiplie le risque d’AVC par 51,2,3 Responsable de près de 15 – 20 % de tous les AVC à l’échelle nationale1,4 Le risque d’AVC chez les patients atteints de FA croît avec l’âge 1,5 % chez les 50 – 59 ans 23,5 % chez les 80 – 89 ans Le risque d’AVC est le même chez les patients atteints de FA paroxystique ou soutenue Atrial fibrillation is a major risk factor for stroke. It increases the risk of stroke by 5-fold and accounts for approximately 15-20% of all strokes nationally. It is associated with a 50-90% increase in mortality risk after adjustment for coexisting cardiovascular conditions. The risk of stroke in AF patients who do not receive anticoagulation averages ~5% per year. The risk of stroke in AF patients increases with age: 1.5% in 50–59 year olds 23.5% in 80–89 year olds References 1. Atrial Fibrillation Investigation Group. Arch Intern Med 2. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22(8):983-8. 3. Savelieva I, Bajpai A, Camm AJ . Stroke in atrial fibrillation: update on pathophysiology, new antithrombotic therapies, and evolution of procedures and devices. Ann Med 2007;39(5): 4. Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ; American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133(6 Suppl):546S- 592S. 1. Atrial Fibrillation Investigation Group. Archives of Internal Medicine, 1994 2. Wolf, PA. et autres. Stroke, 1991 3. Savelieva, I. et autres. Annals of Medicine, 2007 4. Singer, DE. et autres. Chest, 2008 FA = fibrillation auriculaire
: Savelieva I, Bajpai A, Camm AJ . Stroke in atrial fibrillation: update on pathophysiology, new antithrombotic therapies, and evolution of procedures and devices. Ann Med 2007;39(5): Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ; American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133(6 Suppl):546S- 592S. 1. Atrial Fibrillation Investigation Group. Archives of Internal Medicine, Wolf, PA. et autres. Stroke, Savelieva, I. et autres. Annals of Medicine, Singer, DE. et autres. Chest, FA = fibrillation auriculaire.")
23
Les AVC ne dépendent pas du type de FA
Reference Neuwfaat R, et al. Eur Heart J 2008. % de patients atteints d’accidents ischémiques cérébraux (AIC) après 1 an Première détection / Paroxystique / Persistante / Permanente Neuwfaat, R. et autres. European Heart Journal, 2008.
 après 1 an. Première détection / Paroxystique / Persistante / Permanente. Neuwfaat, R. et autres. European Heart Journal,")
24
Gravité des AVC chez les patients atteints de FA
Effet du premier AIC chez les patients atteints de FA (n = 597) 60 % 40 % 0 % 50 % 30 % 20 % 10 % In a recent study by Gladstone and colleagues of nearly 600 patients who were admitted to the hospital with a first ischemic stroke from AF, 60% were disabling and 20% were fatal.1 Note that the rate if disability for these strokes is considerably higher than for stroke overall reported by Thom et al where 22% of men and 25% of women who have an initial stroke die within a year. This percentage is higher among people aged 65 and older, and 51% of men and 53% of women under the age of 65 who have a stroke die within 8 years. The length of time to recover from a stroke depends on its severity where 50–70% of stroke survivors regain functional independence, but 15–30% are permanently disabled, and 20% require institutional care at 3 months after onset.2 References Gladstone DJ, et al. Potentially preventable strokes in high-risk patients with atrial fibrillation who are not adequately anticoagulated. Stroke 2009; 40: Thom T, et al. Heart disease and stroke statistics update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee.Circulation 2006; 113: e85–e151. % de patients Invalidant Mortel FA = fibrillation auriculaire Gladstone, DJ. et autres. Stroke, 40: , 2009.
 60 % 40 % 0 % 50 % 30 % 20 % 10 % In a recent study by Gladstone and colleagues of nearly 600 patients who were admitted to the hospital with a first ischemic stroke from AF, 60% were disabling and 20% were fatal.1. Note that the rate if disability for these strokes is considerably higher than for stroke overall reported by Thom et al where 22% of men and 25% of women who have an initial stroke die within a year. This percentage is higher among people aged 65 and older, and 51% of men and 53% of women under the age of 65 who have a stroke die within 8 years. The length of time to recover from a stroke depends on its severity where 50–70% of stroke survivors regain functional independence, but 15–30% are permanently disabled, and 20% require institutional care at 3 months after onset.2. References. Gladstone DJ, et al. Potentially preventable strokes in high-risk patients with atrial fibrillation who are not adequately anticoagulated. Stroke 2009; 40: Thom T, et al. Heart disease and stroke statistics update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee.Circulation 2006; 113: e85–e151. % de patients. Invalidant. Mortel. FA = fibrillation auriculaire. Gladstone, DJ. et autres. Stroke, 40: ,")
25
Incidence de la FA ajustée selon l’âge et le sexe de 1995 à 2000
L’on s’attend à ce que l’incidence de la FA augmente avec le vieillissement de la population Incidence de la FA ajustée selon l’âge et le sexe de 1995 à 2000 Extrapolation du nombre de personnes atteintes de FA aux États-Unis de 2000 à 2050 Atrial fibrillation is more common in men than in women at all ages and increases significantly with age. Demographic projections suggest a tripling of the frequency over the next 40 years. The age- and sex-adjusted incidence of AF in 1995 to 2000, in Olmstead County, Minnesota, US, is shown in the graph on the left. Age was clearly an important risk factor for AF, with virtually no cases among individuals aged <55 years. The incidence per 1000 patient years increased to over 40 and almost 29 among men and women, respectively, aged ≥85 years. The graph on the right shows the projected number of persons with AF in the US between 2000 and Miyasaka and colleagues project that, by year 2050, nearly 15.9 million people will have AF, assuming a continued increase in incidence rate similar to that in All of these patients are at increased risk for stroke. Reference Miyasaka Y, Barnes ME, Gersh BJ et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114: Millions Années Taux d’incidence par patients-années / Hommes / Femmes / Groupe d’âge (années) / Millions / Année FA = fibrillation auriculaire Miyasaka, Y. et autres. Circulation, 114: , 2006.
 / Millions / Année. FA = fibrillation auriculaire. Miyasaka, Y. et autres. Circulation, 114: ,")
26
Le diabète et la FA Incidence d’un nouvel incident de FA
La prévalence de la FA est supérieure de 44 % dans le cas du DS La FA a 38 % plus de chances de se développer dans le cas du DS Le DS est un prédicteur indépendant hautement significatif de la FA chez les femmes Reference Diabetes Care 2009;32: Incidence cumulative de la FA en % Années de suivi FA = fibrillation auriculaire DS = diabète sucré Diabetes Care, 32: , 2009.

27
Rôle de la tension artérielle dans le risque d’AVC/embolie systémique chez les patients atteints de FA 100 110 120 130 140 150 160 TAS Taux d’événements (%/an) 0,5 1,0 1,5 2,0 2,5 3,0 3,5 4,0 TAS MOYENNE (en mmHg) Hypertension contributes to increased stroke and systemic embolus in AF. This graph emanates from a cross-sectional, longitudinal analysis of data from the SPORTIF III and V trials. It showed an increasing rate of stroke and SEE with increasing quartiles of systolic blood pressure. In the combined SPORTIF III and V cohort, the event rate for stroke/SEE increased markedly at mean SBP above 140 mmHg, as shown by the blue arrow. When the top quartile of SBP was compared with the lowest quartile, the hazard ratio for stroke and SEE was 1.83 (95% CI: ), whereas mortality was lower in the top quartile (HR 0.64; 95% CI: ). There was no relationship between bleeding and quartiles of BP. The proportion of subjects with mean systolic BP at least 140 mmHg was 35.8% (1220/3407) in SPORTIF III and 20.6% (807/3922) in SPORTIF V (p<0.0001). There was a higher stroke rate observed in SPORTIF III which may be related to the greater proportion of subjects with SBP of at least 140 mmHg during the trial. Reference Lip GY et al; for the SPORTIF Investigators. Effect of hypertension on anticoagulated patients with atrial fibrillation. Eur Heart J 2007;28:752-9. TAS = tension artérielle systolique Lip, GY. et autres. for the SPORTIF Investigators, European Heart Journal, 28:752-9, 2007. 27
 0,5. 1,0. 1,5. 2,0. 2,5. 3,0. 3,5. 4,0. TAS MOYENNE (en mmHg) Hypertension contributes to increased stroke and systemic embolus in AF. This graph emanates from a cross-sectional, longitudinal analysis of data from the SPORTIF III and V trials. It showed an increasing rate of stroke and SEE with increasing quartiles of systolic blood pressure. In the combined SPORTIF III and V cohort, the event rate for stroke/SEE increased markedly at mean SBP above 140 mmHg, as shown by the blue arrow. When the top quartile of SBP was compared with the lowest quartile, the hazard ratio for stroke and SEE was 1.83 (95% CI: ), whereas mortality was lower in the top quartile (HR 0.64; 95% CI: ). There was no relationship between bleeding and quartiles of BP. The proportion of subjects with mean systolic BP at least 140 mmHg was 35.8% (1220/3407) in SPORTIF III and 20.6% (807/3922) in SPORTIF V (p<0.0001). There was a higher stroke rate observed in SPORTIF III which may be related to the greater proportion of subjects with SBP of at least 140 mmHg during the trial. Reference. Lip GY et al; for the SPORTIF Investigators. Effect of hypertension on anticoagulated patients with atrial fibrillation. Eur Heart J 2007;28: TAS = tension artérielle systolique. Lip, GY. et autres. for the SPORTIF Investigators, European Heart Journal, 28:752-9,")
29
Numéro de décembre

30
ÉPIDÉMIE DE FA!

31
La pathophysiologie de l’AIC associé à la FA
Près de 16 % des AIC sont associés à la FA, et 10 % sont probablement attribuables à une embolie de l’appendice auriculaire gauche Embolism of left atrial appendage thrombi accounts for most strokes in AF patients, particularly the larger and more disabling strokes. Based on the best available clinical estimates, about two thirds of strokes in AF patients are due to atrial thrombi; however, this does vary according to the distribution of additional risk factors and antithrombotic therapy; high-risk AF patients have a particularly high proportion of cardioembolic strokes. Overall, approximately 10% of all ischemic strokes in population-based cohorts are due to embolism of left atrial appendage thrombi in AF patients. Reference Hart, R. G. et al. Atrial fibrillation and stroke : concepts and controversies. Stroke 2001;32: Fibrillation auriculaire / 16 % des infarctus cérébraux Plaque de la crosse aortique / Athérosclérose de la carotide / Autres maladies du cœur / Petits vaisseaux sanguins / Thrombus auriculaire gauche / 10 % des infarctus cérébraux FA = fibrillation auriculaire Hart, RG. et JL. Halperin. Stroke, 32: , 2001.

32
Appendice auriculaire gauche (AAG)
L’appendice auriculaire gauche (AAG) est le site le plus fréquent de la formation de thrombus chez les patients atteints de FA Left atrial appendage is the most common site for thrombus formation in patients with AF Reference Image courtesy of Albers G, Stanford Stroke Center, Stanford School of Medicine FA = fibrillation auriculaire Image offerte gracieusement par Albers, G. Stanford Stroke Center, Stanford School of Medicine
 est le site le plus fréquent de la formation de thrombus chez les patients atteints de FA. Left atrial appendage is the most common site for thrombus formation in patients with AF. Reference. Image courtesy of Albers G, Stanford Stroke Center, Stanford School of Medicine. FA = fibrillation auriculaire. Image offerte gracieusement par Albers, G. Stanford Stroke Center, Stanford School of Medicine.")
37
Prévention des AVC liés à la FA
- Efficacité et sécurité des traitements actuels contre la FA - Métaanalyse du traitement antithrombotique de la FA New Hart.Ann Intern Med.Jun.2007/ p857/ c1/lines A18-A19, C2/line A1 van Walraven. JAMA.Nov.2002/ p2441/ lines A19 Fuster.J Am Coll Cardiol.Aug.2006/ pe183/table 12 Des doses ajustées de warfarine et d’inhibiteurs de l’agrégation plaquettaire se sont avérées aptes à réduire le risque d’AVC dans des proportions respectives de 64 % et de 22 % avec un risque accru d’hémorragie, comparativement au contrôle La warfarine s’est avérée plus apte que l’Aspirin à réduire les AVC dans une proportion de 45 %, mais avec un risque accru d’hémorragie En se fondant sur ces conclusions, on recommande la warfarine et les autres anticoagulants oraux (ACO) chez les patients à risque accru d’AVC et l’Aspirin chez les patients à risque inférieur Hart.Ann Intern Med.Jun.2007/p857/ c1/lines A18-A19, C2/line A1 Hart.Ann Intern Med.Jun.2007/ p864/ table 5 Note: This slide contains off-label information regarding PLAVIX, and should not be used in promotional presentations except in response to unsolicited questions from the audience. Adjusted-dose warfarin and antiplatelet agents have been shown to reduce the risk of stroke compared with control by 64% and 22%, respectively, with an increase in the number of bleeding events including intracranial hemorrhage and major extracranial hemorrhage.[1] Warfarin has been shown to be more effective than aspirin, in reducing stroke by 45%, but increasing the risk of bleeding.[2] Based on these results, warfarin and other oral anticoagulants (OAC) are recommended for patients at increased risk of stroke; and aspirin is recommended for patients at lower risk.[3] Hart.Ann Intern Med.Jun.2007/p857/ c1/lines A18-A19, C2/line A1 van Walraven. JAMA.Nov.2002/p2441/ lines A19 Fuster.J Am Coll Cardiol.Aug.2006/ pe183/table 12 W % Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146: van Walraven C, Hart RG, Singer DE, Laupacis A, Connolly S, Petersen P, et al. Oral anticoagulants vs aspirin in nonvalvular atrial fibrillation: an individual patient meta-analysis. JAMA. 2002;288: Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation); Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2006;48:e A W % Annals of Internal Medicine, 146: , 2007. Réduction du risque d’AVC / Résultats en matière de sécurité / AIC / ECH majeur 37
 chez les patients à risque accru d’AVC et l’Aspirin chez les patients à risque inférieur. Hart.Ann Intern Med.Jun.2007/p857/ c1/lines A18-A19, C2/line A1. Hart.Ann Intern Med.Jun.2007/ p864/ table 5. Note: This slide contains off-label information regarding PLAVIX, and should not be used in promotional presentations except in response to unsolicited questions from the audience. Adjusted-dose warfarin and antiplatelet agents have been shown to reduce the risk of stroke compared with control by 64% and 22%, respectively, with an increase in the number of bleeding events including intracranial hemorrhage and major extracranial hemorrhage.[1] Warfarin has been shown to be more effective than aspirin, in reducing stroke by 45%, but increasing the risk of bleeding.[2] Based on these results, warfarin and other oral anticoagulants (OAC) are recommended for patients at increased risk of stroke; and aspirin is recommended for patients at lower risk.[3] Hart.Ann Intern Med.Jun.2007/p857/ c1/lines A18-A19, C2/line A1. van Walraven. JAMA.Nov.2002/p2441/ lines A19. Fuster.J Am Coll Cardiol.Aug.2006/ pe183/table 12. W. % Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146: van Walraven C, Hart RG, Singer DE, Laupacis A, Connolly S, Petersen P, et al. Oral anticoagulants vs aspirin in nonvalvular atrial fibrillation: an individual patient meta-analysis. JAMA. 2002;288: Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation); Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2006;48:e A. W. % Annals of Internal Medicine, 146: , Réduction du risque d’AVC / Résultats en matière de sécurité / AIC / ECH majeur. 37.")
38
Le défi de la warfarine : Sa fenêtre thérapeutique étroite
Rapport entre les événements cliniques et le RIN Warfarin—while highly effective in reducing the risk for stroke—is associated with a number of important limitations. Of these, the fact that warfarin has a narrow therapeutic window is among the most important. The data shown on this slide comes from 2 case-controlled studies that evaluated the relationship of INR to intracranial bleeding and ischemic stroke. The 1994 study included 121 adult patients who were hospitalized for intracranial hemorrhage while taking warfarin.1 In this study, the INR was the dominant risk factor for intracranial bleeding. In the second study, the risk of stroke in 74 patients with AF rose steeply at INRs below 2.2 It is clear from this graph that warfarin has a narrow therapeutic window, with an increased risk of ischemic stroke when the INR is <2, and an increased risk of bleeding when the INR >3. References 1. Hylek EM, Singer DE. Risk factors for intracranial hemorrhage in outpatients taking warfarin. Ann Intern Med. 1994;120: 2. Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest effective intensity of prophylactic anticoagulation for patients with nonrheumatic atrial fibrillation. N Engl J Med. 1996;335: Fenêtre thérapeutique / Rapport de probabilités / Accident ischémique cérébral / HIC / RIN HIC = hémorragie intracrânienne RIN = rapport international normalisé 1. Hylek, EM. et autres. Annals of Internal Medicine, 120: , 1994. 2. Hylek, EM. et autres. New England Journal of Medicine, 335: , 1996.

39
Limites du traitement à l'aide de la warfarine
Réaction imprévisible Ajustements fréquents de la dose Les diverses limites de la warfarine compliquent son usage dans la pratique Fenêtre thérapeutique étroite (RIN de 2 - 3) Nombreuses interactions avec les aliments Due to the limitations of warfarin, it has been estimated that up to 50% of patients eligible for treatment receive no anticoagulant treatment.1 References Rowan SB, et al. Trends in Anticoagulation for Atrial Fibrillation in the U.S. An Analysis of the National Ambulatory Medical Care Survey Database. J Am Coll Cardiol 2007;49:1561–5. 2. Ansell J, et al. Pharmacology and Management of the Vitamin K Antagonists. ACCP Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133:160S-198S. 3. Umer Ushman MH, et al. Advancement in antithrombotics for stroke prevention in atrial fibrillation.J Interv Card Electrophysiol 2008; 22: 4. Nutescu EA, et al. New anticoagulant agents: direct thrombin inhibitors.Cardiol Clin 2008; 26: Surveillance régulière de la coagulation Nombreuses interactions avec les autres médicaments Lents début/arrêt de l’action Résistance à la warfarine Ansell, J. et autres. Chest, 133:160S-198S, Umer Ushman, MH. et autres. Journal of Interventional Cardiac Electrophysiology, 22: , Nutescu, EA. et autres. Cardiol Clin, 26: , 2008.
 Nombreuses interactions avec les aliments. Due to the limitations of warfarin, it has been estimated that up to 50% of patients eligible for treatment receive no anticoagulant treatment.1. References. Rowan SB, et al. Trends in Anticoagulation for Atrial Fibrillation in the U.S. An Analysis of the National Ambulatory Medical Care Survey Database. J Am Coll Cardiol 2007;49:1561–5. 2. Ansell J, et al. Pharmacology and Management of the Vitamin K Antagonists. ACCP Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133:160S-198S. 3. Umer Ushman MH, et al. Advancement in antithrombotics for stroke prevention in atrial fibrillation.J Interv Card Electrophysiol 2008; 22: Nutescu EA, et al. New anticoagulant agents: direct thrombin inhibitors.Cardiol Clin 2008; 26: Surveillance régulière de la coagulation. Nombreuses interactions avec les autres médicaments. Lents début/arrêt de l’action. Résistance à la warfarine. Ansell, J. et autres. Chest, 133:160S-198S, Umer Ushman, MH. et autres. Journal of Interventional Cardiac Electrophysiology, 22: , Nutescu, EA. et autres. Cardiol Clin, 26: ,")
40
Contrôle du RIN dans les essais cliniques vs la pratique clinique
Contrôle du RIN* dans les essais cliniques vs la pratique clinique (DMT**) 66 % Essai clinique1 Pratique clinique2 44 % Time in Therapeutic Range (TTR) of with warfarin tends to be highest (60–70%) in well-controlled environments, e.g. clinical trials1 INR control tends to be much lower in clinical practice.2 In a retrospective review in clinical practice setting: relative risk reduction of stroke was only 38%.3 References Kalra L, et al. Prospective cohort study to determine if trial efficacy of anticoagulation for stroke prevention in atrial fibrillation translates into clinical effectiveness. BMJ 2000;320: Matchar DB, et al. Improving the quality of anticoagulation of patients with atrial fibrillation in managed care organizations: results of the managing anticoagulation services trial. Am J Med 2002; 113:42-51. 3. Rietbrock S, et al. How effective are dose-adjusted warfarin and aspirin for the prevention of stroke in patients with chronic atrial fibrillation? An analysis of the UK General Practice Research Database. Thromb Haemost. 2009; 101: 38 % % de patients admissibles recevant de la warfarine 25 % 18 % 9 % <2,0 2,0 – 3,0 RIN>3,0 *RIN = rapport international normalisé ** DMT = durée de la marge thérapeutique (RIN de 2,0 – 3,0) 1. Kalra, L. et autre. BMJ, 320: , 2000. 2. Matchar, DB. et autres. Am J Med, 113:42-51, 2002. Données totalisées : allant de 83 % et 71 % des essais personnalisés
 66 % Essai clinique1. Pratique clinique2. 44 % Time in Therapeutic Range (TTR) of with warfarin tends to be highest (60–70%) in well-controlled environments, e.g. clinical trials1. INR control tends to be much lower in clinical practice.2. In a retrospective review in clinical practice setting: relative risk reduction of stroke was only 38%.3. References. Kalra L, et al. Prospective cohort study to determine if trial efficacy of anticoagulation for stroke prevention in atrial fibrillation translates into clinical effectiveness. BMJ 2000;320: Matchar DB, et al. Improving the quality of anticoagulation of patients with atrial fibrillation in managed care organizations: results of the managing anticoagulation services trial. Am J Med 2002; 113: Rietbrock S, et al. How effective are dose-adjusted warfarin and aspirin for the prevention of stroke in patients with chronic atrial fibrillation An analysis of the UK General Practice Research Database. Thromb Haemost. 2009; 101: % % de patients admissibles recevant de la warfarine. 25 % 18 % 9 % <2,0. 2,0 – 3,0. RIN>3,0. *RIN = rapport international normalisé. ** DMT = durée de la marge thérapeutique (RIN de 2,0 – 3,0) 1. Kalra, L. et autre. BMJ, 320: , Matchar, DB. et autres. Am J Med, 113:42-51, Données totalisées : allant de 83 % et 71 % des essais. personnalisés.")
41
Prévention des AVC liés à la FA
- Le programme ACTIVE FA documentée + 1 facteur de risque : 75 ans, hypertension, AVC/AIT antérieurs, FEVG<45, MAP, 55 – 74 ans + coronaropathie ou diabète Contre-indications à la warfarine ou réticence ACTIVE is a phase III, multicenter, multinational, parallel randomized controlled evaluation of clopidogrel plus ASA, with factorial evaluation of irbesartan, for the prevention of vascular events in patients with atrial fibrillation. Patients will be enrolled over 2 years and followed to common termination date (expected to be about 4 years after enrollment of the first patient). About 14,000 patients will be included in the ACTIVE W or ACTIVE A trials. Due to the partial factorial design, patients will only be randomized in ACTIVE I once first randomized into either ACTIVE A or ACTIVE W. Three separate but related trials are included in the ACTIVE study. These are known as ACTIVE W, ACTIVE A, and ACTIVE I. ACTIVE W (n= 6,500): A multicenter, prospective, randomized, non-inferiority trial of clopidogrel plus ASA versus standard care oral anticoagulation (open trial with blinded outcome evaluation). ACTIVE A (n= 7,500): A multicenter, randomized, double-blind, placebo-controlled superiority trial of clopidogrel plus ASA versus ASA alone. ACTIVE I (n= at least 10,000): A multicenter, partial factorial, randomized, double-blind, placebo-controlled superiority trial of irbesartan. ACTIVE W Clopidogrel+ASA vs warfarine ACTIVE A patients Clopidogrel+ASA vs ASA 6 500 patients Aucun critère d’exclusion dans le cas de l’ACTIVE I ACTIVE I Irbesartan vs placébo ~9 000 patients
. About 14,000 patients will be included in the ACTIVE W or ACTIVE A trials. Due to the partial factorial design, patients will only be randomized in ACTIVE I once first randomized into either ACTIVE A or ACTIVE W. Three separate but related trials are included in the ACTIVE study. These are known as ACTIVE W, ACTIVE A, and ACTIVE I. ACTIVE W (n= 6,500): A multicenter, prospective, randomized, non-inferiority trial of clopidogrel plus ASA versus standard care oral anticoagulation (open trial with blinded outcome evaluation). ACTIVE A (n= 7,500): A multicenter, randomized, double-blind, placebo-controlled superiority trial of clopidogrel plus ASA versus ASA alone. ACTIVE I (n= at least 10,000): A multicenter, partial factorial, randomized, double-blind, placebo-controlled superiority trial of irbesartan. ACTIVE W. Clopidogrel+ASA vs warfarine. ACTIVE A patients. Clopidogrel+ASA vs ASA patients. Aucun critère d’exclusion dans le cas de l’ACTIVE I. ACTIVE I. Irbesartan vs placébo. ~9 000 patients.")
42
Prévention des AVC liés à la FA
- AVC, embolie, IM et mortalité vasculaire - L’étude ACTIVE-W 5,64 %/an RR = 1,45 P = 0,0002 Taux de risque cumulatifs 3,93 %/an Lancet, 367: , 2006 Années OAC = ACO – anticoagulants oraux

43
Prévention des AVC liés à la FA
- Hémorragie majeure - L’étude ACTIVE-W 2,4 %/an RR = 1,06 P = 0,67 2, 2 %/an Taux de risque cumulatifs OAC = ACO – anticoagulants oraux Années Lancet, 367: , 2006.

44
Prévention des AVC liés à la FA
- Le programme ACTIVE AF documentée + 1 facteur de risque : 75 ans, hypertension, AVC/AIT antérieurs, FEVG<45, MAP, ans+ coronaropathie ou diabète Contre-indications à la warfarine ou réticence ACTIVE is a phase III, multicenter, multinational, parallel randomized controlled evaluation of clopidogrel plus ASA, with factorial evaluation of irbesartan, for the prevention of vascular events in patients with atrial fibrillation. Patients will be enrolled over 2 years and followed to common termination date (expected to be about 4 years after enrollment of the first patient). About 14,000 patients will be included in the ACTIVE W or ACTIVE A trials. Due to the partial factorial design, patients will only be randomized in ACTIVE I once first randomized into either ACTIVE A or ACTIVE W. Three separate but related trials are included in the ACTIVE study. These are known as ACTIVE W, ACTIVE A, and ACTIVE I. ACTIVE W (n= 6,500): A multicenter, prospective, randomized, non-inferiority trial of clopidogrel plus ASA versus standard care oral anticoagulation (open trial with blinded outcome evaluation). ACTIVE A (n= 7,500): A multicenter, randomized, double-blind, placebo-controlled superiority trial of clopidogrel plus ASA versus ASA alone. ACTIVE I (n= at least 10,000): A multicenter, partial factorial, randomized, double-blind, placebo-controlled superiority trial of irbesartan. ACTIVE W Clopidogrel+ASA vs warfarine ACTIVE A Clopidogrel+ASA vs ASA 7 500 patients 6 500 patients Aucun critère d’exclusion dans le cas de l’ACTIVE I ACTIVE I Irbesartan vs placébo ~9 000 patients
. About 14,000 patients will be included in the ACTIVE W or ACTIVE A trials. Due to the partial factorial design, patients will only be randomized in ACTIVE I once first randomized into either ACTIVE A or ACTIVE W. Three separate but related trials are included in the ACTIVE study. These are known as ACTIVE W, ACTIVE A, and ACTIVE I. ACTIVE W (n= 6,500): A multicenter, prospective, randomized, non-inferiority trial of clopidogrel plus ASA versus standard care oral anticoagulation (open trial with blinded outcome evaluation). ACTIVE A (n= 7,500): A multicenter, randomized, double-blind, placebo-controlled superiority trial of clopidogrel plus ASA versus ASA alone. ACTIVE I (n= at least 10,000): A multicenter, partial factorial, randomized, double-blind, placebo-controlled superiority trial of irbesartan. ACTIVE W. Clopidogrel+ASA vs warfarine. ACTIVE A. Clopidogrel+ASA vs ASA patients patients. Aucun critère d’exclusion dans le cas de l’ACTIVE I. ACTIVE I. Irbesartan vs placébo. ~9 000 patients.")
45
Prévention des AVC liés à la FA
- AVC, embolie, IM et mortalité vasculaire - L’étude ACTIVE-A New ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2, p7/fig 1A (inset) 0.4 11 % RRR RR = 0,89 (IC à 95 %, 0,81 – 0,98; P = 0,01) 924 (7,6 %/an) 0.3 Note: This slide contains off-label information regarding PLAVIX, and should not be used in promotional presentations except in response to unsolicited questions from the audience. In the ACTIVE A trial, the primary endpoint occurred in 7.6% of patients per year treated with ASA compared with 6.8% of patients per year treated with clopidogrel + ASA. This represented an 11% relative risk reduction (RRR) in patients treated with clopidogrel + ASA vs ASA alone (RR=0.89; 95% CI, 0.81 to 0.98; P=0.01). Reduction in the primary endpoint was driven by a significant RRR in stroke of 28% (RR=0.72; 95% CI, 0.62 to 0.83; P<0.001) ASA 832 (6,8 %/an) Incidence cumulative 0.2 ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2 Clopidogrel + ASA 0.1 0.0 1 2 3 4 Années New England Journal of Medicine, 360: , 2009. ACTIVE Investigators. Effect of clopidogrel added to aspirin in patients with atrial fibrillation [published online ahead of print March 31, 2009]. N Engl J Med. doi: /NEJMoa 45
 % RRR RR = 0,89 (IC à 95 %, 0,81 – 0,98; P = 0,01) 924 (7,6 %/an) 0.3. Note: This slide contains off-label information regarding PLAVIX, and should not be used in promotional presentations except in response to unsolicited questions from the audience. In the ACTIVE A trial, the primary endpoint occurred in 7.6% of patients per year treated with ASA compared with 6.8% of patients per year treated with clopidogrel + ASA. This represented an 11% relative risk reduction (RRR) in patients treated with clopidogrel + ASA vs ASA alone (RR=0.89; 95% CI, 0.81 to 0.98; P=0.01). Reduction in the primary endpoint was driven by a significant RRR in stroke of 28% (RR=0.72; 95% CI, 0.62 to 0.83; P<0.001) ASA. 832 (6,8 %/an) Incidence cumulative ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2. Clopidogrel + ASA Années. New England Journal of Medicine, 360: , ACTIVE Investigators. Effect of clopidogrel added to aspirin in patients with atrial fibrillation [published online ahead of print March 31, 2009]. N Engl J Med. doi: /NEJMoa")
46
Prévention des AVC liés à la FA
- AVC (tout type) - L’étude ACTIVE-A New ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2, p7/fig 1B (inset) RRR de 28 % RR = 0,72 (IC à 95 %, 0,62 – 0,83; P = <0,001) 0,15 408 (3,3 %/an) ASA Note: This slide contains off-label information regarding PLAVIX, and should not be used in promotional presentations except in response to unsolicited questions from the audience. In the ACTIVE A trial, stroke was a component of the primary endpoint and occurred in 3.3% of patients per year treated with ASA compared with 2.4% of patients per year treated with clopidogrel + ASA. This represents a 28% RRR in patients treated with clopidogrel + ASA vs ASA alone (RR=0.72; 95% CI, 0.62 to 0.83; P<0.001). 0,10 Incidence cumulative 296 (2,4 %/an) ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2, p7/fig 1B 0,05 Clopidogrel + ASA 0,0 1 2 3 4 Années New England Journal of Medicine, 360: , 2009. ACTIVE Investigators. Effect of clopidogrel added to aspirin in patients with atrial fibrillation [published online ahead of print March 31, 2009]. N Engl J Med. doi: /NEJMoa 46
 - L’étude ACTIVE-A. New. ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2, p7/fig 1B (inset) RRR de 28 % RR = 0,72 (IC à 95 %, 0,62 – 0,83; P = <0,001) 0, (3,3 %/an) ASA. Note: This slide contains off-label information regarding PLAVIX, and should not be used in promotional presentations except in response to unsolicited questions from the audience. In the ACTIVE A trial, stroke was a component of the primary endpoint and occurred in 3.3% of patients per year treated with ASA compared with 2.4% of patients per year treated with clopidogrel + ASA. This represents a 28% RRR in patients treated with clopidogrel + ASA vs ASA alone (RR=0.72; 95% CI, 0.62 to 0.83; P<0.001). 0,10. Incidence cumulative. 296 (2,4 %/an) ACTIVE.N Engl J Med.Mar.2009/ p6/tab 2, p7/fig 1B. 0,05. Clopidogrel + ASA. 0, Années. New England Journal of Medicine, 360: , ACTIVE Investigators. Effect of clopidogrel added to aspirin in patients with atrial fibrillation [published online ahead of print March 31, 2009]. N Engl J Med. doi: /NEJMoa")
47
Insuffisance cardiaque congestive
Score CHADS2 1 point pour l’insuffisance cardiaque congestive - C 1 point pour l’Hypertension 1 point pour l’âge ≥ 75 ans - A 1 point pour le Diabète sucré 2 points pour les AVC ou AIT antérieurs Score CHADS2* Taux d’AVC 1,9 (1,2 - 3,0) 1 2,8 (2,0 - 3,8) 2 4,0 (3,1 - 5,1) 3 5,9 (4,6 - 7,3) 4 8,5 (6,3 – 11,1) 5 12,5 (8,2 – 17,5) 6 18,2 (10,5 – 17,4) *Score de 0 : Les patients peuvent recevoir de l’Aspirin *Score de 1 : Les patients peuvent recevoir de l’Aspirin ou un anticoagulant *Score de ≥2 : Les patients devraient recevoir un anticoagulant CHADS2 is an easy-to use classification scheme that estimates the risk of stroke in elderly patients with AF. Physicians and patients should use CHADS2 to make decisions about antithrombotic therapy based on patient-specific risk of stroke. The CHADS2 index is calculated by assigning 1 point each for the presence of congestive heart failure, history of hypertension, age ≥ 75 years, and diabetes mellitus by assigning 2 points for a history of transient ischemic attack or ischemic stroke. The CHADS2 score for the patient case (Alice), is 3, calculated as follows: 0 points – Alice does not have congestive heart failure 1 point – Alice is being treated for hypertension 0 points – Alice is less than 75 years old 0 points – Alice does not have diabetes mellitus 2 points – Alice has just suffered her first transient ischemic attack 3 points - Total Reference Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285: Dossier de patient - Alice Affection Points Insuffisance cardiaque congestive Hypertension 1 Âge, 74 ans Diabète sucré AVC/AIT antérieurs 2 Total des points 3 Gage, BF. et autres. JAMA, 285: , 2001.
 1. 2,8 (2,0 - 3,8) 2. 4,0 (3,1 - 5,1) 3. 5,9 (4,6 - 7,3) 4. 8,5 (6,3 – 11,1) 5. 12,5 (8,2 – 17,5) 6. 18,2 (10,5 – 17,4) *Score de 0 : Les patients peuvent recevoir de l’Aspirin. *Score de 1 : Les patients peuvent recevoir de l’Aspirin ou un anticoagulant. *Score de ≥2 : Les patients devraient recevoir un anticoagulant. CHADS2 is an easy-to use classification scheme that estimates the risk of stroke in elderly patients with AF. Physicians and patients should use CHADS2 to make decisions about antithrombotic therapy based on patient-specific risk of stroke. The CHADS2 index is calculated by assigning 1 point each for the presence of congestive heart failure, history of hypertension, age ≥ 75 years, and diabetes mellitus by assigning 2 points for a history of transient ischemic attack or ischemic stroke. The CHADS2 score for the patient case (Alice), is 3, calculated as follows: 0 points – Alice does not have congestive heart failure. 1 point – Alice is being treated for hypertension. 0 points – Alice is less than 75 years old. 0 points – Alice does not have diabetes mellitus. 2 points – Alice has just suffered her first transient ischemic attack. 3 points - Total. Reference. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285: Dossier de patient - Alice. Affection. Points. Insuffisance cardiaque congestive. Hypertension. 1. Âge, 74 ans. Diabète sucré. AVC/AIT antérieurs. 2. Total des points. 3. Gage, BF. et autres. JAMA, 285: ,")
48
CHA2DS2VASc Facteurs de risque Points C ICH H Hypertension
A Âge > 75 D Diabète S AVC/AIT/TE (thrombo-embolie) V Maladies vasculaires (IM, MVP et aortiques) A Âge 65 – 75 ans Sc Catégorie selon le sexe (femmes) (MVP = maladies vasculaires périphériques 1 2
 V Maladies vasculaires (IM, MVP et aortiques) A Âge 65 – 75 ans. Sc Catégorie selon le sexe (femmes) (MVP = maladies vasculaires périphériques")
49
CHA2DS2-VASc Score CHA2DS2-VASc Taux de TE sur 1 an - % 1 2 3 4 5 6 7
1 2 3 4 5 6 7 8 0,7 1,9 4,7 2,3 3,9 4,5 10,1 14,2

50
Facteurs de risque d’hémorragie
Âge ≥ 65 ans AVC antérieur Ulcère gastroduodénal (UGD) antérieur Hémorragie gastro-intestinale antérieure Affections rénales Anémie Thrombocytopénie Maladies du foie Diabète sucré Utilisation d’inhibiteurs de l’agrégation plaquettaire Taux d’hémorragie supérieur chez les patients âgés de ≥ 65 ans vs les patients plus jeunes (taux de risque 2,6, intervalle de confiance à 95 % 1,0 – 6,9) Les taux d’hémorragie croissent selon le nombre de facteurs de risque présents et le taux de risque lié aux autres facteurs, 1,7 (intervalle de confiance à 95 %, 1,1 – 2,6) This information regarding risk factors for bleeding is derived from a randomized, double-blind study, was conducted in which 738 patients who had completed three or more months of warfarin therapy for unprovoked venous thromboembolism were randomly assigned to continue warfarin therapy with a target international normalized ratio (INR) of 2.0 to 3.0 (conventional intensity) or a target INR of 1.5 to 1.9 (low intensity). There was a higher rate of major bleeding episodes among patients 65 years of age or older than among those younger than 65 years (hazard ratio, 2.6 [95 percent confidence interval, 1.0 to 6.9]), and the rate increased with the number of predefined risk factors for bleeding that were present at enrollment (risk factors included an age of 65 years or more, previous stroke, previous peptic ulcer disease, previous gastrointestinal bleeding, renal impairment, anemia, thrombocytopenia, liver disease, diabetes, and use of antiplatelet therapy; hazard ratio associated with each additional risk factor, 1.7 [95 percent confidence interval, 1.1 to 2.6]). Reference Kearon C, et al. Extended Low-Intensity Anticoagulation for Thrombo- Embolism Investigators. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism.N Engl J Med. 2003;349:631-9. Kearon, C. et autres. New England Journal of Medicine, 349: , 2003.
 antérieur. Hémorragie gastro-intestinale antérieure. Affections rénales. Anémie. Thrombocytopénie. Maladies du foie. Diabète sucré. Utilisation d’inhibiteurs de l’agrégation plaquettaire. Taux d’hémorragie supérieur chez les patients âgés de ≥ 65 ans vs les patients plus jeunes (taux de risque 2,6, intervalle de confiance à 95 % 1,0 – 6,9) Les taux d’hémorragie croissent selon le nombre de facteurs de risque présents et le taux de risque lié aux autres facteurs, 1,7 (intervalle de confiance à 95 %, 1,1 – 2,6) This information regarding risk factors for bleeding is derived from a randomized, double-blind study, was conducted in which 738 patients who had completed three or more months of warfarin therapy for unprovoked venous thromboembolism were randomly assigned to continue warfarin therapy with a target international normalized ratio (INR) of 2.0 to 3.0 (conventional intensity) or a target INR of 1.5 to 1.9 (low intensity). There was a higher rate of major bleeding episodes among patients 65 years of age or older than among those younger than 65 years (hazard ratio, 2.6 [95 percent confidence interval, 1.0 to 6.9]), and the rate increased with the number of predefined risk factors for bleeding that were present at enrollment (risk factors included an age of 65 years or more, previous stroke, previous peptic ulcer disease, previous gastrointestinal bleeding, renal impairment, anemia, thrombocytopenia, liver disease, diabetes, and use of antiplatelet therapy; hazard ratio associated with each additional risk factor, 1.7 [95 percent confidence interval, 1.1 to 2.6]). Reference. Kearon C, et al. Extended Low-Intensity Anticoagulation for Thrombo- Embolism Investigators. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism.N Engl J Med. 2003;349: Kearon, C. et autres. New England Journal of Medicine, 349: ,")
51
Contre-indications au recours aux anticoagulants
Grossesse Lié au développement d’anomalies Imminence d’avortement, d’éclampsie et de prééclampsie Chirurgie récente SNC, œil et chirurgies traumatiques, entraînant d’importantes surfaces ouvertes Tendances à l’hémorragie liées à l’ulcération active ou hémorragie apparente GI, GU ou AG Hémorragie vasculaire cérébrale – anévrisme, dissection de l’aorte Péricardite et épanchement péricardique Endocardite bactérienne Patients non suivis Atteints d’alcoolisme Atteints de psychose Autres types de non-coopération Ponction lombaire Tout type de diagnostic ou de procédure thérapeutique pouvant susciter une hémorragie incontrôlable Divers Régionale majeure Anesthésie par infiltration lombaire Hypertension artérielle maligne Hypersensibilité à la warfarine connue This slide reviews warfarin contraindications. Reference RxList. Coumadin: Overdosage & Contraindications. Available at Accessed March 31, 2010. SNC = système nerveux central; GI = gastro-intestinal; GU = génito-urinaire; VG = voies génitales

52
La warfarine et la prévention des AVC chez les patients atteints de FA
AFSAK I SPAF I BAATAF CAFA SPINAF EAFT Tous les essais (n = 6) Dose ajustée de warfarine comparativement au placébo ou au témoin Réduction relative du risque (IC à 95 %) This is data from a meta-analysis of trials characterizingthe efficacy and safety of antithrombotic agents for stroke prevention in patients who have atrial fibrillation. Twenty-nine randomized trials with 28,044 participants (mean age, 71 years; mean follow-up, 1.5 years) were included. The chart shows that compared with the control, adjusted-dose warfarin (6 trials, participants) reduced stroke by 64% (95% CI, 49% to 74%). Additional data demonstrated when only ischemic strokes were considered, adjusted-dose warfarin was associated with a 67% (95% CI, 54% to 77%) relative risk reduction. The analysis also showed that antiplatelet agents reduced stroke by 22% (95% CI, 6% to 35%). Adjusted-dose warfarin was substantially more efficacious than antiplatelet therapy (relative risk reduction, 39% [95% CI, 22% to 52%]) (12 trials, participants). Absolute increases in major extracranial hemorrhage were small (0.3% per year) and all- cause mortality was substantially reduced (26% [95% CI, 3% to 43%) by adjusted-dose warfarin versus control. Reference Hart RG, Pearce LA, and Aguilar MI. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007;146: Favorable à la warfarine/Favorable au placébo ou au contrôle AFSAK I = Étude de Copenhague sur la fibrillation auriculaire, l’Aspirin et l’anticoagulation SPAF I = Étude sur la prévention des AVC liés à la fibrillation auriculaire BAATAF = Essai de la région de Boston sur la fibrillation auriculaire CAFA = Anticoagulation dans le cas de la Fibrillation auriculaire au Canada SPINAF = Prévention des AVC liés à la fibrillation auriculaire non rhumatismale EAFT = Essais européens sur la fibrillation auriculaire Hart, RG.et autres. Annals of Internal Medicine, 46: , 2007
 Dose ajustée de warfarine comparativement au placébo ou au témoin. Réduction relative du risque (IC à 95 %) This is data from a meta-analysis of trials characterizingthe efficacy and safety of antithrombotic agents for stroke prevention in patients who have atrial fibrillation. Twenty-nine randomized trials with 28,044 participants (mean age, 71 years; mean follow-up, 1.5 years) were included. The chart shows that compared with the control, adjusted-dose warfarin (6 trials, 2900 participants) reduced stroke by 64% (95% CI, 49% to 74%). Additional data demonstrated when only ischemic strokes were considered, adjusted-dose warfarin was associated with a 67% (95% CI, 54% to 77%) relative risk reduction. The analysis also showed that antiplatelet agents reduced stroke by 22% (95% CI, 6% to 35%). Adjusted-dose warfarin was substantially more efficacious than antiplatelet therapy (relative risk reduction, 39% [95% CI, 22% to 52%]) (12 trials, participants). Absolute increases in major extracranial hemorrhage were small (0.3% per year) and all- cause mortality was substantially reduced (26% [95% CI, 3% to 43%) by adjusted-dose warfarin versus control. Reference. Hart RG, Pearce LA, and Aguilar MI. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007;146: Favorable à la warfarine/Favorable au placébo ou au contrôle. AFSAK I = Étude de Copenhague sur la fibrillation auriculaire, l’Aspirin et l’anticoagulation. SPAF I = Étude sur la prévention des AVC liés à la fibrillation auriculaire. BAATAF = Essai de la région de Boston sur la fibrillation auriculaire. CAFA = Anticoagulation dans le cas de la Fibrillation auriculaire au Canada. SPINAF = Prévention des AVC liés à la fibrillation auriculaire non rhumatismale. EAFT = Essais européens sur la fibrillation auriculaire. Hart, RG.et autres. Annals of Internal Medicine, 46: ,")
53
Sous-utilisation de la warfarine dans le cas de la FA*
Près de la moitié des patients à risque élevé atteints de fibrillation auriculaire reçoivent de la warfarine Recours à la warfarine Non-recours à la warfarine 13 community hospitals 21 academic hospitals This is data from a retrospective cohort study of inpatients was performed at 21 teaching, 13 community, and 4 Veterans Administration hospitals in the US. Among the 945 patients studied, the mean age was 71.5 (± 13.5) years; 43% were >75 years of age, 54.5% were men, and 67% had a history of hypertension. Most (86%) had factors that stratified them as at high risk of stroke, and only 55% of those received warfarin. Neither warfarin nor aspirin were prescribed in 21% of high-risk patients, including 18% of those with a previous stroke, transient ischemic attack, or systemic embolic event. Age >80 years (p = 0.008) and perceived bleeding risk (p = 0.022) were negative predictors of warfarin use. Persistent/permanent AF (p < 0.001) and history of stroke, transient ischemic attack, or systemic embolus (p = 0.014) were positive predictors of warfarin use, whereas high-risk stratification was not. This study confirms the under-use of warfarin, but also adds to published reports in several regards. It showed that risk stratification, the guidepost for treatment in international guidelines, had little effect on warfarin use, and that age >80 years and AF classification (permanent/persistent) are factors that influence warfarin use. Reference Waldo AL et al. Hospitalized patients with atrial fibrillation and a high risk of stroke are not being provided with adequate anticoagulation. J Am Coll Cardiol 2005;46:1729–1736. 13 hôpitaux communautaires 21 hôpitaux universitaires Waldo, AL. et autres. Journal of American College Cardiology, 2005 *Population américaine janvier – décembre 2002
 years; 43% were >75 years of age, 54.5% were men, and 67% had a history of hypertension. Most (86%) had factors that stratified them as at high risk of stroke, and only 55% of those received warfarin. Neither warfarin nor aspirin were prescribed in 21% of high-risk patients, including 18% of those with a previous stroke, transient ischemic attack, or systemic embolic event. Age >80 years (p = 0.008) and perceived bleeding risk (p = 0.022) were negative predictors of warfarin use. Persistent/permanent AF (p < 0.001) and history of stroke, transient ischemic attack, or systemic embolus (p = 0.014) were positive predictors of warfarin use, whereas high-risk stratification was not. This study confirms the under-use of warfarin, but also adds to published reports in several regards. It showed that risk stratification, the guidepost for treatment in international guidelines, had little effect on warfarin use, and that age >80 years and AF classification (permanent/persistent) are factors that influence warfarin use. Reference. Waldo AL et al. Hospitalized patients with atrial fibrillation and a high risk of stroke are not being provided with adequate anticoagulation. J Am Coll Cardiol 2005;46:1729– hôpitaux communautaires. 21 hôpitaux universitaires. Waldo, AL. et autres. Journal of American College Cardiology, *Population américaine janvier – décembre")
55
Mise à jour sur les inhibiteurs de l’agrégation plaquettaire et les anticoagulants
- Nouveaux agents antithrombotiques Société canadienne de cardiologie Voie intrinsèque Voie extrinsèque Xll Xl lX TF Fondaparinux VIII VII Coumadin X HFPM (héparine de faible poids moléculaire) V II Héparine XIII Caillot de fibrine 55
 V. II. Héparine. XIII. Caillot de fibrine. 55.")
56
Prévention des AVC liés à la FA
- Nouveaux agents de préventions des AVC Voie intrinsèque Voie extrinsèque Xll Xl lX TF VIII VII X Inhibiteurs directs du facteur Xa - apixaban - rivaroxaban V II Inhibiteurs directs de la thrombine - dabigatran XIII Caillot de fibrine

57
L’étéxilate de dabigatran (un inhibiteur direct de la thrombine) pour le traitement de la FA
Inhibiteur direct et réversible de la thrombine (IDR) Promédicament oral se convertissant en dabigatran Début d’action rapide Demi-vie de h Excrétion rénale ~ 80 % Faible probabilité d’interactions avec les autres médicaments et aucune interaction avec les aliments Absence d’exigences en matière de suivi régulier de la coagulation Dabigatran etexilate is a new oral direct thrombin inhibitor (DTI). It is the prodrug of the active compound, dabigatran, which binds directly to thrombin with a high affinity and specificity. It has a rapid onset of action, with a half-life of between 12 to 17 hours. The majority of the drug (approximately 80%) is renally excreted. Dabigatran has low potential for drug-drug interactions and does not possess drug-food interactions. It has a predictable anticoagulant effect, is adminstered at a fixed dose, and does not require monitoring. Reference Stangier J. Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate. Clin Pharmacokinet 2008;47: Stangier. J. Clin Pharmacokinetics, 47: , 2008.
 Promédicament oral se convertissant en dabigatran. Début d’action rapide. Demi-vie de h. Excrétion rénale ~ 80 % Faible probabilité d’interactions avec les autres médicaments et aucune interaction avec les aliments. Absence d’exigences en matière de suivi régulier de la coagulation. Dabigatran etexilate is a new oral direct thrombin inhibitor (DTI). It is the prodrug of the active compound, dabigatran, which binds directly to thrombin with a high affinity and specificity. It has a rapid onset of action, with a half-life of between 12 to 17 hours. The majority of the drug (approximately 80%) is renally excreted. Dabigatran has low potential for drug-drug interactions and does not possess drug-food interactions. It has a predictable anticoagulant effect, is adminstered at a fixed dose, and does not require monitoring. Reference. Stangier J. Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate. Clin Pharmacokinet 2008;47: Stangier. J. Clin Pharmacokinetics, 47: ,")
58
RE-LY® : Évaluation randomisée de l’anticoagulation à long terme
patients atteints de FA et d’au moins un facteur de risque d’AVC 50 % des patients inscrits n’avaient jamais pris d’ACO Durée médiane du traitement : 2 ans Conclusion principale : AVC ou embolie systémique References Connolly SJ, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361: L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA Connolly, SJ. et autres. New England Journal of Medicine, 61: , 2009.

59
RE-LY® : Critères d’inclusion
Fibrillation auriculaire documentée et Un autre facteur de risque d’AVC : Antécédents d’AVC, d’AIT ou d’embolie systémique FEVG de moins de 40 % Insuffisance cardiaque symptomatique, catégorie II ou plus selon la NYHA 75 ans ou plus 65 ans ou plus et un des autres facteurs de risques suivants : le diabète sucré, une coronaropathie ou l’hypertension L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA Connolly, SJ. et autres. New England Journal of Medicine, 361: , 2009.

60
Baseline characteristics
Dabigatran 110 mg Dabigatran 150 mg Warfarin Randomized 6015 6076 6022 Mean age (years) 71.4 71.5 71.6 Male (%) 64.3 63.2 63.3 CHADS2 score (mean) 0-1 (%) (%) 3+ (%) 2.1 32.6 34.7 32.7 2.2 32.2 35.2 30.9 37.0 32.1 Prior stroke/TIA (%) 19.9 20.3 19.8 Prior MI (%) 16.8 16.9 16.1 CHF (%) 31.8 31.9 Baseline ASA (%) 40.0 38.7 40.6 VKA naïve (%) 50.1 50.2 48.6 Patients were well distributed between the three arm of the trial. There were no significant differences in baseline characteristics between the dabigatran etexilate arms and the warfarin arm. Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:
 Male (%) CHADS2 score (mean) 0-1 (%) 2 (%) 3+ (%) Prior stroke/TIA (%) Prior MI (%) CHF (%) Baseline ASA (%) VKA naïve (%) Patients were well distributed between the three arm of the trial. There were no significant differences in baseline characteristics between the dabigatran etexilate arms and the warfarin arm. Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation. Connolly SJ., et al. N Engl J Med 2009; 361:")
61
Stroke or systemic embolism (SSE)
Noninferiority Superiority p-value p-value Dabigatran 110 mg vs. warfarin <0.001 0.30 Both dosages of dabigatran etexilate met the non-inferiority criteria (p value < 0.001). The upper limit of the confidence intervals for dabigatran etexilate 110 mg BID was far below the non-inferiority margin of Dabigatran 150 mg BID demonstrated superiority with the point of estimate and 95% CI well below the line of unity and a p-value of < (superiority). Dabigatran 150 mg vs. warfarin <0.001 <0.001 Margin = 1.46 0.50 0.75 1.00 1.25 1.50 HR (95% CI) Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:
. The upper limit of the confidence intervals for dabigatran etexilate 110 mg BID was far below the non-inferiority margin of Dabigatran 150 mg BID demonstrated superiority with the point of estimate and 95% CI well below the line of unity and a p-value of < (superiority). Dabigatran 150 mg. vs. warfarin. < < Margin = HR (95% CI) Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation. Connolly SJ., et al. N Engl J Med 2009; 361:")
62
Time to first stroke / SSE
RR 0.90 (95% CI: 0.74–1.10) p<0.001 (NI) p=0.30 (Sup) 0.05 0.04 RRR 35% Warfarin Dabigatran etexilate 110 mg Dabigatran etexilate 150 mg 0.03 Cumulative hazard rates RR 0.65 (95% CI: 0.52–0.81) p<0.001 (NI) p<0.001 (Sup) 0.02 0.01 0.0 0.5 1.0 1.5 2.0 2.5 Years RR, relative risk; CI, confidence interval; NI, non-inferior; Sup, superior Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:
 p<0.001 (NI) p=0.30 (Sup) RRR. 35% Warfarin. Dabigatran etexilate 110 mg. Dabigatran etexilate 150 mg Cumulative hazard rates. RR (95% CI: 0.52–0.81) p<0.001 (NI) p<0.001 (Sup) Years. RR, relative risk; CI, confidence interval; NI, non-inferior; Sup, superior. Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation. Connolly SJ., et al. N Engl J Med 2009; 361:")
63
All cause mortality RR 0.91 (95% CI: 0.80–1.03) p=0.13 (sup)
% per year 446 / 6,015 438 / 6,076 487 / 6,022 Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:

64
Major bleeding rates RR 0.80 (95% CI: 0.70–0.93) p=0.003 (sup)
RRR 20% % per year 342 / 6,015 399 / 6,076 421 / 6,022 Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:

65
Hemorrhagic stroke 50 45 40 30 20 14 10 12 D110 mg BID D150 mg BID
RR 0.31 (95% CI: 0.17–0.56) p<0.001 (sup) RR 0.26 (95% CI: 0.14–0.49) p<0.001 (sup) 50 Number of events 45 40 RRR 69% RRR 74% 0.38% Both dosages of dabigatran etexilate significantly reduced the incidence of hemorrhagic stroke (one element of the primary efficacy endpoint including stroke and systemic embolism) compared to warfarin: The relative risk reduction (RRR) for dabigatran etexilate 110mg BID compared to warfarin was 69%, RRR for dabigatran etexilate 150mg was 74%. 30 20 14 10 12 0.12% 0.10% D110 mg BID D150 mg BID Warfarin 6,015 6,076 6,022 Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:
 p<0.001 (sup) RR 0.26 (95% CI: 0.14–0.49) p<0.001 (sup) 50. Number of events RRR. 69% RRR. 74% 0.38% Both dosages of dabigatran etexilate significantly reduced the incidence of hemorrhagic stroke (one element of the primary efficacy endpoint including stroke and systemic embolism) compared to warfarin: The relative risk reduction (RRR) for dabigatran etexilate 110mg BID compared to warfarin was 69%, RRR for dabigatran etexilate 150mg was 74% % 0.10% D110 mg BID. D150 mg BID. Warfarin. 6,015. 6,076. 6,022. Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation. Connolly SJ., et al. N Engl J Med 2009; 361:")
66
RE-LY® : Taux d’IM Caractéristique Infarctus du myocarde (IM) (%/an)
Dabigatran 110 mg (N = 6 015) Dabigatran 150 mg (N = 6 076) Warfarine (N = 6 022) Valeur de p Dabigatran 110 mg vs warfarine Valeur de p Dabigatran 150 mg vs warfarine Infarctus du myocarde (IM) (%/an) 0,82 0,81 0,64 0,09 0,012 The rate of myocardial infarction was 0.53% per year with warfarin and was higher with dabigatran: 0.72% per year in the 110-mg group (relative risk, 1.35; 95% CI, 0.98 to 1.87; P = 0.07) and 0.74% per year in the 150-mg group (relative risk, 1.38, 95% CI, 1.00 to 1.91; P = 0.048). References Connolly SJ, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361: Connolly, SJ. et autres. New England Journal of Medicine, 361: , 2009.
 Dabigatran 150 mg (N = 6 076) Warfarine (N = 6 022) Valeur de p Dabigatran 110 mg vs warfarine. Valeur de p Dabigatran 150 mg vs warfarine. Infarctus du myocarde (IM) (%/an) 0,82. 0,81. 0,64. 0,09. 0,012. The rate of myocardial infarction was 0.53% per year with warfarin and was higher with dabigatran: 0.72% per year in the 110-mg group (relative risk, 1.35; 95% CI, 0.98 to 1.87; P = 0.07) and 0.74% per year in the 150-mg group (relative risk, 1.38, 95% CI, 1.00 to 1.91; P = 0.048). References. Connolly SJ, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361: Connolly, SJ. et autres. New England Journal of Medicine, 361: ,")
67
Time to first intra-cranial bleed
Warfarin Dabigatran etexilate 110 mg Dabigatran etexilate 150 mg 0.02 RRR 59% RRR 70% Cumulative hazard rates 0.01 RR 0.41 (95% CI: 0.28–0.60) p<0.001 (Sup) RR 0.30 (95% CI: 0.19–0.45) p<0.001 (Sup) 0.0 0.5 1.0 1.5 2.0 2.5 Years RR, Relative risk; CI, confidence interval; Sup, superior Connolly SJ., et al. N Engl J Med 2009; 361: Adapted from Camm J.: Oral presentation at ESC on Aug. 30, Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation
 p<0.001 (Sup) RR (95% CI: 0.19–0.45) p<0.001 (Sup) Years. RR, Relative risk; CI, confidence interval; Sup, superior. Connolly SJ., et al. N Engl J Med 2009; 361: Adapted from Camm J.: Oral presentation at ESC on Aug. 30, Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation.")
68
Vascular mortality 2.69 2.43 2.28 RR 0.90 (95% CI: 0.77–1.06)
p=0.21 (sup) RR 0.85 (95% CI: 0.72–0.99) p=0.04 (sup) % per year 2.69 RRR 15% 2.43 2.28 Regarding vascular mortality, dabigatran etexilate 150mg BID was superior to warfarin with p=0.038. Dabigatran etexilate 110mg BID was statistically comparable to warfarin regarding vascular mortality. However, numerically there were fewer deaths with dabigatran etexilate 110mg BID compared to warfarin. Definition of vascular mortality: Vascular mortality includes both cardiovascular death and other types of vascular death: Cardiovascular death : - Sudden / arrhythmic death (e.g. documented asystole, documented ventricular flutter/fibrillation, recent myocardial infarction, other) - Pump failure death (e.g. cardiac heart failure/cardiac shock, cardiac tamponade, recent myocardial infarction, other) Other vascular death: resulting from stroke, pulmonary embolus, peripheral embolus, haemorrhage, unknown cause (but still classifiable as "vascular"), other 289/ 6,015 274 / 6,076 317 / 6,022 Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Connolly SJ., et al. N Engl J Med 2009; 361:
 RR 0.85 (95% CI: 0.72–0.99) p=0.04 (sup) % per year RRR. 15% Regarding vascular mortality, dabigatran etexilate 150mg BID was superior to warfarin with p= Dabigatran etexilate 110mg BID was statistically comparable to warfarin regarding vascular mortality. However, numerically there were fewer deaths with dabigatran etexilate 110mg BID compared to warfarin. Definition of vascular mortality: Vascular mortality includes both cardiovascular death and other types of vascular death: Cardiovascular death : - Sudden / arrhythmic death (e.g. documented asystole, documented ventricular flutter/fibrillation, recent myocardial infarction, other) - Pump failure death (e.g. cardiac heart failure/cardiac shock, cardiac tamponade, recent myocardial infarction, other) Other vascular death: resulting from stroke, pulmonary embolus, peripheral embolus, haemorrhage, unknown cause (but still classifiable as vascular ), other. 289/ 6, / 6, / 6,022. Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation. Connolly SJ., et al. N Engl J Med 2009; 361:")
69
RE-LY® : Effets indésirables les plus répandus
Dabigatran 110 mg (%) Dabigatran 150 mg (%) Warfarine (%) Dyspepsie* 11,8 11,3 5,8 Dyspnée 9,3 9,5 9,7 Étourdissement 8,1 8,3 9,4 Œdème périphérique 7,9 7,8 Fatigue 6,6 6,2 Toux 5,7 6,0 Douleur thoracique 5,2 5,9 Arthralgie 4,5 5,5 Douleur dorsale 5,3 5,6 Rhinopharyngite 5,4 Diarrhée 6,3 6,5 Infection urinaire 4,8 Infection des voies respiratoires supérieures 4,7 Overall rates of adverse events were low and similar between the treatment arms. The increase in dyspepsia, or related symptoms, could be related to the dabigatran capsules. To enhance absorption of dabigatran, a low pH is required. Therefore dabigatran capsules contain dabigatran-coated pellets with a tartaric acid core. This acidity may explain the increased incidence of dyspeptic symptoms with dabigatran. Elevations in the serum aspartate aminotransferase (AST) or alanine aminotransferase (ALT) level of more than 3 times the upper limit of the normal range did not occur more frequently with dabigatran, at either dose, than with warfarin. References Connolly SJ., et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361: *S’est produite plus souvent avec le dabigatran p<0,001 Connolly, SJ. et autres. New England Journal of Medicine, 361: , 2009. L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA
 Dabigatran 150 mg (%) Warfarine (%) Dyspepsie* 11,8. 11,3. 5,8. Dyspnée. 9,3. 9,5. 9,7. Étourdissement. 8,1. 8,3. 9,4. Œdème périphérique. 7,9. 7,8. Fatigue. 6,6. 6,2. Toux. 5,7. 6,0. Douleur thoracique. 5,2. 5,9. Arthralgie. 4,5. 5,5. Douleur dorsale. 5,3. 5,6. Rhinopharyngite. 5,4. Diarrhée. 6,3. 6,5. Infection urinaire. 4,8. Infection des voies respiratoires supérieures. 4,7. Overall rates of adverse events were low and similar between the treatment arms. The increase in dyspepsia, or related symptoms, could be related to the dabigatran capsules. To enhance absorption of dabigatran, a low pH is required. Therefore dabigatran capsules contain dabigatran-coated pellets with a tartaric acid core. This acidity may explain the increased incidence of dyspeptic symptoms with dabigatran. Elevations in the serum aspartate aminotransferase (AST) or alanine aminotransferase (ALT) level of more than 3 times the upper limit of the normal range did not occur more frequently with dabigatran, at either dose, than with warfarin. References. Connolly SJ., et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361: *S’est produite plus souvent avec le dabigatran p<0,001. Connolly, SJ. et autres. New England Journal of Medicine, 361: , L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA.")
70
RE-LY® : Résumé des conclusions
Dose de 110 mg versus la warfarine Taux comparables d’AVC/embolies systémiques Réduction statistiquement importante des AVC hémorragiques Réduction statistiquement importante des taux d’hémorragie majeure Réduction importante des hémorragies totales, des hémorragies potentiellement mortelles et des hémorragies intracrâniennes Dose de 150 mg versus la warfarine Réduction statistiquement importante des AVC/embolies systémiques Réduction statistiquement importante de la mortalité vasculaire Taux comparables d’hémorragies majeures References Connolly SJ., et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361: Connolly, SJ. et autres. New England Journal of Medicine, 361: , 2009. L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA

71
Aspects clés On a révisé les lignes directrices suivantes :
Utilisation des traitements antithrombotiques dans le cas de la FA Prévention des thrombo-embolies chez les patients atteints de FA subissant une cardioversion Gestion péri-opératoire des patients recevant des antagonistes de la vitamine K (AVK) Gestion des patients atteints de FA suscitant des préoccupations particulières – infarctus du myocarde, hyperthyroïdie, grossesse et cardiomyopathie hypertrophique Gestion des patients ayant reçu un diagnostic récent de FA - atteints de FA paroxystique récurrente et de FA persistante ou permanente récurrente
 Gestion des patients atteints de FA suscitant des préoccupations particulières – infarctus du myocarde, hyperthyroïdie, grossesse et cardiomyopathie hypertrophique. Gestion des patients ayant reçu un diagnostic récent de FA - atteints de FA paroxystique récurrente et de FA persistante ou permanente récurrente.")
72
Aspects clés La FA aggrave le pronostic des patients atteints de comorbidités La FA augmente les risques au sein du continuum cardiovasculaire L’hypertension est l’un des plus éloquents prédicteurs d’AVC chez les patients atteints de FA Insistance sur une stratégie possible de gestion du remplacement de la warfarine par le dabigatran

73
Gestion des patients de fin de semaine
Gestion des patients qui se présentent le vendredi après-midi Par exemple : Administration initiale de warfarine dès l’admission et vérification du RIN le dimanche ou le lundi selon les possibilités d’interactions avec d’autres médicaments ou les affections sous- jacentes, le cas échéant À quelle fréquence doit-on surveiller les symptômes, la durée à l’intérieur de la marge thérapeutique et l’anticoagulation clinique vs la gestion au bureau Dans le cas de la warfarine, on devrait d’abord exercer un suivi bihebdomadaire jusqu’à l’atteinte de la marge thérapeutique et, par la suite, faire un suivi hebdomadaire jusqu’à deux semaines consécutives à l’intérieur de la marge thérapeutique, suivi d’intervalles de 4 à 6 semaines (CHEST 2008)
")
74
Affections rénales Reference Stangier J. Clinical Pharmacokinetics and Pharmacodynamics of the Oral Direct Thrombin Inhibitor Dabigatran Etexilate. Clin Pharmacokinet 2008; 47: Les affections rénales augmentent l’exposition au dabigatran qui correspond à la gravité des dysfonctions rénales Il est possible de retirer par hémodialyse une partie (62 – 68 %) du dabigatran du plasma L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA Stangier. Clin Pharmacokinet, 49(4): , 2010
 du dabigatran du plasma. L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins. cliniques pour la prévention des AVC chez les patients atteints de FA. Stangier. Clin Pharmacokinet, 49(4): ,")
75
Prévention des AVC liés à la FA
- Apixaban : Un inhibiteur direct oral du facteur Xa L’apixaban est un inhibiteur direct réversible oral du factor Xa L’apixaban se fixe directement au site actif du facteur Xa et ne nécessite aucune antithrombine afin de produire son effet pharmacologique Biodisponibilité de 50 % Atteinte de la concentration maximale dans le plasma 3 ou 4 h après la dose Nombreuses voies d’excrétion, rénale à ~ 27 % T½ de 12 h Absence d’interactions avec les autres médicaments ou les aliments connues Effets anticoagulants prévisibles et conséquents Absence d’exigences en matière de surveillance de la coagulation

76
Prévention des AVC liés à la FA
- L’étude AVERROES - Méthodologie Apixaban 5 mg BID AF et ≥1 facteur de risque et inaptitude manifeste ou prévue dans le cas des AVK 2,5 mg BID chez certains patients Statistical testing in the RE-LY Study: Primary endpoint: Non-inferiority design allowing for statistical analysis of superiority once non-inferiority is achieved All other endpoints: Superiority testing. P < 0.05 superior (95% CI is below 1) P > 0.05 comparable (if 95% CI includes 1) R 5 600 patients À double insu ASA ( mg/d) Objectif principal : Établir la non-infériorité de l’apixaban à 5 mb bid par rapport à l’ASA 81 – 324 mg od Suivi minimal de 1 an, maximal de 3 ans et moyen de 2 ans Présentation auprès de la Société européenne de cardiologie, Stockholm, septembre 2010 76
 P > 0.05 comparable (if 95% CI includes 1) R patients. À double insu. ASA ( mg/d) Objectif principal : Établir la non-infériorité de l’apixaban à 5 mb bid par rapport à l’ASA 81 – 324 mg od. Suivi minimal de 1 an, maximal de 3 ans et moyen de 2 ans. Présentation auprès de la Société européenne de cardiologie, Stockholm, septembre")
77
Prévention des AVC liés à la FA
- L’étude AVEROES - Conclusion principale : AVC ou embolie systémique 0,06 ASA 81 – 324 mg od Apixaban 5 mg bid 0.03 0,05 RRR 54 % 0,04 Risque cumulatif 0,03 0,02 RR 0,46 (IC à 95 % : 0,33 – 0,64) p<0,001 0,01 0,0 3 6 9 12 15 18 21 No à risque Mois 329 626 Présentation auprès de la Société européenne de cardiologie, Stockholm, septembre 2010 ASA 2791 2720 2541 2124 1541 353 617 Apix 2809 2761 2567 2127 1523
 p<0,001. 0,01. 0, No à risque. Mois Présentation auprès de la Société européenne de cardiologie, Stockholm, septembre ASA Apix")
78
Le rivaroxaban (un inhibiteur du facteur Xa) dans le cas de la FA : étude ROCKET
Patients atteints de + ≥2 facteurs de risque de FA : ICH, hypertension, 75 ans ou plus, diabète ou AVC, AIT ou embolie systémique n ~14 000 Rivaroxaban Warfarine 20 mg par jour 15 mg pour la ClCr 30 – 49 Cible du RIN 2,5 (2,0 – 3,0 inclusivement) Suivi mensuel et adhésion aux normes des lignes directrices en matière de soins Effet principal : AVC ou embolie systémique hors système nerveux central (SNC) sur 4 ans (fin prévue de l’étude : mai 2010) AIT : accident ischémique transitoire ClCr : clairance de la créatinine
 Suivi mensuel et adhésion aux normes des lignes directrices en matière de soins. Effet principal : AVC ou embolie systémique hors système nerveux central (SNC) sur 4 ans (fin prévue de l’étude : mai 2010) AIT : accident ischémique transitoire. ClCr : clairance de la créatinine.")
79
Étude ROCKET sur la FA Présentation auprès de l’AHA le 15 novembre 2010 Le rivaroxaban n’est ni inférieur ni supérieur selon les choix de traitement (vs la warfarine) Hémorragies majeures et non majeures comparables Le rivaroxaban provoque moins de décès ou d’hémorragies intracrâniennes Score CHADS2 de 3 ou plus dans 90 % des cas
 Hémorragies majeures et non majeures comparables. Le rivaroxaban provoque moins de décès ou d’hémorragies intracrâniennes. Score CHADS2 de 3 ou plus dans 90 % des cas.")
80
Nouveaux anticoagulants oraux
1- Qui paiera? 2- Évaluation de la conformité? 3- Traitement des complications liées aux hémorragies?

81
Nouveaux anticoagulants oraux
Conformité? Avec l’apixaban : Imagerie isotopique Avec le dabigatran : Temps de coagulation de la thrombine TTPa (temps de thromboplastine partielle activée)
")
82
Nouveaux anticoagulants oraux
Hémorragie souvent contrôlée par des mesures de soutien Le dabigatran est dialysable Agents spécifiques pour l’annulation des effets anticoagulants : Facteur VII activé recombinant CCP (concentrés de complexe prothrombinique)
")
83
Surdose et stratégies d’annulation Preuves scientifiques fondées sur les données d’essais in vitro et sur les animaux Recommandations sur la gestion des surdoses de dabigatran Maintenir ou augmenter la diurèse Administration précoce de charbon Hémoperfusion avec filtre de charbon / hémodialyse Recommandations sur la gestion des hémorragies graves Agents spécifiques pour l’annulation des effets anticoagulants : Facteur VII activé recombinant CCP (concentrés de complexe prothrombinique) Hémodialyse et hémofiltration On procède actuellement à la confirmation in vivo des stratégies d’annulation proposées Van Ryn, J. et autres. Thromb & Haemost, 103: doi: /TH , 2010. L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA
 Hémodialyse et hémofiltration. On procède actuellement à la confirmation in vivo des stratégies d’annulation proposées. Van Ryn, J. et autres. Thromb & Haemost, 103: doi: /TH , L’étéxilate de dabigatran est en développement clinique et ne peut servir à des fins cliniques pour la prévention des AVC chez les patients atteints de FA.")
84
Société canadienne de cardiologie
Mise à jour des lignes directrices en matière de fibrillation auriculaire Introduction Anne M Gillis MD, FRCPC, FHRS Professeure de médecine Département des sciences cardiaques Université de Calgary Libin Cardiovascular Institute of Alberta Leadership – Connaissances - Communauté

85
Recommandations - Antithrombotiques
Société canadienne de cardiologie 2. Nous recommandons d’administrer aux patients à très faible risque d’AVC (CHADS2 = 0) de l’Aspirin ( mg/jour). (Forte recommandation – preuve de qualité élevée). Nous suggérons que certains jeunes ne présentant aucun facteur de risque habituel d’AVC pourraient ne pas nécessiter de traitement antithrombotique. (Recommandation conditionnelle – preuve de qualité modérée) Leadership – Connaissances - Communauté
 de l’Aspirin ( mg/jour). (Forte recommandation – preuve de qualité élevée). Nous suggérons que certains jeunes ne présentant aucun facteur de risque habituel d’AVC pourraient ne pas nécessiter de traitement antithrombotique. (Recommandation conditionnelle – preuve de qualité modérée) Leadership – Connaissances - Communauté.")
86
Recommandations - Antithrombotiques
Société canadienne de cardiologie 3. Nous recommandons d’administrer aux patients à faible risque d’AVC (CHADS2 = 1) un ACO (warfarine [RIN de 2 – 3] ou dabigatran). (Forte recommandation – preuve de qualité élevée). Nous appuyant sur des considérations en matière de risques/avantages individuels, nous suggérons que l’Aspirin est un choix raisonnable dans certains cas. (Recommandation conditionnelle – preuve de qualité modérée) 4. Nous recommandons d’administrer aux patients à risque modéré d’AVC (CHADS2 ≥ 2) un ACO (warfarine [RIN de 2 – 3] ou dabigatran). (Forte recommandation – preuve de qualité élevée) Leadership – Connaissances - Communauté
 un ACO (warfarine [RIN de 2 – 3] ou dabigatran). (Forte recommandation – preuve de qualité élevée). Nous appuyant sur des considérations en matière de risques/avantages individuels, nous suggérons que l’Aspirin est un choix raisonnable dans certains cas. (Recommandation conditionnelle – preuve de qualité modérée) 4. Nous recommandons d’administrer aux patients à risque modéré d’AVC (CHADS2 ≥ 2) un ACO (warfarine [RIN de 2 – 3] ou dabigatran). (Forte recommandation – preuve de qualité élevée) Leadership – Connaissances - Communauté.")
87
Recommandations - Antithrombotiques
Société canadienne de cardiologie Recommandations - Antithrombotiques 5. Nous suggérons, dans les cas où les AOC sont indiqués, d’administrer à la plupart des patients du dabigatran au lieu de la warfarine. En général, la dose de dabigatran à 150 mg po bid s’avère préférable à la dose de 110 mg po (les exceptions sont présentées dans le texte) (Recommandation conditionnelle – preuve de qualité élevée) Leadership – Connaissances - Communauté
 (Recommandation conditionnelle – preuve de qualité élevée) Leadership – Connaissances - Communauté.")
88
Recommandations – coronaropathies stables
Société canadienne de cardiologie Recommandations – coronaropathies stables 10. Nous suggérons d’administrer aux patients atteints de FA ou de flutter auriculaire et de coronaropathies stables un traitement antithrombotique établi en fonction de leur risque d’AVC (Aspirin pour un CHADS2 = 0 et ACO pour un CHADS2 ≥ 1). Il est préférable de recourir à la warfarine au lieu du dabigatran chez les personnes à risque élevé d’événements coronariens. (Recommandation conditionnelle – preuve de qualité modérée) Leadership – Connaissances - Communauté
. Il est préférable de recourir à la warfarine au lieu du dabigatran chez les personnes à risque élevé d’événements coronariens. (Recommandation conditionnelle – preuve de qualité modérée) Leadership – Connaissances - Communauté.")
89
MERCI!

90
QUESTIONS?

Présentations similaires





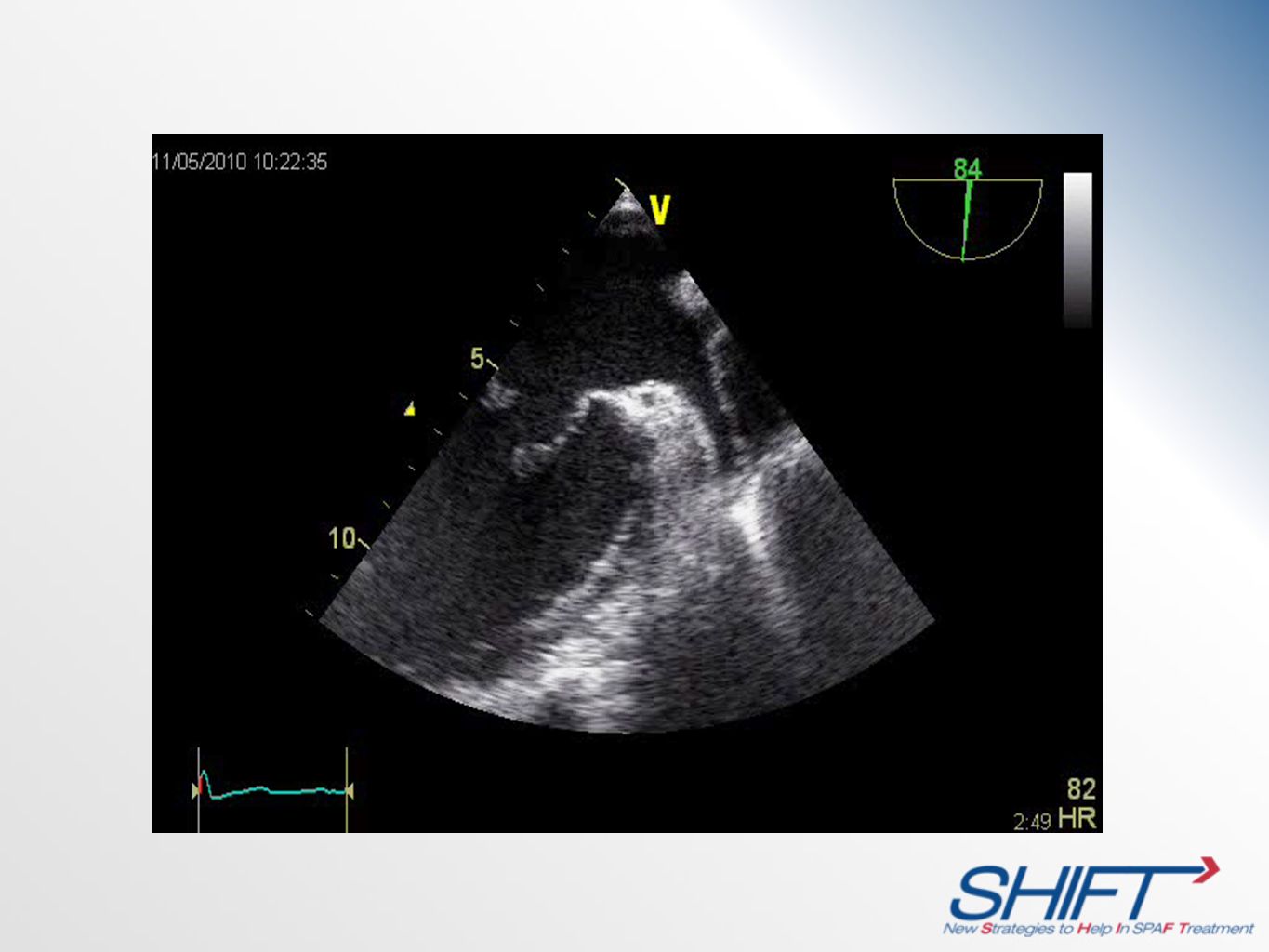
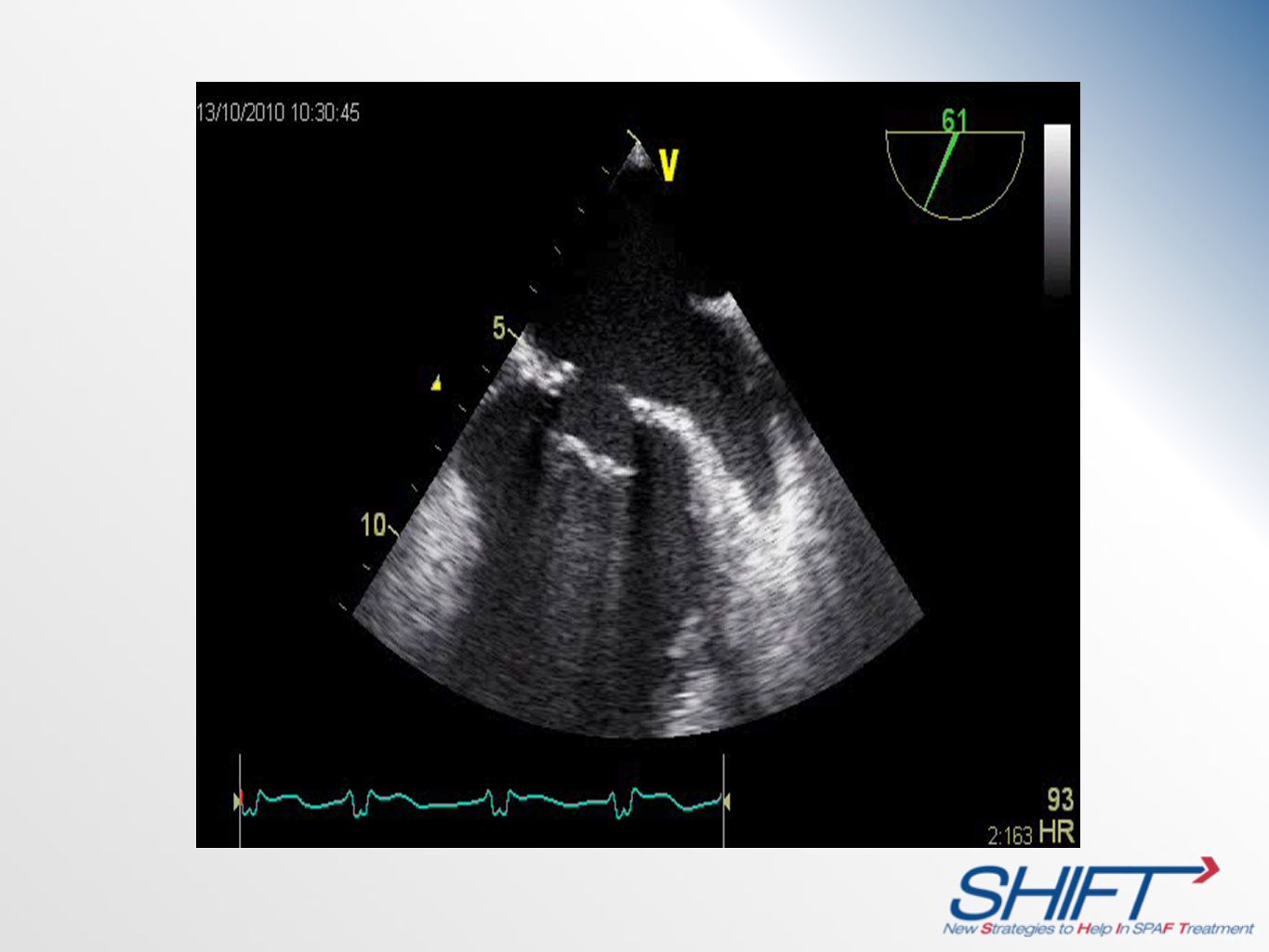
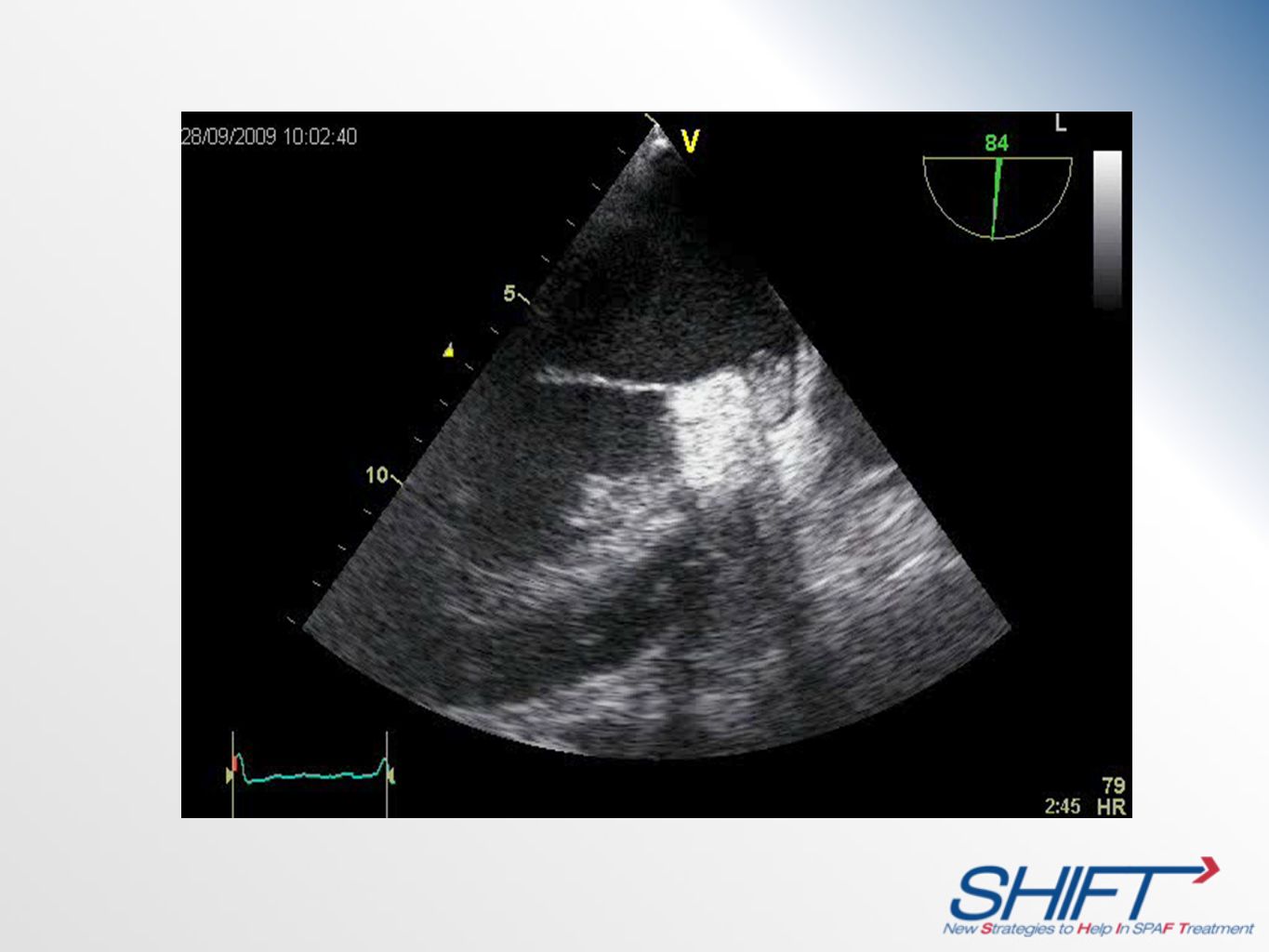
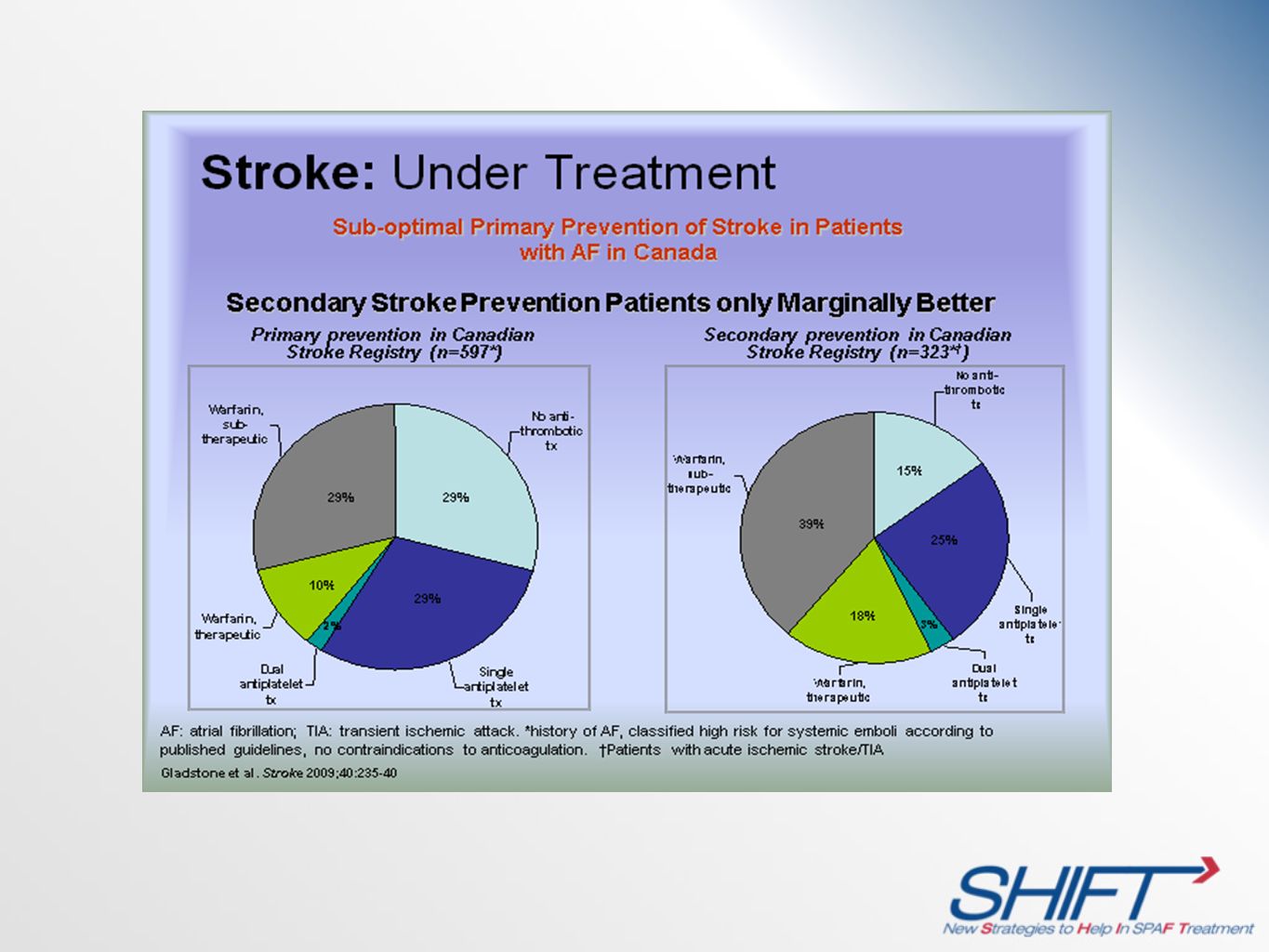




>")














