Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Traitement de la FA Pr JS Hermida

2
Contrôle de fréquence Contrôle de fréquence Contrôle du Rythme
Natural’ time course of AF. The dark blue boxes show a typical sequence of periods in AF against a background of sinus rhythm, and illustrate the progression of AF from silent and undiagnosed to paroxysmal and chronic forms, at times symptomatic. The upper bars indicate therapeutic measures that could be pursued. Light blue boxes indicate therapies that have proven effects on ‘hard outcomes’ in AF, such as stroke or acute heart failure. Red boxes indicate therapies that are currently used for symptom relief, but may in the future contribute to reduction of AF-related complications. Rate control (grey box) is valuable for symptom relief and may improve cardiovascular outcomes.
 is valuable for symptom relief and may improve cardiovascular outcomes.")
3
Contrôle de fréquence Contrôle du Rythme Natural’ time course of AF.
The dark blue boxes show a typical sequence of periods in AF against a background of sinus rhythm, and illustrate the progression of AF from silent and undiagnosed to paroxysmal and chronic forms, at times symptomatic. The upper bars indicate therapeutic measures that could be pursued. Light blue boxes indicate therapies that have proven effects on ‘hard outcomes’ in AF, such as stroke or acute heart failure. Red boxes indicate therapies that are currently used for symptom relief, but may in the future contribute to reduction of AF-related complications. Rate control (grey box) is valuable for symptom relief and may improve cardiovascular outcomes.
 is valuable for symptom relief and may improve cardiovascular outcomes.")
4
Anticoagulants

5
Prévention des accidents thrombo-emboliques
Tt Antithrombotique pour prévenir les accidents TE est recommandé pour tous les patients avec de la FA sauf si FA isolée ou si CI. Classe I IIa IIb III A B C Prévention des accidents thrombo-emboliques survenant lors des FA Il est rappelé que de façon indiscutable (classe I niveau A), tous les patients devaient être sous anticoagulants, sauf contre-indication ou FA isolée.
, tous les patients devaient être sous anticoagulants, sauf contre-indication ou FA isolée.")
6
Anti vitamine K AVC 1.4% 4.5% p<0.001 DC 3.6% 5.4% p<0.001
Réduction du risque absolu Warfarine Placebo AVC 1.4% 4.5% p<0.001 DC % 5.4% p<0.001 Hart RG et al, Ann Intern Med 1999;131:492–501.

7
Anti vitamine K Réduction du risque relatif
-AVC = 62%1 to 68%2 (ischémique+hemorragique) -Décès = 33% -AVC+Embolie systémique+DC = 48% Stroke= ischemic+hemorrhagic (if only ischemic: 65% reduction) AVC hémorragiques = 0.3%/an si AVK VS 0.1% sans AVK (Hart) (diminution NS mortalité avec AVK) 1 Hart RG et al, Ann Intern Med 1999;131:492–501. 2 Atrial Fibrillation Investigators, Arch InternMed.1994; 154: 7
 -Décès = 33% -AVC+Embolie. systémique+DC = 48% Stroke= ischemic+hemorrhagic (if only ischemic: 65% reduction) AVC hémorragiques = 0.3%/an si AVK VS 0.1% sans AVK (Hart) (diminution NS mortalité avec AVK) 1 Hart RG et al, Ann Intern Med 1999;131:492– Atrial Fibrillation Investigators, Arch InternMed.1994; 154:")
8
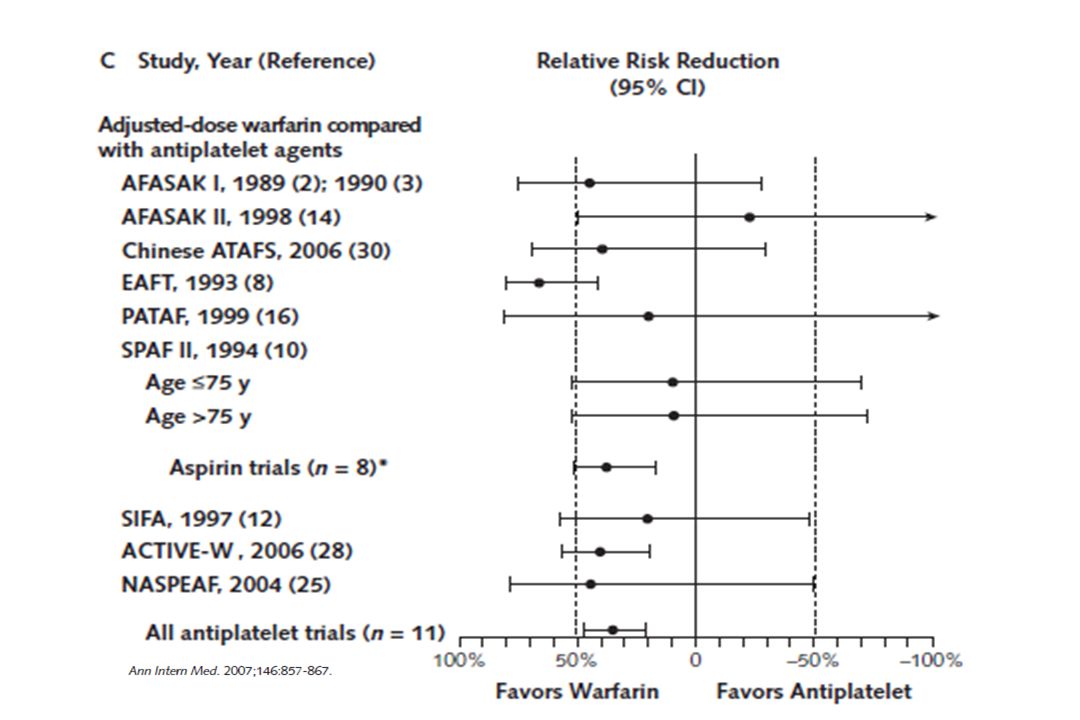
Description: The image to the right shows the results of trials comparing aspirin versus placebo as antithrombotic therapy to reduce stroke in patients with atrial fibrillation. Although all six trials showed trends toward reduced stroke using aspirin, this result was statistically significant only in the SPAF Study (3), which was stopped at an interim analysis due to aspirin’s efficacy. The graphic on the left compares adjusted-dose warfarin versus aspirin. The effect of warfarin on stroke versus aspirin varied widely among these five trials. No statistically significant heterogeneity was seen (p=0.09), and meta-analysis showed that adjusted-dose warfarin reduced overall relative risk for all stroke by 36% (CI, 14% to 52%) compared with aspirin. Horizontal lines are 95% CIs around the point estimates. AFASAK = Copenhagen Atrial Fibrillation, Aspirin, and Anticoagulation Study (I and II); EAFT = European Atrial Fibrillation Trial; ESPS II = European Stroke Prevention Study II; LASAF = Low-Dose Aspirin, Stroke, and Atrial Fibrillation Pilot Study; PATAF = Prevention of Arterial Thromboembolism in Atrial Fibrillation; SPAF = Stroke Prevention in Atrial Fibrillation Study; UK-TIA = United Kingdom TIA Study. Citation: Reproduced with permission from ACP-ASIM. Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysis. Ann Intern Med 1999;131:

10
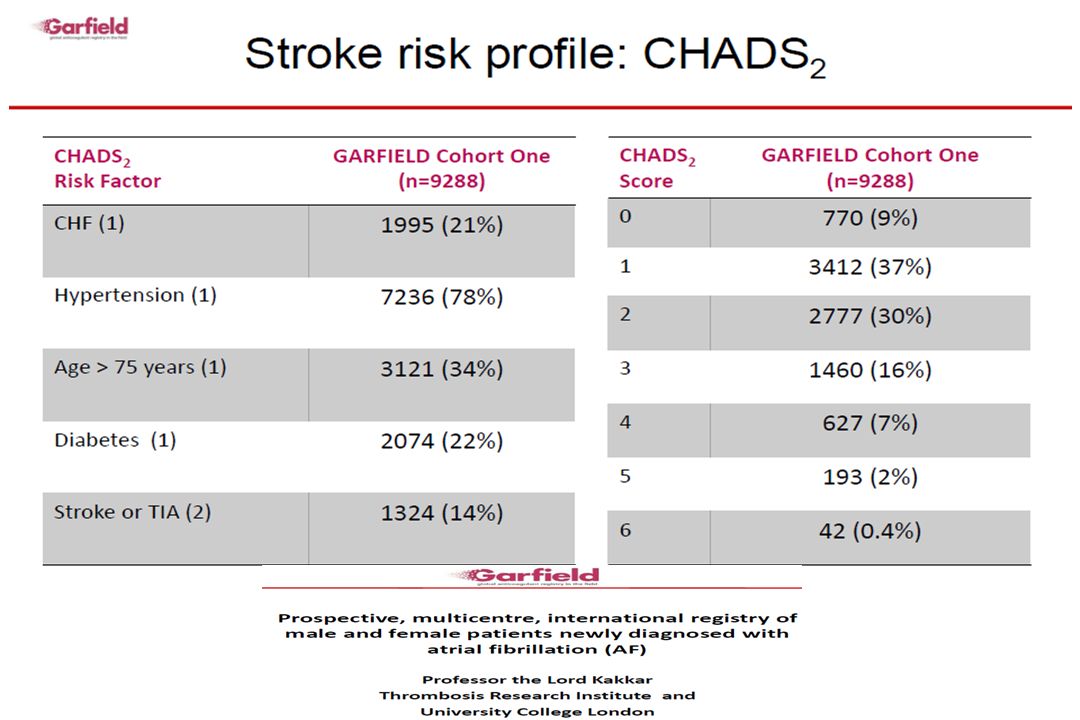
Score CHADS2 (En dehors du RM et des Prothèses Valvulaires)
C – Cardiaque Insuffisance ou baisse FEVG (1pt) H – HTA (1pt) A – Age > 75 (1pt) D – Diabetes (1pt) S2 – Strokes: AIT ou AVC ischémique antérieur (2pts) Faible risque = 0 Risque intermédiaire = 1 Risque élevé = 2 et plus
 H – HTA (1pt) A – Age > 75 (1pt) D – Diabetes (1pt) S2 – Strokes: AIT ou AVC ischémique antérieur (2pts) Faible risque = 0. Risque intermédiaire = 1. Risque élevé = 2 et plus.")
12
FA non valvulaire Rockson SG et al. JACC 2004 Si CHADS2 ≥2: AVK

13
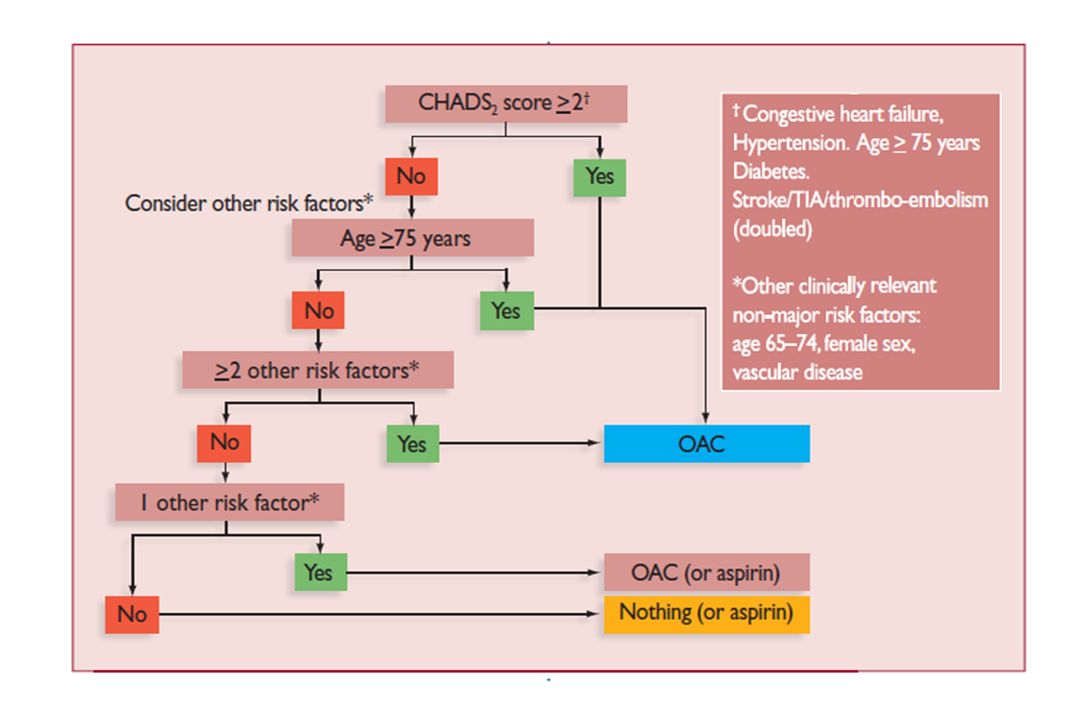
Si CHADS2 = 0 ou 1?

14
Recommandations European Society of Cardiology 2010

15
Recommandations European Society of Cardiology 2010

17
INR cible Pour une FA non rhumatismale un INR cible de 2,5 (entre 2 et 3), Rapport risque-bénéfice optimal (prévention efficace des accidents emboliques et un faible taux d’accidents hémorragiques, environ de 1% par an) Pour des patients à haut risque embolique tels les patients ayant une prothèse valvulaire mécanique, l’INR doit être >2,5
 Pour des patients à haut risque embolique tels les patients ayant une prothèse valvulaire mécanique, l’INR doit être >2,5.")
18
International Normalized Ratio
Risque d’hémorragie intracranienne selon l’intensité de l’anticoagulation 20 15 10 5 1 Odd ratio Accidents ischémiques Hémorragies intracraniennes Prévention des accidents thrombo-emboliques survenant lors des FA Il est rappelé que l'INR doit être compris entre 2 et 3. Un INR supérieur n'apporte pas de bénéfice, mais augmente le risque hémorragique. 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 Fuster V, Ryden LE, Cannom DS et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation Sep;8(9): International Normalized Ratio
: International Normalized Ratio.")
19
Recommandations European Society of Cardiology 2010

20
AVK et cardioversion Le traitement anticoagulant doit être utilisé avant toute cardioversion pharmacologique ou électrique. 2 stratégies sont possibles : 1- AVK durant 3 semaines au moins avant la cardioversion 2- Héparine NF ou HBPM et vérifier par une ETO l’absence de thrombus intracavitaire Après la cardioversion, les AVK doivent être poursuivis pendant au moins 4 semaines, ou plus si le risque de récidive de la FA est jugé important.

21
Recommandations European
Society of Cardiology 2010

22
Conduite à tenir en cas de surdosage asymptomatique
Mesures thérapeutiques permettant de corriger le surdosage INR mesuré et INR cible INR mesuré INR cible 2.5 Fenêtre entre 2 et 3 INR cible ≥ 3 Fenêtre ou 3 - 4,5 INR < 4 Pas de saut de prise Pas de Vit K 4 ≤ INR < 6 Saut d’une prise 6 ≤ INR < 10 Arrêt des AVK 1 à 2 mg Vit K PO Avis Cardio pour discuter Vit K INR ≥ 10 5 mg VIT K PO Avis Spécialisé sans délai ou Hospitalisation ( Prise en charge des surdosages, des situations à risque hémorragique et des accidents hémorragiques chez les patients traités par antivitamines K en ville et en milieu hospitalier (Sang Thromb Vaiss 2008;20(N°spécial) juillet 2008).
 juillet 2008).")
23
Ralentir ou Réduire ? Points d’accords
*Compte tenu de l’efficacité limitée des AA et de leur risque proarythmique, il n’y a pas de supériorité prouvée de la stratégie de maintien du RS par technique pharmacologique (RACE et AFFIRM). MAIS Bénéfice de : -Existence du RS (AFFIRM) -Maintien des AVK si prévention FA paroxystique médicamenteuse
. MAIS Bénéfice de : -Existence du RS (AFFIRM) -Maintien des AVK si prévention FA paroxystique médicamenteuse.")
24
FA: Toujours ralentir (contrôle de fréquence)
FA: Toujours ralentir (contrôle de fréquence). Quand associer un contrôle du rythme? Si le patient reste symptomatique malgré un contrôle adéquate de la fréquence cardiaque Si le patient est jeune ou a un niveau d’activité élevé Si FA paroxystique sans cardiopathie Si FA chronique négligée. “Long lasting persistent AF”
. Quand associer un contrôle du rythme Si le patient reste symptomatique malgré un contrôle adéquate de la fréquence cardiaque. Si le patient est jeune ou a un niveau d’activité élevé. Si FA paroxystique sans cardiopathie. Si FA chronique négligée. Long lasting persistent AF")
25
A-Contrôle du rythme 1-Cardioversion Pharmacologique ou électrique
2-Maintien du RS Antiarythmiques Ablation percutanée Il permet la disparition des symptômes liés à la FA, une amélioration de l’état hémodynamique.

26
1-Cardioversion - Cardioversion pharmacologique
Les AA utilisés appartiennent à la classe I ou III de Vaughan-Williams. Flécaïnide, la propafénone, l’amiodarone IV ou PO CI: IC une altération de la FEVG, une cardiopathie ischémique, BBG. Effets secondaires : transformation de la FA en flutter auriculaire (5 à 10 % des cas) avec une conduction AV 1:1. ; bradycardie.
 avec une conduction AV 1:1. ; bradycardie.")
27
- Cardioversion électrique
CEE synchronisé sur l’onde R. AG brève. Taux de succès : 65 à 90 %. Facteurs de succès: FA récente, petite oreillette G Maintien du RS dépend taille de OG (< 50 mm), l’existence d’une cardiopathie et l’utilisation ou non d’AA Importance d’enregistrer l’ECG après le CEE. *En cas de récidive précoce, cela indique un foyer atrial actif *En l’absence de réduction, il s’agit alors de seuils de défibrillation élevés. Le recours à un choc endocavitaire basse énergie peut se révéler efficace
, l’existence d’une cardiopathie et l’utilisation ou non d’AA. Importance d’enregistrer l’ECG après le CEE. *En cas de récidive précoce, cela indique un foyer atrial actif. *En l’absence de réduction, il s’agit alors de seuils de défibrillation élevés. Le recours à un choc endocavitaire basse énergie peut se révéler efficace.")
28
2-Maintien du RS Les AA sont utilisés en première intention pour prévenir les récidives de FA. Sans AA 75% récidive de la FA. Avec AA, 50%. . En l’absence de cardiopathie AA Ic (Flec, Propafenone, cibenzoline). Sotalol. Si échec: amiodarone ou ablation par catheter Si cardiopathie : Amiodarone ou ablation Si Insuffisance cardiaque : Amiodarone ou ablation Dronedarone : retrait possible
. Sotalol. Si échec: amiodarone ou ablation par catheter. Si cardiopathie : Amiodarone ou ablation. Si Insuffisance cardiaque : Amiodarone ou ablation. Dronedarone : retrait possible.")
29
Patients éligibles à l’ablation percutanée
Recommandations European Society of Cardiology 2010 Figure 12 Choice between ablation and antiarrhythmic drug therapy for patients with and without structural heart disease. Proposed integration of antiarrhythmic drug and catheter ablation for AF in patients with relevant underlying heart disease and for those with no or minimal heart disease, including hypertension (HT) without left ventricular hypertrophy (LVH). †More extensive LA ablation may be needed; *usually PVI is appropriate. AF ¼ atrial fibrillation; CAD ¼ coronary artery disease; CHF ¼ congestive heart failure; HT ¼ hypertension; LVH ¼ left ventricular hypertrophy; NYHA ¼ New York Heart Association; PVI ¼ pulmonary vein isolation. Antiarrhythmic agents are listed in alphabetical order within each treatment box. Please note that left atrium (LA) ablation as first-line therapy (dashed line) is a Class IIb recommendation for patients with paroxysmal AF and no or minimal heart disease, who remain highly symptomatic, despite rate control, and who reject antiarrhythmic drug therapy. Patients éligibles à l’ablation percutanée
 without left ventricular hypertrophy (LVH). †More extensive LA ablation may be needed; *usually. PVI is appropriate. AF ¼ atrial fibrillation; CAD ¼ coronary artery disease; CHF ¼ congestive heart failure; HT ¼ hypertension; LVH ¼ left ventricular. hypertrophy; NYHA ¼ New York Heart Association; PVI ¼ pulmonary vein isolation. Antiarrhythmic agents are listed in alphabetical. order within each treatment box. Please note that left atrium (LA) ablation as first-line therapy (dashed line) is a Class IIb recommendation for. patients with paroxysmal AF and no or minimal heart disease, who remain highly symptomatic, despite rate control, and who reject antiarrhythmic. drug therapy. Patients éligibles à l’ablation percutanée.")
30
AF Efficacy: Maintaining NSR > 6 Months

31
B-Contrôle de la fréquence ventriculaire : Ralentir
Quand? Toujours sauf si patient lent en FA spontanément Contrôler la cadence ventriculaire au repos et à l’effort. On utilise les digitaliques, les BB et les CaB (vérapamil ou diltiazem). Dans les cas difficiles, le recours à l’ablation de la jonction nodohissienne peut se justifier
. Dans les cas difficiles, le recours à l’ablation de la jonction nodohissienne peut se justifier.")
32
ESC 2010

33
Traitements non pharmacologiques
Ablation par radiofréquence ou cryothérapie avec déconnexion des VP. Quand échec du traitement antiarythmique médicamenteux

34
Nav X

35
Autres -Ablation de la jonction AV avec implantation d’un stimulateur cardiaque chez les sujet >75ans - Chirurgie (opération du labyrinthe ou opération d’isolation des veines pulmonaires) seulement si existe une autre indication à une chirurgie à coeur ouvert - Défibrillateur auriculaire abandonné
 seulement si existe une autre indication à une chirurgie à coeur ouvert. - Défibrillateur auriculaire abandonné.")
Présentations similaires
















 1-IEC 2-B Bloquant 3-ARA 2 4-Anti-aldostérone.>")

>")
