Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Quels traitements antithrombosants dans les SCA ?
Journées de l’AFL Beyrouth 11-12 mai 2007 G de Gevigney Hôpital Cardiologique Lyon, France

2
Introduction Aspirine Héparine Clopidogrel HBPM Thrombolytiques
Anti GP2B3A Fondaparinux Bivalirudine

3
Best-of 2004 des valvulopathies
Les acquis dans les SCA ST+ et ST- Best-of 2004 des valvulopathies

4
Acute Coronary Syndromes Without ST Evidence for Aspirin
1.0 2.0 Favors Placebo Favors Aspirin Cairns Lewis Theroux Wallentin Pooled This slide of five randomized trials show there is a 25-30% reduction in the risk of death or MI when comparing aspirin vs placebo in patients presenting with acute coronary syndrome. Relative Risk — Death or MI

5
Relative Risk of Death or MI
Acute Coronary Syndromes without ST Evidence for Heparin Use (UFH + ASA versus ASA) Relative Risk of Death or MI Theroux (n = 243) RISC (n = 399) Cohen (n = 69) Cohen (n = 214) Holdright (n = 185) Gurfinkel (n = 143) Overall (n = 1353) 0.5 1 1.5 2 ASA + UFH Better ASA Better 2.66 6.87 P = 0.06 Oler A, JAMA 1996
 Relative Risk of Death or MI. Theroux (n = 243) RISC (n = 399) Cohen (n = 69) Cohen (n = 214) Holdright (n = 185) Gurfinkel (n = 143) Overall (n = 1353) ASA + UFH Better. ASA Better P = Oler A, JAMA")
6
Clopidogrel Critère de jugement principal tous patients
% de patients présentant un événement ischémique ( décès vasculaire, IDM, AVC) 10 14 12 4 8 6 2 Le bénéfice apparait dès les premières heures et continue de croître à 12 mois 20% RRR p= n=12 562 Slide 5 Résulats d’efficacité / critère de jugement principal 1 Les courbes de Kaplan-Meier commencent à diverger dés les premières heures et continuent à diverger tout au long des 12 mois de suivi PLAVIX, en plus d’un traitement standard comprenant de l’aspirine, apporte donc un bénéfice dés les premières heures de la prise en charge des patients présentant un SCA ( angor instable ou IDM san onde Q) et ce bénéfice sur le risque de récidive ischémique se poursuit à long terme Traitement standard Clopidogrel + traitement standard 1 2 3 4 5 6 7 8 9 10 11 12 Suivi en mois The CURE Investigators. N Eng J Med August 2001 References The CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with non ST elevation acute coronary syndromes. N Eng J Med August 2001. Sanofi-Synthelabo. Data on file.
 Le bénéfice apparait dès les premières heures et continue de croître à 12 mois. 20% RRR. p= n= Slide 5 Résulats d’efficacité / critère de jugement principal 1. Les courbes de Kaplan-Meier commencent à diverger dés les premières heures et continuent à diverger tout au long des 12 mois de suivi. PLAVIX, en plus d’un traitement standard comprenant de l’aspirine, apporte donc un bénéfice dés les premières heures de la prise en charge des patients présentant un SCA ( angor instable ou IDM san onde Q) et ce bénéfice sur le risque de récidive ischémique se poursuit à long terme. Traitement standard. Clopidogrel + traitement standard Suivi en mois. The CURE Investigators. N Eng J Med August References. The CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with non ST elevation acute coronary syndromes. N Eng J Med August Sanofi-Synthelabo. Data on file.")
7
Résultats à long terme de la randomisation à la fin du suivi
PCI- Résultats à long terme de la randomisation à la fin du suivi Cumulative hazard rates 0.15 12.6% 31% RRR p=0.002 n=2658 0.10 8.8% Tt conventionnel Clopidogrel + tt conventionnel 0.05 Slide 36 Résultats à long terme Critère de jugement composé: décès cardiovasculaire, IDM survenant entre la randomisation dans CURE et la fin du suivi Pour le critère de jugement survenu des décès CV ou IDM survenant entre la randomisation dans CURE et la fin du suivi, il existe une diminution du Risque Rerlatif de 31% dans le groupe des patients recevant du Clopidogrel plus un traitement conventionnel par rapport à ceux recevant du placébo ( traitement conventionnel seul) ((8.8% clopidogrel vs. 12.6% placebo, p=0.002). Les courbes divergent très rapidement dés les premièrse heures et continuent à diverger tout au long du suivi de 12 mois. Ceci signifie qu’un traitement par clopidogrel avant une ACP apporte un bénéfice sur la prévention des IDM et des décès cardiovasculaires ( a court et long terme). Le bénéfice se retrouve sur les différents sous groupes de patients. †up to 12 months Critére: IDM + décès vasculaire 0.0 10 40 100 200 300 400 Jours de suivi a b a = délais médian randomisation /ACP (10 jours) b = 30 jours aprés ACP Reference The CURE Trial Investigators. Effect of clopidogrel and aspirin pre-treatment followed by long term therapy in patients undergoing percutaneous coronary intervention: The PCI-CURE Study. Lancet August 2001.
 ((8.8% clopidogrel vs. 12.6% placebo, p=0.002). Les courbes divergent très rapidement dés les premièrse heures et continuent à diverger tout au long du suivi de 12 mois. Ceci signifie qu’un traitement par clopidogrel avant une ACP apporte un bénéfice sur la prévention des IDM et des décès cardiovasculaires ( a court et long terme). Le bénéfice se retrouve sur les différents sous groupes de patients. †up to 12 months. Critére: IDM + décès vasculaire Jours de suivi. a. b. a = délais médian randomisation /ACP (10 jours) b = 30 jours aprés ACP. Reference. The CURE Trial Investigators. Effect of clopidogrel and aspirin pre-treatment followed by long term therapy in patients undergoing percutaneous coronary intervention: The PCI-CURE Study. Lancet August")
8
Les acquis dans les SCA AntiGP-IIB-IIIA SCA ST + échec dans SCA ST -
Thrombolytiques SCA ST + échec dans SCA ST - AntiGP-IIB-IIIA SCA ST -

9
Best-of 2004 des valvulopathies
HBPM Best-of 2004 des valvulopathies

10
HBPM IDM ST+ HNF ENOXAPARINE durant 48H EXTRACT TIMI 25 fibrinolyse
20056 pts fibrinolyse HNF durant 48H ENOXAPARINE Bolus IV puis 1mg/kg SC 2 fois par jour si < 75ans pas bolus et 0.75mg/kg si >75ans durant toute l’hospitalisation randomisée, double aveugle 30 jours Critères 1aires: décès et IDM Critères IIaires : hémorragies majeures Exclusion : choc créat>220 FIBRINOLYSE : streptokinase 20% ENOX < 75 y: 30 mg IV bolus SC 1.0 mg / kg q 12 h (Hosp DC) ≥ 75 y: No bolus SC 0.75 mg / kg q 12 h (Hosp DC) CrCl < 30: 1.0 mg / kg q 24 h UFH 60 U / kg bolus (4000 U) Inf 12 U / kg / h (1000 U / h) Duration: at least 48 h Cont’d at MD discretion Important de dire que durée des 2 anticoagulations différente Antmann EM NEJM
 ≥ 75 y: No bolus SC 0.75 mg / kg q 12 h (Hosp DC) CrCl < 30: 1.0 mg / kg q 24 h. UFH 60 U / kg bolus (4000 U) Inf 12 U / kg / h (1000 U / h) Duration: at least 48 h Cont’d at MD discretion. Important de dire que durée des 2 anticoagulations différente. Antmann EM NEJM")
11
ST + : Primary End Point Death or Nonfatal MI
UFH 12.0% (1223) 206 events 9.9% (1017) Primary End Point (%) ENOX 5.2% We examined the treatment benefit of enoxaparin on the primary end point over time. As depicted in the horizontal bars UFH was given for a median of 2 days And Enox for a median of 7 days At 48 hours (when there was a direct pharmacologic comparison of the drugs) there already was a trend in favor of enoxaparin with a reduction in the event rate from 5.2 % with UFH to 4.7% with enox. The difference then widened and through 30 days a total of 206 fewer primary end point events occurred in the enox group. Relative Risk 0.83 (0.77 to 0.90) P<0.0001 4.7% RR (0.80 to 1.01) P=0.08 UFH ENOX Days
 206 events. 9.9% (1017) Primary End Point (%) ENOX. 5.2% We examined the treatment benefit of enoxaparin on the primary end point over time. As depicted in the horizontal bars UFH was given for a median of 2 days. And Enox for a median of 7 days. At 48 hours (when there was a direct pharmacologic comparison of the drugs) there already was a trend in favor of enoxaparin with a reduction in the event rate from 5.2 % with UFH to 4.7% with enox. The difference then widened and through 30 days a total of 206 fewer primary end point events occurred in the enox group. Relative Risk 0.83 (0.77 to 0.90) P< % RR 0.90 (0.80 to 1.01) P=0.08. UFH. ENOX. Days.")
12
Bleeding Endpoints (TIMI) 30 Days
UFH ENOX ARD 0.7% RR 1.53 P<0.0001 ARD 0.4% RR 1.39 P = 0.014 ARD 0.1% RR 1.27 P = 0.14 % Events The major bleeding rates observed in both groups were lower than those reported in prior trials , probably as a result of the conservative dosing strategies we used. The major bleeding rate was 2.1% with Enox and 1.4% with UFH-- a 0.7% ARI and RRI of 1.53 that was associated with a P value < There was no difference in the rate of fatal major bleeds , which occurred in about 35% of both groups. The rates of nonfatal major bleeds, shown here were 0.9% with Enox and 1.3 % with UFH—a 0.4% ARI with P=0.014 There was no significant difference in ICH that occurred in 0.8% of Enox and 0.7% of UFH patients. Major Bleed (fatal + nonfatal) Nonfatal Major Bleed ICH
 Nonfatal Major Bleed. ICH.")
13
Méta analyse HBPM vs HNF: ST+ thrombolysé
Eikelboom JW et Al Circulation 2005

14
Méta analyse HBPM vs HNF ST+ thrombolysé
Outcomes during hospitalization/at 7 days with LMWH vs UFH End point LMWH UFH Odds ratio 95% CI Reinfarction (%) 3.0 5.2 0.57 Death (%) 4.8 5.3 0.92 Major bleeding (%) 3.3 2.5 1.30 Minor bleeding (%) 22.8 19.4 1.26 Eikelboom JW et Al Circulation 2005
 Death (%) Major bleeding (%) Minor bleeding (%) Eikelboom JW et Al Circulation")
15
HBPM SCA ST- décès ou infarctus à 30 jours
saignements majeurs : pas de différence significative Elkelboom Lancet 2000; 355: 1936

16
HBPM SCA ST- SYNERGY Décès et IDM à 30 jours
9978 patients SCA ST- randomisés HNF vs enoxaparine avec 92% patients coronarographiés Décès et IDM à 30 jours 5 10 15 20 25 30 0.8 0.85 0.9 0.95 1.0 % patients sans décès ni IDM Jours après randomisation UFH Enoxaparin Synergy JAMA 2005 Pour l’ATL les HBPM ne sont pas considérés aussi fiable que hnf ds reco de 2005 Hnf -60IU/kgvs 1MG/KG/12H Pas de différence significative Ferguson J JAMA :45-54

17
Efficacy and Safety Outcomes With Consistent Therapy (Including Crossovers)
[SYNERGY/R/52] [SYNERGY/S/52] HR [95%] 0.82 [ ] 18% RRR Patients (%) In the population of 6,138 patients receiving consistent therapy, the primary composite efficacy endpoint of 30-day death and MI occurred in 13.3% of LOVENOX®-treated patients vs 15.9% of UFH-treated patients. Statistical analysis showed a hazard ratio of 0.82 (95% CI ) favoring LOVENOX®, which indicates that patients who were treated with LOVENOX® had only 0.82 of the risk of experiencing death or MI at 30 days compared to patients treated with UFH. There was therefore an RRR of 18% in favor of LOVENOX® UFH ENOX HR=hazard ratio. SYNERGY Trial Investigators. JAMA. 2004;292:45-54.
 In the population of 6,138 patients receiving consistent therapy, the primary composite efficacy endpoint of 30-day death and MI occurred in 13.3% of LOVENOX®-treated patients vs 15.9% of UFH-treated patients. Statistical analysis showed a hazard ratio of 0.82 (95% CI ) favoring LOVENOX®, which indicates that patients who were treated with LOVENOX® had only 0.82 of the risk of experiencing death or MI at 30 days compared to patients treated with UFH. There was therefore an RRR of 18% in favor of LOVENOX® UFH. ENOX. HR=hazard ratio. SYNERGY Trial Investigators. JAMA. 2004;292:")
18
HBPM SCA ST- SYNERGY Enoxaparin UFH (n = 4993) (n = 4985) P-value
Complications hémorragiques Enoxaparin UFH (n = 4993) (n = 4985) P-value GUSTO severe TIMI major - clinical: CABG-related Non-CABG-related H/H drop - algorithm Any RBC transfusion ICH < 0.1 < 0.1 NS Ferguson J JAMA :45-54
 (n = 4985) P-value. GUSTO severe TIMI major - clinical: CABG-related Non-CABG-related H/H drop - algorithm Any RBC transfusion ICH < 0.1 < 0.1 NS. Ferguson J JAMA :")
19
HBPM Chez patients avec SCA ST- HBPM au moins aussi efficace qu’HNF; avantages : . administration SC . pas surveillance coagulation . meilleure prédictibilité et stabilité traitement Chez Patients avec IDM ST+ avant 75 ans utilisation possible

20
Best-of 2004 des valvulopathies
AntiGP IIB III A Best-of 2004 des valvulopathies

22
Best-of 2004 des valvulopathies
Fondaparinux Best-of 2004 des valvulopathies

23
Agents anti Xa exclusifs
Anticoagulants Rappels Voie extrinsèque (facteur tissulaire) Voie intrinsèque XIIa VIIa XIa Héparine / HBPM AT-III dépendant) IXa Hirudine/Hirulog bivalirudine Antithrombine exclusifs Activités inhibitrices HNF équvalentes sur thrombine et facteur Xa Xa polysaccharides fondaparinux Agents anti Xa exclusifs Thrombine (IIa) Thrombine-Fibrine
 Voie intrinsèque. XIIa. VIIa. XIa. Héparine / HBPM AT-III dépendant) IXa. Hirudine/Hirulog. bivalirudine. Antithrombine exclusifs. Activités inhibitrices HNF équvalentes sur thrombine et facteur Xa. Xa. polysaccharides. fondaparinux. Agents anti Xa exclusifs. Thrombine (IIa) Thrombine-Fibrine.")
24
Anti-Xa Fondaparinux pentasaccharide synthétique
élimination rénale demi-vie d’élimination 17-21H contre-indication : insuffisance rénale sévère pas de cas de thrombopénie induite décrite pas de surveillance numération plaquettaire Demi-vie permet une inj/jour Clairance inferieur à 30mL/min contre indication Dose 7,5mg/jour entre 50 et 100kg, 5mg en dessous de 50kg, 10mg/jour au dessus de 100kg

29
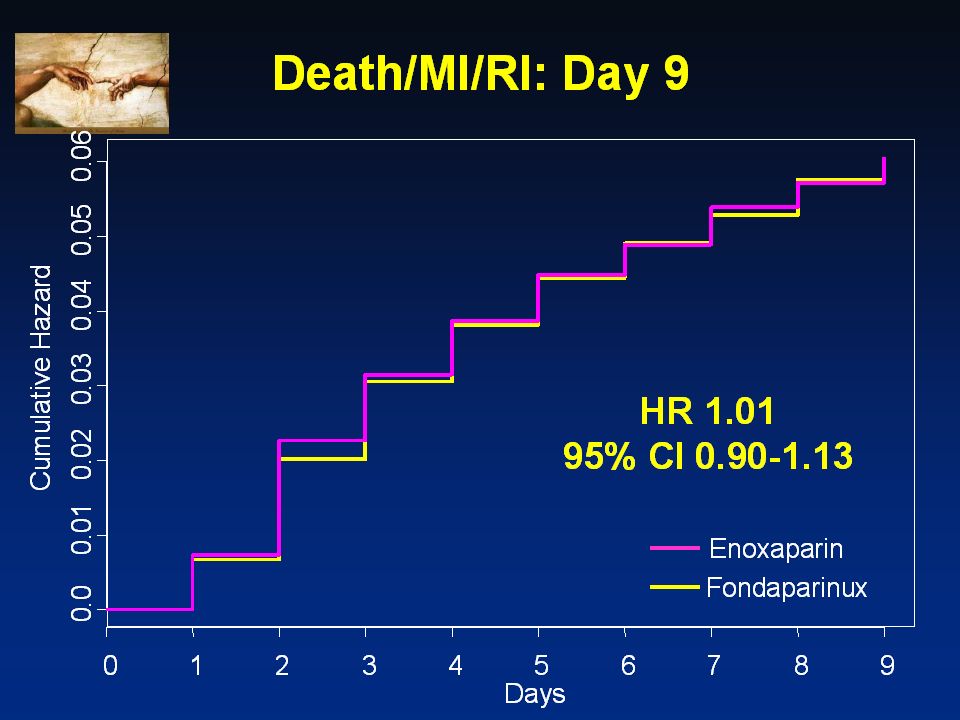
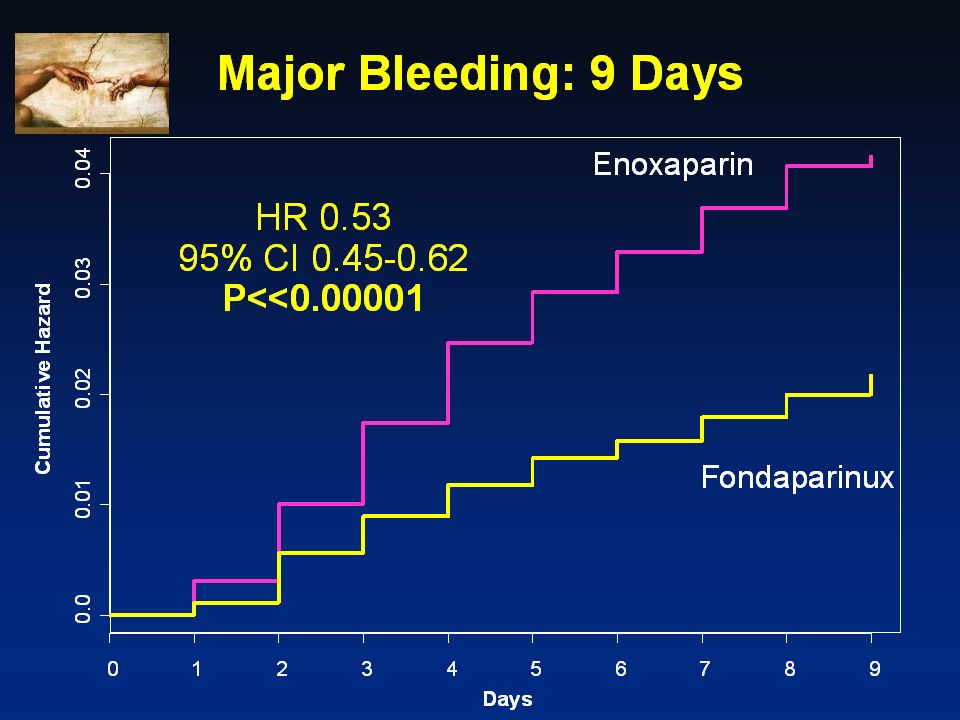
Fondaparinux efficacité similaire fondaparinux/enoxaparine
CONCLUSION OASIS 5 efficacité similaire fondaparinux/enoxaparine réduction hémorragies avec fondaparinux entrainant diminution mortalité limites : seulement 60% patients coronarographiés, 33% population a eu une ATL groupe enoxaparine a reçu HNF pour angioplastie 65% patients sous clopidogrel lors angioplastie cas thrombus dans cathéter 50% patients ont eu ATL avec HNF Serait à réserver aux patients traiter avec traitement conservateur sans coronarographie YUSUF S NEJM

30
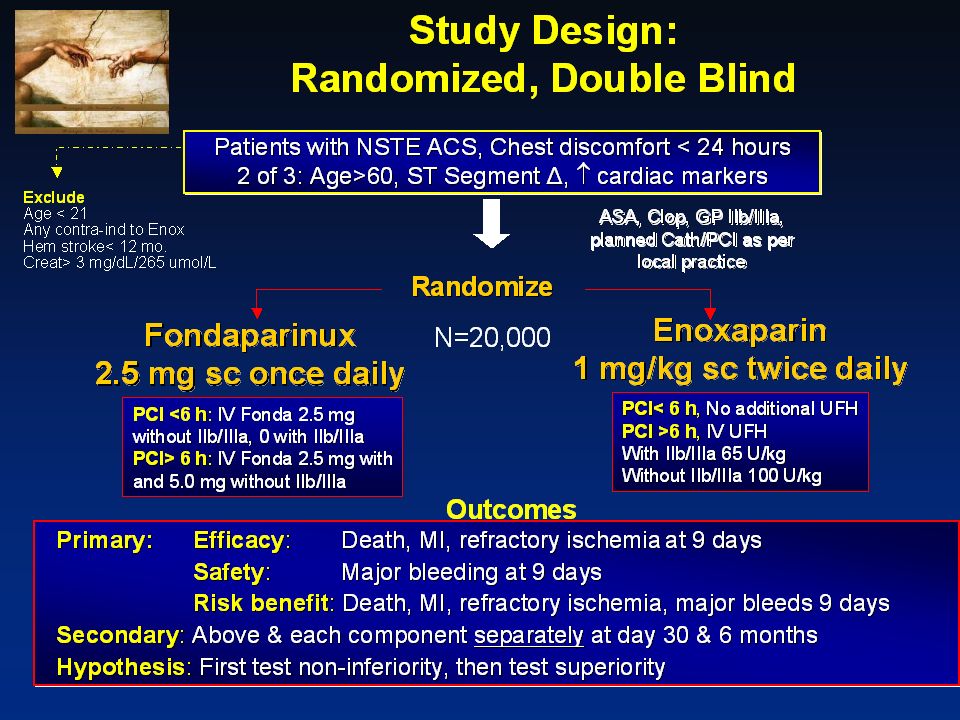
OASIS 6: Randomized, Double Blind, Double Dummy
12,000 Patients with STEMI < 12 h of symptom onset Inclusion: ST 2 mm prec leads or 1 mm limb leads Exclusion: Contra-ind. for anticoagulant, INR>1.8, pregnancy, ICH<12 mo. Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late) Stratification In the ISAR-REACT study, patients (N=2,159, mean age 66 years) received 600 mg clopidogrel at least 2 hours before a PCI procedure with aspirin and a heparin bolus of 70 U/kg. They were then randomized to either abciximab (bolus 0.25 mg/kg, infusion mg/kg/min for 12 hours) or a placebo infusion. Thereafter, all patients received clopidogrel 75 mg twice daily until discharge and then 75 mg clopidogrel daily for at least 4 weeks along with aspirin (100 mg/d). All patients had symptomatic coronary artery disease, but patients with acute coronary syndromes and other patients considered to be at high risk were excluded.* *High-risk exclusion criteria: acute coronary syndromes; acute myocardial infarction within 14 days, ST-segment depression, positive biomarkers, insulin-dependent diabetes, chronic total occlusions, ejection fraction 30%, thrombus and lesions in bypass grafts. Schömig A, Mehilli J, Dotzer F, et al. ISAR-REACT: glycoprotein IIb/IIIa inhibition with abciximab in patients undergoing coronary stenting after pretreatment with a high loading dose of clopidogrel: a multicenter, randomized, double blind, placebo-controlled trial. Presented at: 52nd Annual Scientific Session of the American College of Cardiology; March 30-April 2, 2003; Chicago, Ill. UFH not indicated UFH indicated Randomization Randomization Fondaparinux 2.5 mg Placebo Fondaparinux 2.5 mg UFH
, Primary PCI or no reperfusion (eg. late) Stratification. In the ISAR-REACT study, patients (N=2,159, mean age 66 years) received 600 mg clopidogrel at least 2 hours before a PCI procedure with aspirin and a heparin bolus of 70 U/kg. They were then randomized to either abciximab (bolus 0.25 mg/kg, infusion mg/kg/min for 12 hours) or a placebo infusion. Thereafter, all patients received clopidogrel 75 mg twice daily until discharge and then 75 mg clopidogrel daily for at least 4 weeks along with aspirin (100 mg/d). All patients had symptomatic coronary artery disease, but patients with acute coronary syndromes and other patients considered to be at high risk were excluded.* *High-risk exclusion criteria: acute coronary syndromes; acute myocardial infarction within 14 days, ST-segment depression, positive biomarkers, insulin-dependent diabetes, chronic total occlusions, ejection fraction 30%, thrombus and lesions in bypass grafts. Schömig A, Mehilli J, Dotzer F, et al. ISAR-REACT: glycoprotein IIb/IIIa inhibition with abciximab in patients undergoing coronary stenting after pretreatment with a high loading dose of clopidogrel: a multicenter, randomized, double blind, placebo-controlled trial. Presented at: 52nd Annual Scientific Session of the American College of Cardiology; March 30-April 2, 2003; Chicago, Ill. UFH not indicated. UFH indicated. Randomization. Randomization. Fondaparinux. 2.5 mg. Placebo. Fondaparinux. 2.5 mg. UFH.")
31
Primary Efficacy Outcome Death/MI at 30 Days
0.12 UFH/Placebo 0.10 Fondaparinux 0.08 0.06 Cumulative Hazard HR 0.86 95% CI P = 0.008 0.04 0.02 0.0 3 6 9 12 15 18 21 24 27 30 Days

32
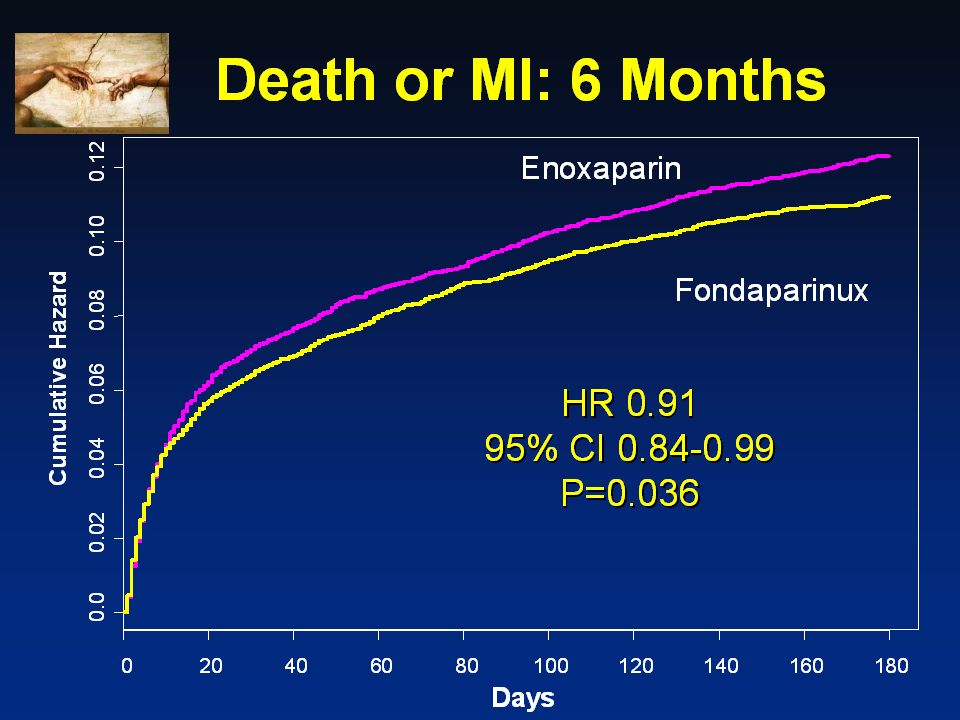
Death at Study End (3 or 6 months)
0.12 UFH/Placebo 0.10 Fondaparinux 0.08 0.06 Cumulative Hazard HR 0.88 95% CI P = 0.029 0.04 0.02 0.0 18 36 54 72 90 108 126 144 162 180 Days

33
Severe hemorrhage at 30 days

34
Fondaparinux OASIS 6 randomisation complexe
fondaparinux pas supérieure à l’HNF plus complications lors angioplastie groupe fondaparinux intérêt fondaparinux si pas de revascularisation par angioplastie envisagée YUSUF S JAMA

35
Best-of 2004 des valvulopathies
Bivalirudine Best-of 2004 des valvulopathies

36
Agents anti Xa exclusifs
Anticoagulants Rappels Voie extrinsèque (facteur tissulaire) Voie intrinsèque XIIa VIIa XIa Héparine / HBPM AT-III dépendant) IXa Hirudine/Hirulog bivalirudine Antithrombine exclusifs Activités inhibitrices HNF équvalentes sur thrombine et facteur Xa Xa polysaccharides fondaparinux Agents anti Xa exclusifs Thrombine (IIa) Thrombine-Fibrine
 Voie intrinsèque. XIIa. VIIa. XIa. Héparine / HBPM AT-III dépendant) IXa. Hirudine/Hirulog. bivalirudine. Antithrombine exclusifs. Activités inhibitrices HNF équvalentes sur thrombine et facteur Xa. Xa. polysaccharides. fondaparinux. Agents anti Xa exclusifs. Thrombine (IIa) Thrombine-Fibrine.")
37
Study Design – First Randomization
Moderate and high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819) UFH/Enox + GP IIb/IIIa (n=4,603) Bivalirudin (n=4,604) Alone (n=4,612) R* Angiography within 72h Medical management PCI CABG 33% Moderate and high risk ACS (n=13,819) 56% Aspirin in all Clopidogrel dosing and timing per local practice 11% *Stratified by pre-angiography thienopyridine use or administration 37
 UFH/Enox. + GP IIb/IIIa. (n=4,603) Bivalirudin. (n=4,604) Alone. (n=4,612) R* Angiography within 72h. Medical. management. PCI. CABG. 33% Moderate. and high. risk ACS. (n=13,819) 56% Aspirin in all. Clopidogrel. dosing and timing. per local practice. 11% *Stratified by pre-angiography thienopyridine use or administration. 37.")
38
Study Design – Second Randomization
Moderate and high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819) UFH/Enox + GP IIb/IIIa (N=4,603) Bivalirudin (N=4,604) Alone (N=4,612) R* GPI upstream (N=2294) GPI CCL for PCI (N=2309) GPI upstream (N=2311) GPI CCL for PCI (N=2293) Moderate and high risk ACS (n=13,819 Aspirin in all Clopidogrel dosing and timing per local practice *Stratified by pre-angiography thienopyridine use or administration 38
 UFH/Enox. + GP IIb/IIIa. (N=4,603) Bivalirudin. (N=4,604) Alone. (N=4,612) R* GPI upstream (N=2294) GPI CCL for PCI (N=2309) GPI upstream (N=2311) GPI CCL for PCI (N=2293) Moderate. and high. risk ACS. (n=13,819. Aspirin in all. Clopidogrel. dosing and timing. per local practice. *Stratified by pre-angiography thienopyridine use or administration. 38.")
39
Ischemic Composite Endpoint (Death, MI, unplanned revascularization for ischemia)
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone 25 Estimate P (log rank) 30 day 7.4% 0.36 7.8% 0.34 7.9% — Estimate P (log rank) 16.3% 0.38 16.5% 0.31 16.4% 1 year — 20 UFH/Enoxaparin + IIb/IIIa Bivalirudin + IIb/IIIa Bivalirudin alone p=0.55 15 Ischemic Composite (%) 10 Bivalirudin+GPI vs. Hep+GPI HR [95% CI] = 1.05 ( ) 5 Bivalirudin alone vs. Hep+GPI HR [95% CI] = 1.05 ( ) 30 60 90 120 150 180 210 240 270 300 330 360 390 Days from Randomization
 30 day. 7.4% % % — Estimate. P. (log rank) 16.3% % % 1 year. — 20. UFH/Enoxaparin + IIb/IIIa. Bivalirudin + IIb/IIIa. Bivalirudin alone. p= Ischemic Composite (%) 10. Bivalirudin+GPI vs. Hep+GPI. HR [95% CI] = 1.05 ( ) 5. Bivalirudin alone vs. Hep+GPI. HR [95% CI] = 1.05 ( ) Days from Randomization.")
40
Myocardial Infarction
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone 15 30 day P (log rank) 1 year P (log rank) Estimate Estimate UFH/Enoxaparin + IIb/IIIa Bivalirudin + IIb/IIIa Bivalirudin alone 4.4% — 6.2% — 10 4.6% 0.69 6.4% 0.63 4.8% 0.36 7.1% 0.10 MI (%) p=0.24 5 30 60 90 120 150 180 210 240 270 300 330 360 390 Days from Randomization
 1 year. P. (log rank) Estimate. Estimate. UFH/Enoxaparin + IIb/IIIa. Bivalirudin + IIb/IIIa. Bivalirudin alone. 4.4% — 6.2% — % % % % MI (%) p= Days from Randomization.")
41
Mortality: 524 total deaths at 1-year
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone 5 Bivalirudin+GPI vs. Hep+GPI HR [95% CI] = 0.99 ( ) p=0.90 4 Bivalirudin alone vs. Hep+GPI HR [95% CI] = 0.95 ( ) 3 Mortality (%) 2 Estimate P (log rank) 1.4% 0.53 1.6% 0.39 — 30 day Estimate P (log rank) 4.4% 0.93 4.2% 0.66 3.8% 1 year — 1 UFH/Enoxaparin + IIb/IIIa Bivalirudin + IIb/IIIa Bivalirudin alone 30 60 90 120 150 180 210 240 270 300 330 360 390 Days from Randomization
 p= Bivalirudin alone vs. Hep+GPI. HR [95% CI] = 0.95 ( ) 3. Mortality (%) 2. Estimate. P. (log rank) 1.4% % — 30 day. Estimate. P. (log rank) 4.4% % % 1 year. — 1. UFH/Enoxaparin + IIb/IIIa. Bivalirudin + IIb/IIIa. Bivalirudin alone Days from Randomization.")
42
Days from Randomization
Impact of MI and Major Bleeding (non-CABG) in the First 30 Days on Risk of Death Over 1 Year 1 year Estimate 28.9% Both MI and Major Bleed (N=94) Major Bleed only (without MI) (N=551) 12.5% MI only (without Major Bleed) (N=611) 8.6% 30 3.4% No MI or Major Bleed (N=12,557) 28.9% 25 20 Mortality (%) 15 12.5% 10 8.6% 5 3.4% 30 60 90 120 150 180 210 240 270 300 330 360 390 Days from Randomization
 in the First 30 Days on Risk of Death Over 1 Year. 1 year Estimate. 28.9% Both MI and Major Bleed (N=94) Major Bleed only (without MI) (N=551) 12.5% MI only (without Major Bleed) (N=611) 8.6% % No MI or Major Bleed (N=12,557) 28.9% Mortality (%) % % % Days from Randomization.")
43
Conclusions In patients with moderate and high risk ACS undergoing an early invasive strategy with the use of GP IIb/IIIa inhibitors Bivalirudin is an acceptable substitute for either unfractionated heparin or enoxaparin Compared to either UFH/enoxaparin with GP IIb/IIIa inhibitors or bivalirudin with GP IIb/IIIa inhibitors A bivalirudin alone strategy results in marked reduction of bleeding at 30 days, and similar rates of mortality and composite ischemia at 1-year The results of this study further establish the important relationship between iatrogenic bleeding complications and subsequent mortality in patients with ACS

44
Recommandations actuelles
Maladie coronarienne IDM ST+ ACC ESC SCA ST- HNF 1C B 1A B HBPM 2B 1A A HBPM préférée à 2A A Complications coro: no reflow, dissecion, nouveau thrombus, perforation si enoxaparine

45
Conclusions pas de recommendations par rapport fondaparinux et bivalirudine important de prendre en compte le risque hémorragique Dire HNF n’est pas recommandé pares ATL car augmente juste risque hémorragique

46
Best-of 2004 des valvulopathies
CONCLUSIONS Best-of 2004 des valvulopathies

47
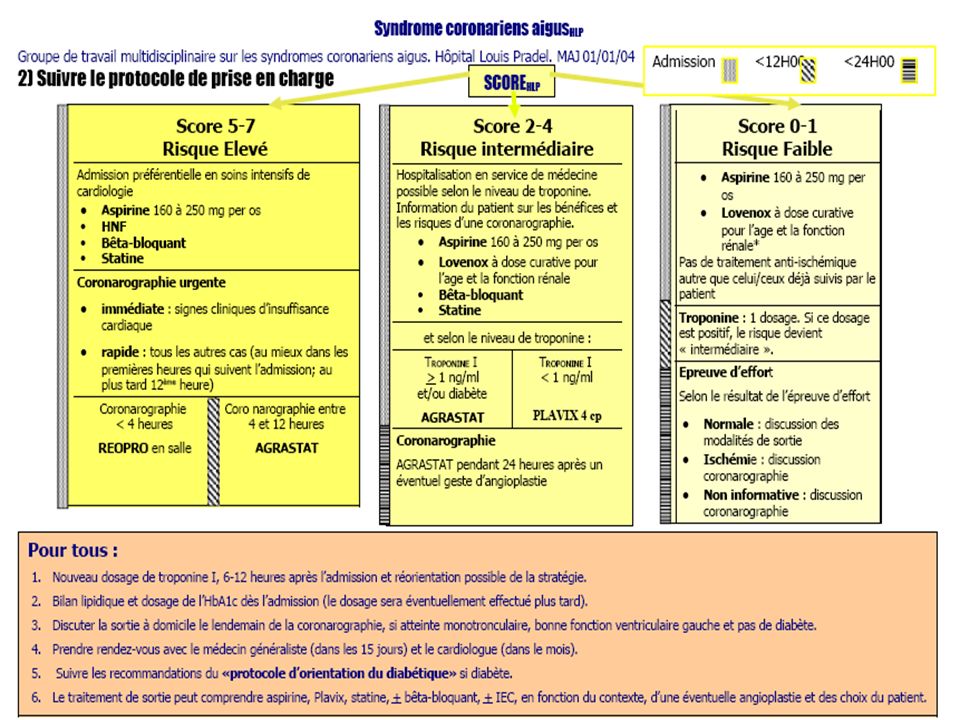
Prise en charge des SCA sans élévation du segment ST

Présentations similaires











 (n=483) Control12.011.2 Abciximab4.65.8 P value0.0050.038 n 6-month.>")







