Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Stéfanie SERRE Service de Réanimation-CHU NICE DES de cardiologie 2iéme année DESC de réanimation médicale Grenoble 2006 Mehta SR et al

2
- angor instable /syndrome de menace - Idm sous endocardique/Idm non Q (NSTEMI) prise en charge des syndromes coronariens aigus sans sus décalage du segment ST Stratégie invasive ou conservatrice? Stratégie invasive: « routine invasive strategy » réalisation précoce d’une coronarographie +/- revascularisation (angioplastie / pontage) Stratégie conservatrice: « selective invasive strategy » traitement médical Coronarographie +/- revascularisation envisagées que si récidive ischémique
 Stratégie conservatrice: « selective invasive strategy » traitement médical Coronarographie +/- revascularisation envisagées que si récidive ischémique.")
3
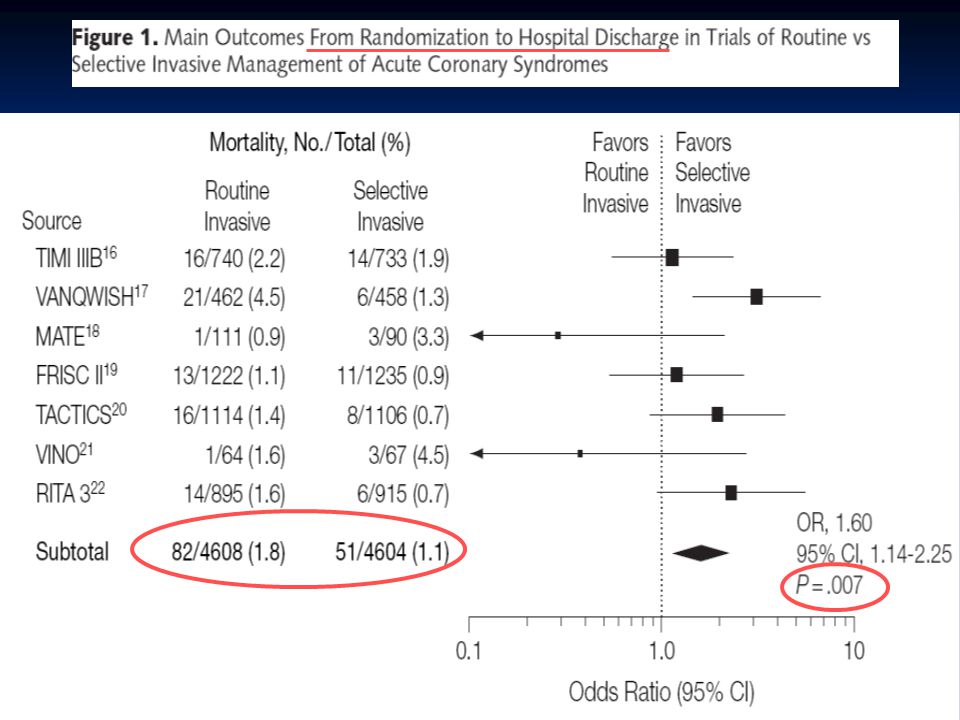
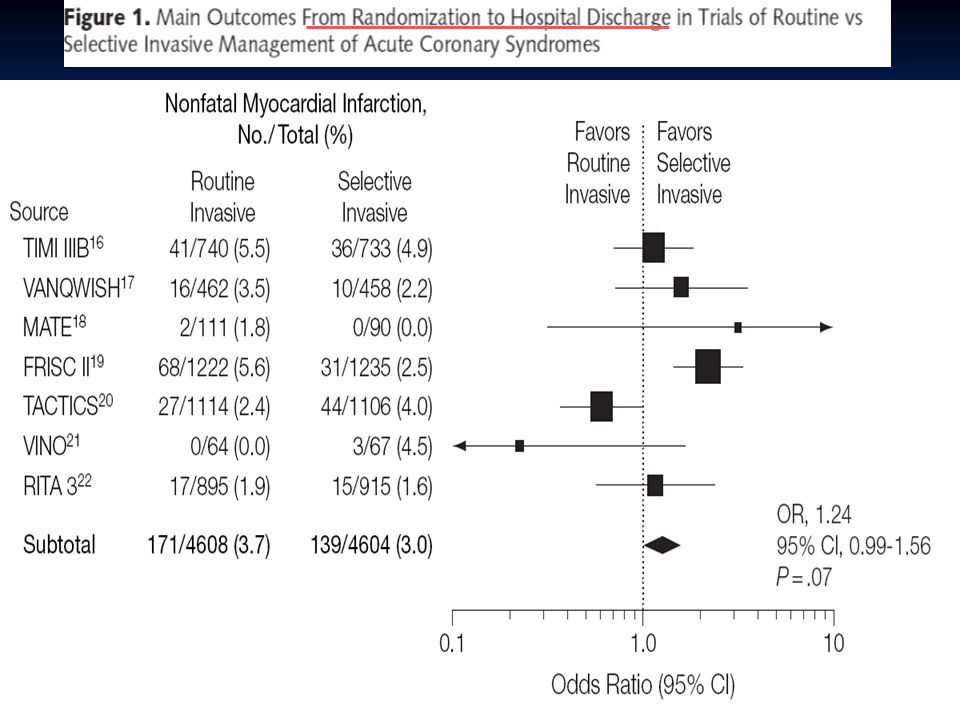
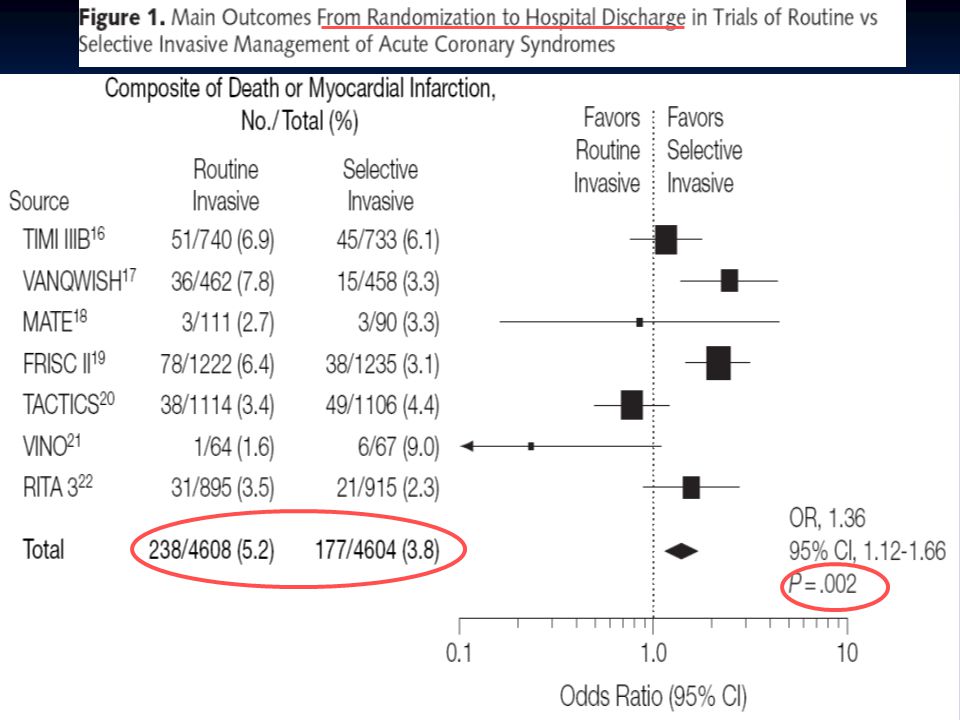
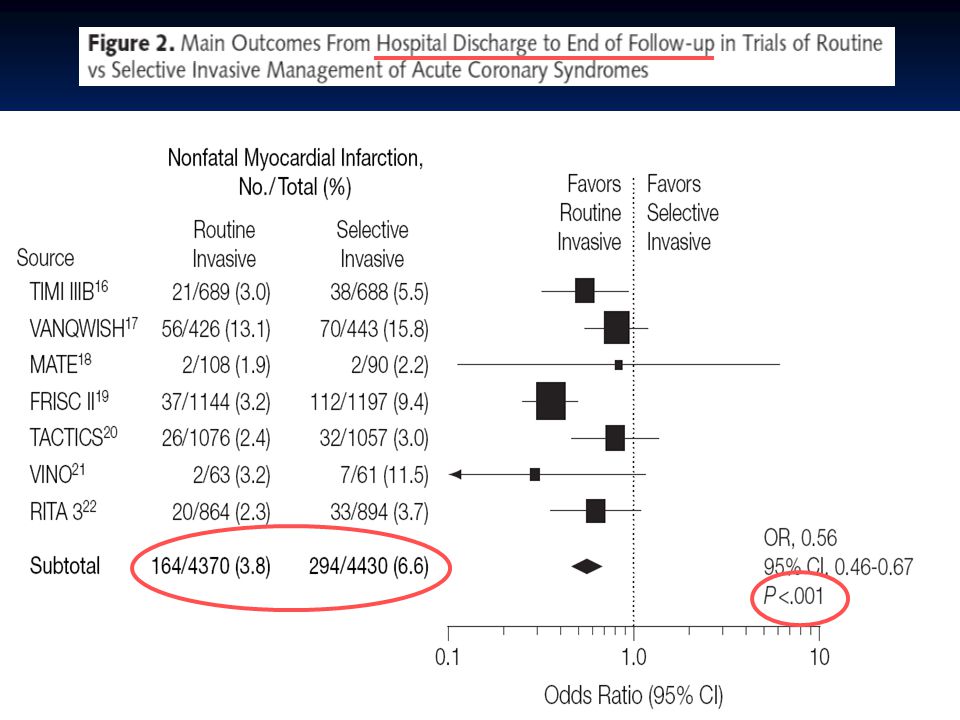
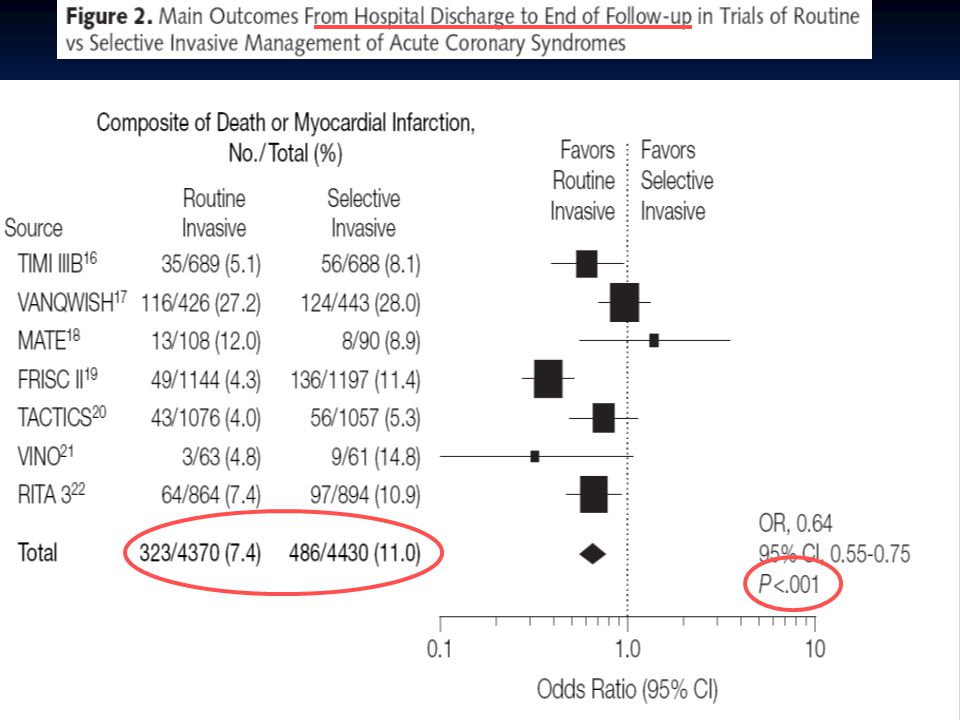
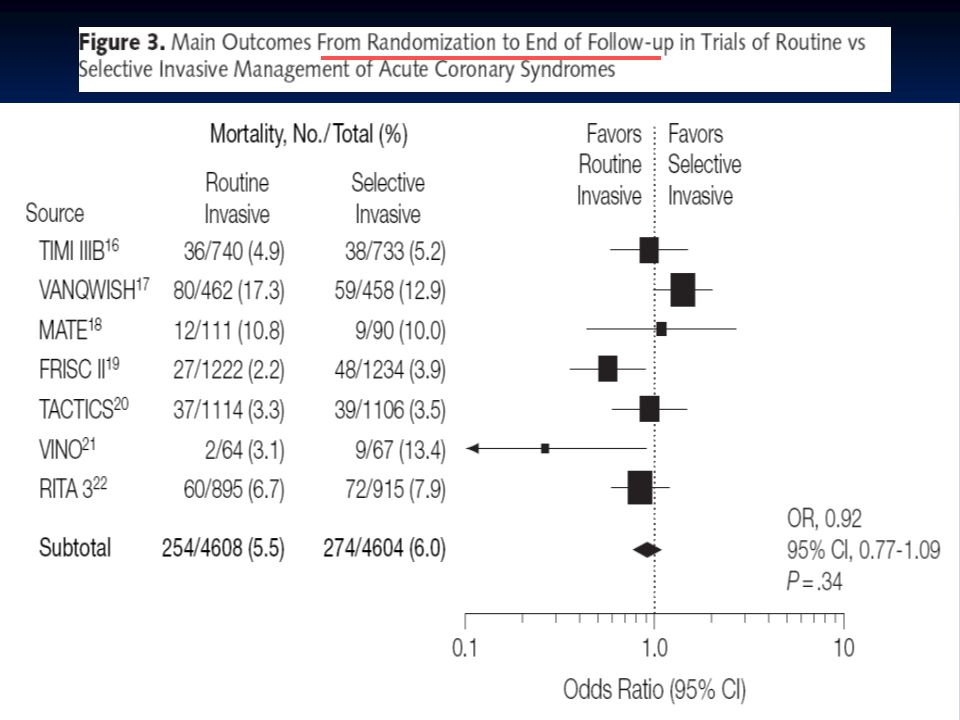
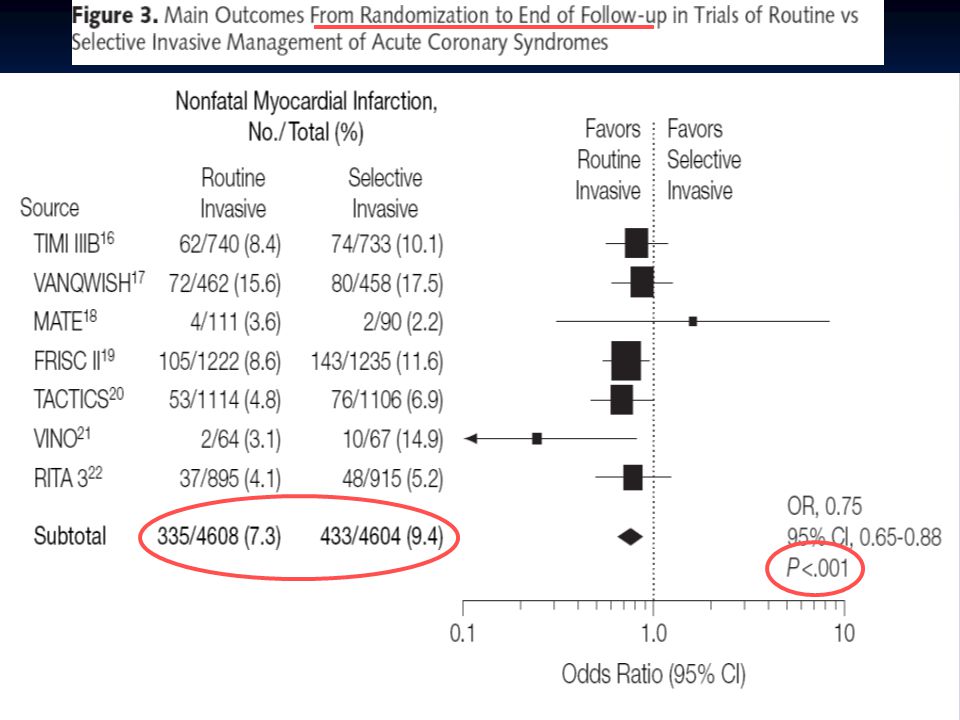
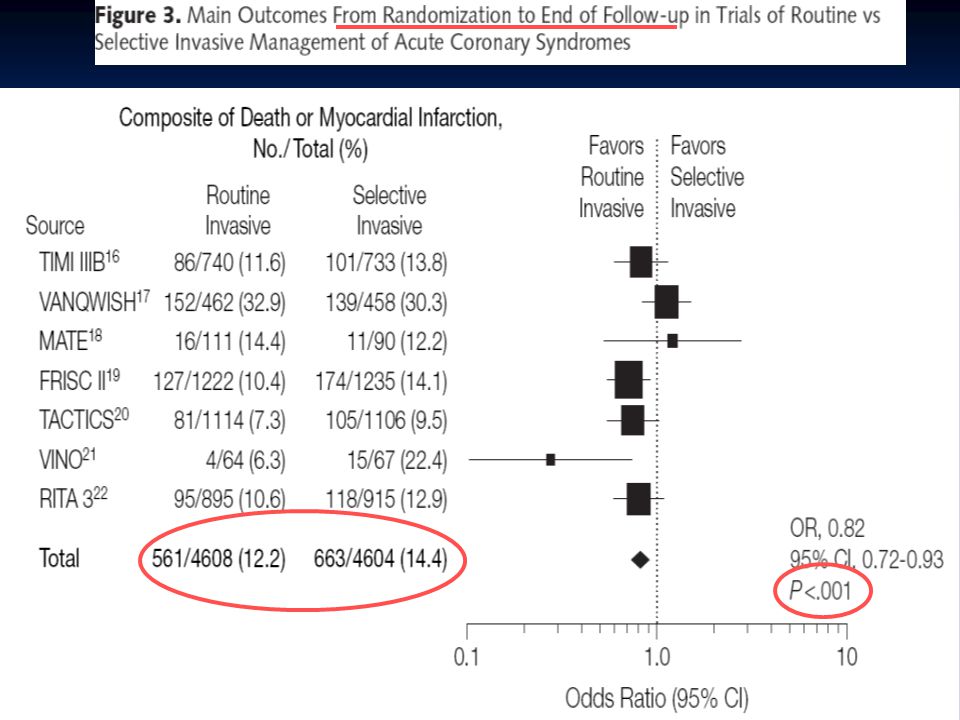
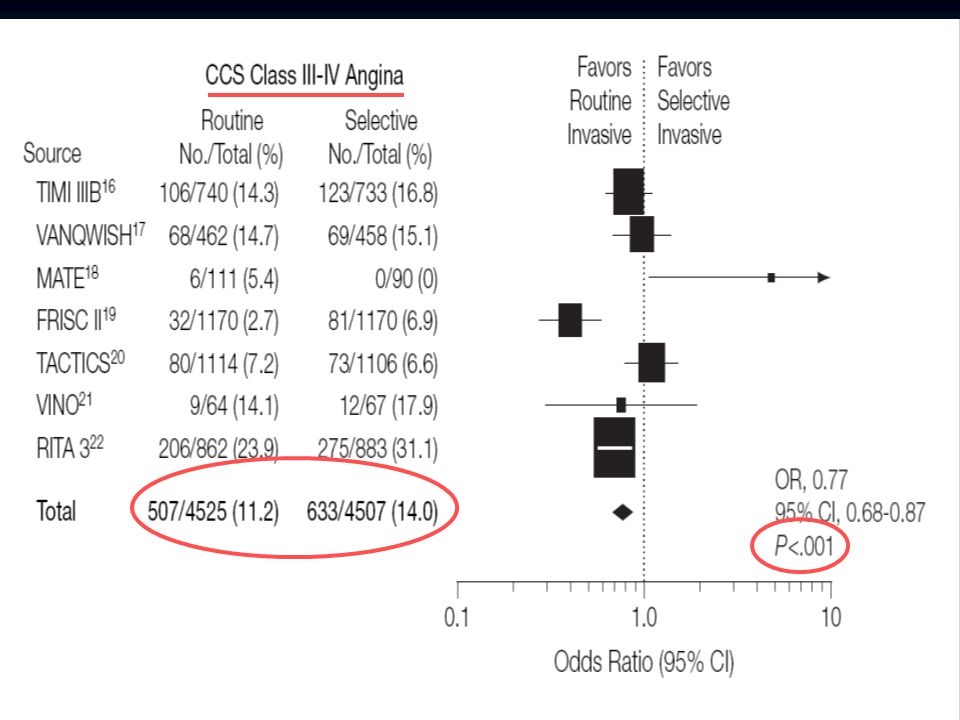
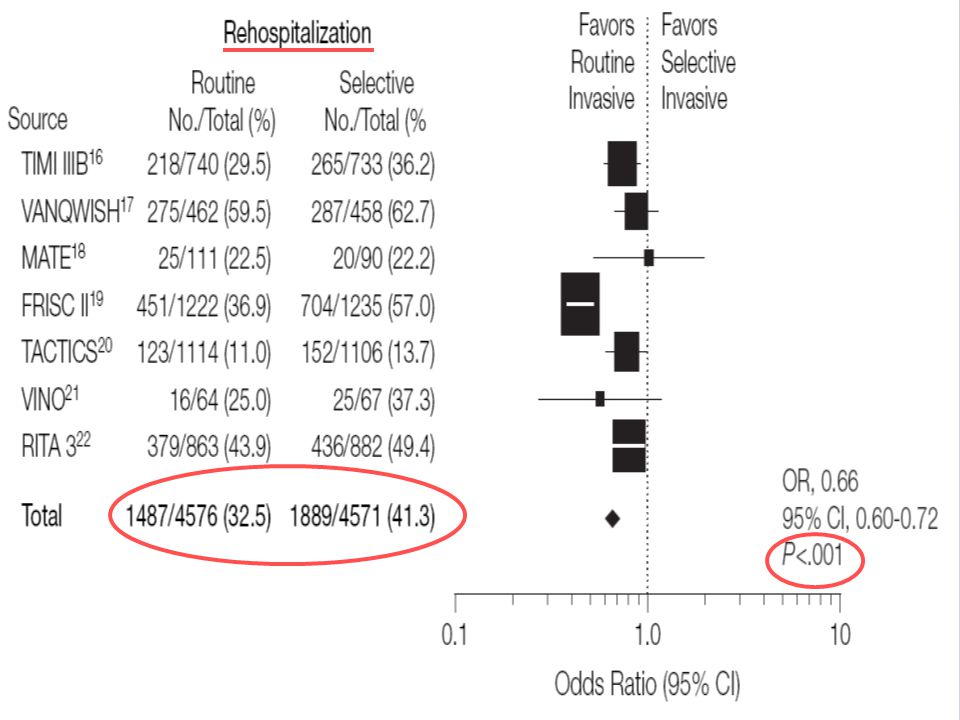
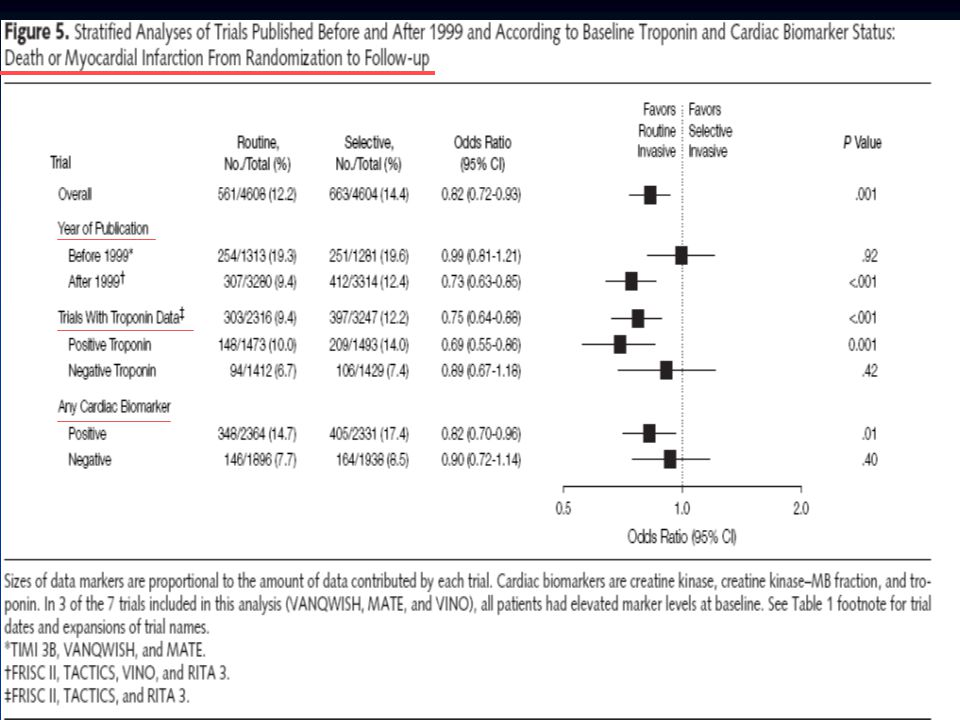
META ANALYSE Revue de la littérature de 1970 -> juin 2004 7 études randomisées incluant 9212 patients => 4608 ROUTINE INVASIVE vs 4604 SELECTIVE INVASIVE -> mortalité -> IDM non mortels -> décès combinés/IDM -> angor -> taux de réhospitalisations Sortie de l’hôpital Fin du suivit Randomisation

4
les études…

5
caractéristiques des patients

6
Résultats

7
RANDOMISATIONSORTIE DE L’HOPITAL

11
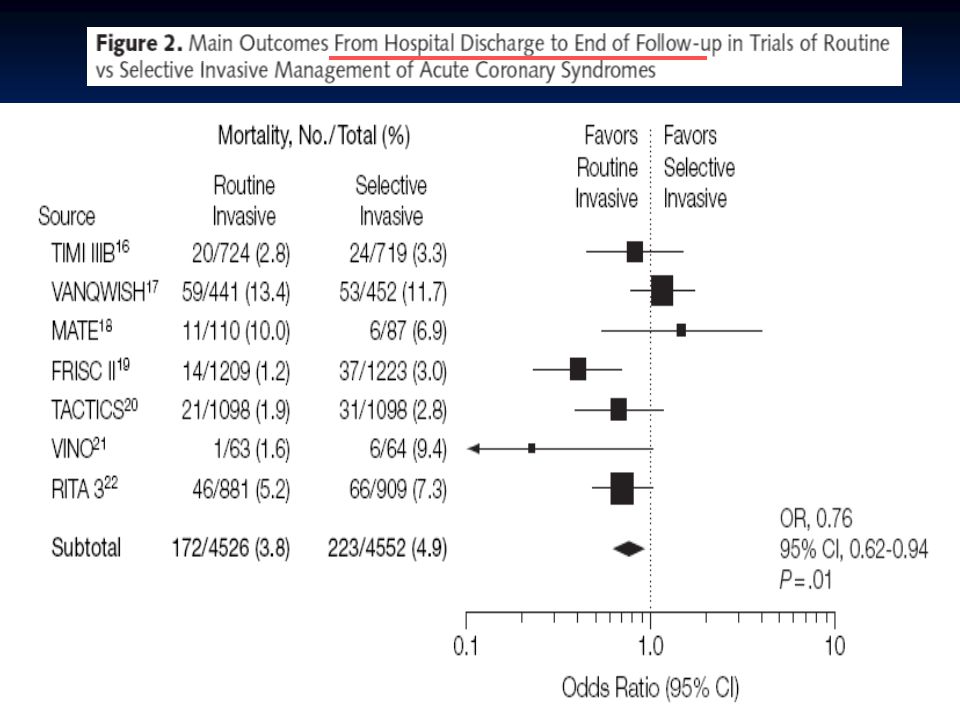
FIN DU SUIVIT

15
RANDOMISATION

21
Interprétations et conclusions

22
Stratégie invasive au cours de syndrome coronariens aigus sans sus décalage du segment ST diminue le risque combiné de décès ou de récidive d’événements ischémiques et de réhospitalisations. Ce bénéfice émerge après la sortie de l’hôpital Et ce… au prix d’une mortalité plus élevée durant l’hospitalisation

23
ABCIXIMAB TICLOPIDINE STENT Faible taux de CROSS OVER Mortalité moins élevée chez les pontés n=201 IDM AIGU CROSS OVER++ IDM NON q Exclusion de 247patients à haut risque) Mortalté apres pontage↑ 44% revascularisation TICLOPIDINE
 Mortalté apres pontage↑ 44% revascularisation TICLOPIDINE")
24
les traitements utilisés n’étaient pas les mêmes …clopidogrel et antigp2b3a … l’utilisation des stents… l’utilisation des stents… évolution des techniques de cathéterisme et de chirurgies cardiaques évolution des techniques de cathéterisme et de chirurgies cardiaques CROSS OVER CROSS OVER durées de suivit très variables durées de suivit très variables

29
Que faire ?

30
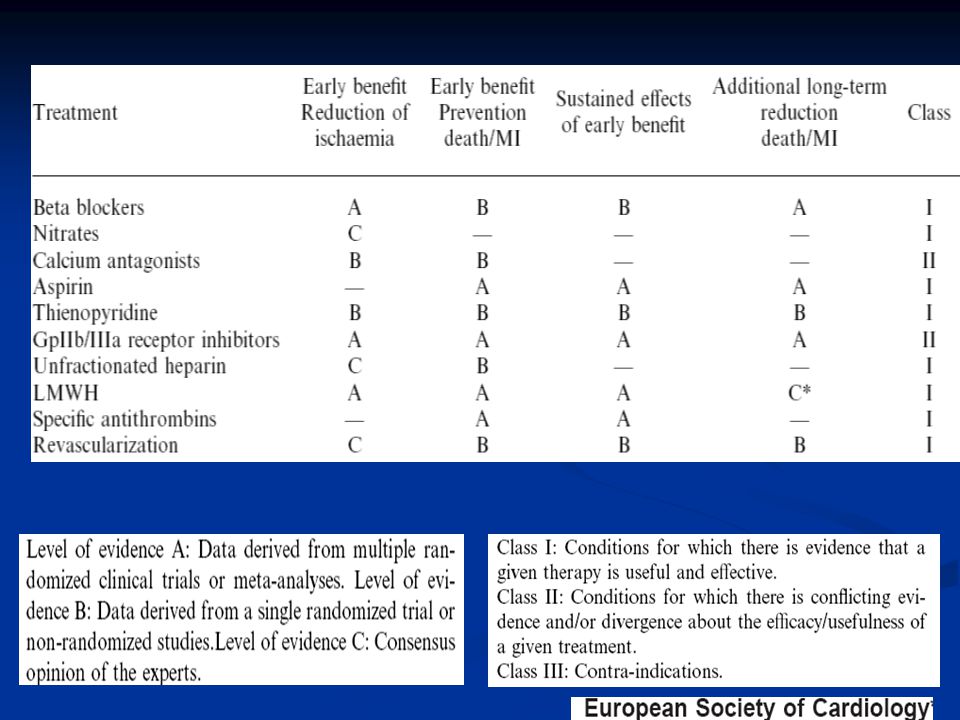
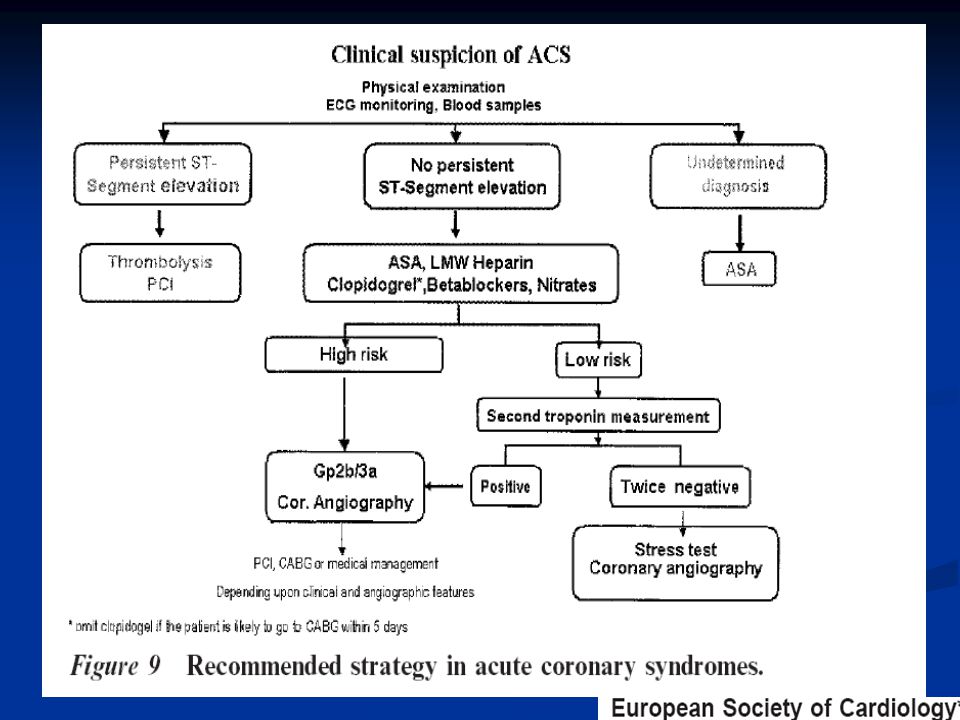
Traitement médical «optimal» : aspirine clopidogrel ß bloquant dérivés nitrés héparine (hbpm) antiGp2b3a IEC / statines
 antiGp2b3a IEC / statines")
31
STEPHEN D. WIVIOTT, M.D., and EUGENE BRAUNWALD, M.D

33
bibliographie - Braunwald E et al. ACC/AHA guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction Circulation. 2002;106:1893-1900. - TIMI IIIB Investigators. Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non-Q-wave myocardial infarction: results of theTIMI IIIBtrial. Circulation. 1994;89:1545-1556. - Boden WE, O’Rourke RA, Crawford MH, et al;Veterans Affairs Non-Q-Wave Infarction Strategies inHospital (VANQWISH) Trial Investigators. Outcomes in patients with acute non-Q-wave myocardial infarction randomly assigned to an invasive as compared with a conservative management strategy.N Engl J Med. 1998;338:1785-1792. -FRagmin and Fast Revascularisation during In-Stability in Coronary artery disease (FRISC II) Investigators. Invasive compared with non-invasive treatment in unstable coronary-artery disease: FRISC II prospective randomised multicentre study. Lancet.1999;354:708-715.20. -Wiviott SD, Braunwald E.Unstable angina and non-ST-segment elevation myocardial infarction: part I. Initial evaluation and management, and hospital care. Am Fam Physician. 2004 Aug 1;70(3):525-32.
 Trial Investigators. Outcomes in patients with acute non-Q-wave myocardial infarction randomly assigned to an invasive as compared with a conservative management strategy.N Engl J Med. 1998;338: FRagmin and Fast Revascularisation during In-Stability in Coronary artery disease (FRISC II) Investigators. Invasive compared with non-invasive treatment in unstable coronary-artery disease: FRISC II prospective randomised multicentre study. Lancet.1999;354: Wiviott SD, Braunwald E.Unstable angina and non-ST-segment elevation myocardial infarction: part I. Initial evaluation and management, and hospital care. Am Fam Physician Aug 1;70(3):")
34
- Cannon CP, Weintraub WS, Demopoulos LA, et al; TACTICS (Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive or Conservative Strategy)—Thrombolysis in Myocardial Infarction 18 Investigators. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887. - Fox KA, Poole-Wilson PA, Henderson RA, et al; Randomized Intervention Trial of unstable Angina Investigators. Interventional versus conservative treatment for patients with unstable angina or non- STelevationmyocardial infarction: the British Heart Foundation RITA 3 randomised trial. Lancet. 2002;360:743-751 - PURSUIT Trial Investigators. Inhibition of plateletglycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. N Engl J Med. 1998;339:436-443. - Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina andnon-Q-wave myocardial infarction. N Engl J Med.1998;338:1488-1497. -CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494-502. -SYNERGY Trial Investigators. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST- segment elevation acute coronary syndromes managedwith an intended early invasive strategy: primaryresults of the SYNERGY randomized trial.. JAMA. 2004;292:45-54.
 Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina andnon-Q-wave myocardial infarction. N Engl J Med.1998;338: CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345: SYNERGY Trial Investigators. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST- segment elevation acute coronary syndromes managedwith an intended early invasive strategy: primaryresults of the SYNERGY randomized trial.. JAMA. 2004;292:")
Présentations similaires













 1-IEC 2-B Bloquant 3-ARA 2 4-Anti-aldostérone.>")

>")
>")


 mortality and reinfarction at 1 year.>")