Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Physiopathologie de l’hypertension artérielle pulmonaire
Pr Anh Tuan DINH-XUAN Service de Physiologie-Explorations Fonctionnelles Pôle Cœur-Poumons – Hôpital Cochin

2
Historique 1891 : Romberg (Deutsch Arch Klin Med 48:197)
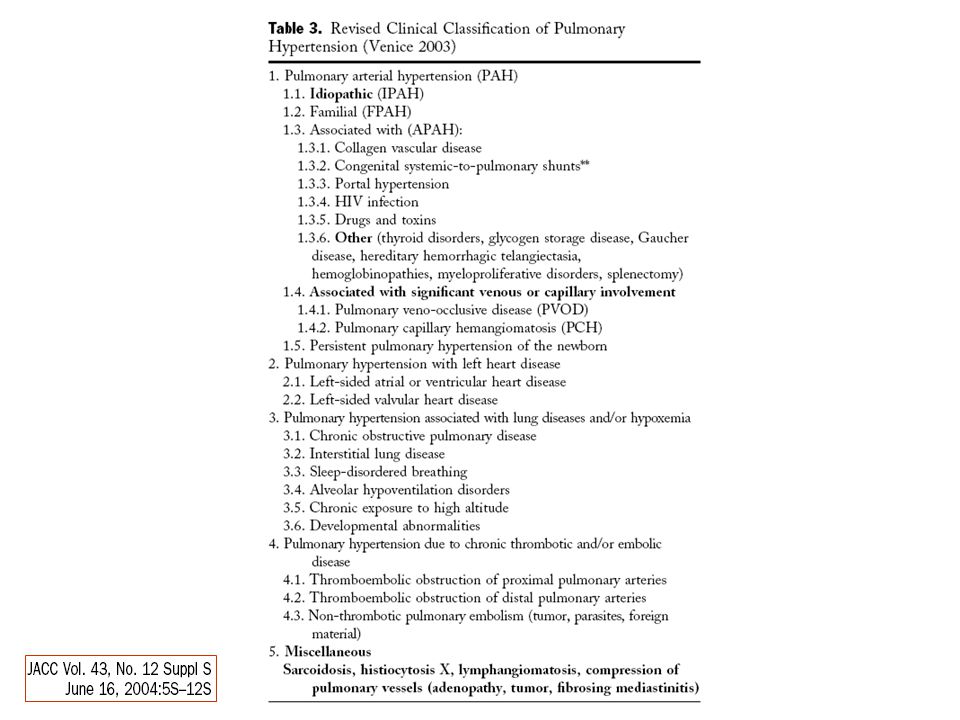
1907 : Monckerberg (Deutsch Med Wschr 33: 1243) sclérose primitive de l’artère pulmonaire 1927 : Durand endartérite oblitérante primitive de l’artère pulmonaire 1935 : Brenner (Arch Intern Med 56:976) artériosclérose pulmonaire primitive 1950 : Wood (Br Med J ii:693) 1951 : Dresdale et al (Am J Med 11:686) hypertension artérielle pulmonaire primitive Organisation Mondiale de la Santé 1973 (Genève) 1998 (Evian) 2003 (Venise) J Am Coll Cardiol 2004; 43 (suppl 12): S5-S12.
 sclérose primitive de l’artère pulmonaire : Durand endartérite oblitérante primitive de l’artère pulmonaire : Brenner (Arch Intern Med 56:976) artériosclérose pulmonaire primitive : Wood (Br Med J ii:693) 1951 : Dresdale et al (Am J Med 11:686) hypertension artérielle pulmonaire primitive. Organisation Mondiale de la Santé (Genève) 1998 (Evian) 2003 (Venise) J Am Coll Cardiol 2004; 43 (suppl 12): S5-S12.")
4
Humbert et al. N Engl J Med 2004; 351: 1425-36.
Targets for Current or Emerging Therapies in Pulmonary Arterial Hypertension Figure 1. Targets for Current or Emerging Therapies in Pulmonary Arterial Hypertension. Three major pathways involved in abnormal proliferation and contraction of the smooth-muscle cells of the pulmonary artery in patients with pulmonary arterial hypertension are shown. These pathways correspond to important therapeutic targets in this condition and play a role in determining which of four classes of drugs — endothelin-receptor antagonists, nitric oxide, phosphodiesterase type 5 inhibitors, and prostacyclin derivatives — will be used. At the top of the figure, a transverse section of a small pulmonary artery (<500 µm in diameter) from a patient with severe pulmonary arterial hypertension shows intimal proliferation and marked medial hypertrophy. Dysfunctional pulmonary-artery endothelial cells (blue) have decreased production of prostacyclin and endogenous nitric oxide, with an increased production of endothelin-1 — a condition promoting vasoconstriction and proliferation of smooth-muscle cells in the pulmonary arteries (red). Current or emerging therapies interfere with specific targets in smooth-muscle cells in the pulmonary arteries. In addition to their actions on smooth-muscle cells, prostacyclin derivatives and nitric oxide have several other properties, including antiplatelet effects. Plus signs denote an increase in the intracellular concentration; minus signs blockage of a receptor, inhibition of an enzyme, or a decrease in the intracellular concentration; and cGMP cyclic guanosine monophosphate. Humbert et al. N Engl J Med 2004; 351:
 from a patient with severe pulmonary arterial hypertension shows intimal proliferation and marked medial hypertrophy. Dysfunctional pulmonary-artery endothelial cells (blue) have decreased production of prostacyclin and endogenous nitric oxide, with an increased production of endothelin-1 — a condition promoting vasoconstriction and proliferation of smooth-muscle cells in the pulmonary arteries (red). Current or emerging therapies interfere with specific targets in smooth-muscle cells in the pulmonary arteries. In addition to their actions on smooth-muscle cells, prostacyclin derivatives and nitric oxide have several other properties, including antiplatelet effects. Plus signs denote an increase in the intracellular concentration; minus signs blockage of a receptor, inhibition of an enzyme, or a decrease in the intracellular concentration; and cGMP cyclic guanosine monophosphate. Humbert et al. N Engl J Med 2004; 351:")
5
Major signal transduction pathways in SMC induced by PG and TXA2
Prostacyclin and its analogues in the treatment of pulmonary hypertension Horst Olschewski , , Frank Rose, Ralph Schermuly, H. Ardeschir Ghofrani, Beate Enke, Andrea Olschewski and Werner Seeger Pharmacology & Therapeutics Volume 102, Issue 2 , May 2004, Pages Fig. 1. Major signal transduction pathways in SMC induced by PG and TXA2. PG and TXA2 receptors are coupled to different intracellular signaling cascades via activation of specific G proteins. After binding to different receptors, the vessel tone is changed via Gs (stimulatory)- and Gi (inhibitory)-coupled control of adenylate cyclase (AC). The vasodilatory effects are mediated by activation of protein kinase A (PKA), whereas the vasoconstrictor effects are mediated by Gq-coupled phosphoinositide breakdown activating the release of Ca2+ from the sarcoplasmic reticulum (SR). DAG, diacylglycerol; IP3, inositol-1,4,5-phosphate; PKC, protein kinase C; PLC, phospholipase C; vein, pulmonary veins; DA, ductus arteriosus. From Olschewski et al. (2001a). Olschewski et al. J Lab Clin Med 2001; 138:
- and Gi (inhibitory)-coupled control of adenylate cyclase (AC). The vasodilatory effects are mediated by activation of protein kinase A (PKA), whereas the vasoconstrictor effects are mediated by Gq-coupled phosphoinositide breakdown activating the release of Ca2+ from the sarcoplasmic reticulum (SR). DAG, diacylglycerol; IP3, inositol-1,4,5-phosphate; PKC, protein kinase C; PLC, phospholipase C; vein, pulmonary veins; DA, ductus arteriosus. From Olschewski et al. (2001a). Olschewski et al. J Lab Clin Med 2001; 138:")
6
Muscle lisse vasculaire Relaxation
NO Inhibiteurs de la PDE-5 Muscle lisse vasculaire GTP GMPc GCs PDE-5 5’-GMP PKG Relaxation

7
Beavo & Brunton. Nature Rev Mol Cell Biol 2002; 3: 710-8.
PDE5 inhibitors Nature Reviews Molecular Cell Biology 3; (2002); doi: /nrm911 CYCLIC NUCLEOTIDE RESEARCH — STILL EXPANDING AFTER HALF A CENTURY Box 2 | Mechanism of action of the drug Viagra® Penile erection occurs when blood swells the corpus cavernosum, an effect facilitated by relaxation of regional smooth muscle. Smooth muscle tone is regulated by cellular Ca2+, which activates the Ca2+/calmodulin (CaM)-dependent enzyme myosin light chain kinase (MLCK), which leads to MLC phosphorylation and contraction. The nitric oxide (NO) pathway leads to relaxation of smooth muscle by stimulating the soluble guanylyl cyclase (sGC), which results in the production of cyclic GMP (cGMP) and the activation of cGMP-dependent protein kinase (PKG). PKG causes smooth-muscle relaxation by mechanisms that are still being defined and that might include a reduction in cytosolic Ca2+ (by enhanced Ca2+ export and/or by reduced inositol trisphosphate (InsP3) receptor-mediated Ca2+ mobilization) and dephosphorylation of myosin light chains (by activation of MLC phosphatase and/or by sequestration of MLCK in a phosphorylated form that is not readily activated by Ca2+/CaM). Viagra® specifically inhibits the breakdown of cellular cGMP by PDE5 (an isoform of phosphodiesterase that is localized to erectile tissue), and thereby prolongs and enhances the effects of NO/cGMP. Beavo & Brunton. Nature Rev Mol Cell Biol 2002; 3:
; doi: /nrm911 CYCLIC NUCLEOTIDE RESEARCH — STILL EXPANDING AFTER HALF A CENTURY. Box 2 | Mechanism of action of the drug Viagra® Penile erection occurs when blood swells the corpus cavernosum, an effect facilitated by relaxation of regional smooth muscle. Smooth muscle tone is regulated by cellular Ca2+, which activates the Ca2+/calmodulin (CaM)-dependent enzyme myosin light chain kinase (MLCK), which leads to MLC phosphorylation and contraction. The nitric oxide (NO) pathway leads to relaxation of smooth muscle by stimulating the soluble guanylyl cyclase (sGC), which results in the production of cyclic GMP (cGMP) and the activation of cGMP-dependent protein kinase (PKG). PKG causes smooth-muscle relaxation by mechanisms that are still being defined and that might include a reduction in cytosolic Ca2+ (by enhanced Ca2+ export and/or by reduced inositol trisphosphate (InsP3) receptor-mediated Ca2+ mobilization) and dephosphorylation of myosin light chains (by activation of MLC phosphatase and/or by sequestration of MLCK in a phosphorylated form that is not readily activated by Ca2+/CaM). Viagra® specifically inhibits the breakdown of cellular cGMP by PDE5 (an isoform of phosphodiesterase that is localized to erectile tissue), and thereby prolongs and enhances the effects of NO/cGMP. Beavo & Brunton. Nature Rev Mol Cell Biol 2002; 3:")
8
Griffiths & Evans. N Engl J Med 2005; 353: 2683-95.
Inhaled Nitric Oxide Therapy in Adults Mark J.D. Griffiths, M.R.C.P., Ph.D., and Timothy W. Evans, M.D., Ph.D. Figure 1. Regulation of the Relaxation of Vascular Smooth Muscle by Nitric Oxide. Nitric oxide activates soluble guanylyl cyclase, leading to the activation of cyclic guanosine 3' 5'-monophosphate (cGMP)–dependent protein kinase (cGKI). In turn, cGKI decreases the sensitivity of myosin to calcium-induced contraction and lowers the intracellular calcium concentration by activating calcium-sensitive potassium channels and inhibiting the release of calcium from the sarcoplasmic reticulum. cGMP is degraded by phosphodiesterase type 5, which is inhibited by sildenafil and zaprinast. GTP denotes guanosine triphosphate. Griffiths & Evans. N Engl J Med 2005; 353:
–dependent protein kinase (cGKI). In turn, cGKI decreases the sensitivity of myosin to calcium-induced contraction and lowers the intracellular calcium concentration by activating calcium-sensitive potassium channels and inhibiting the release of calcium from the sarcoplasmic reticulum. cGMP is degraded by phosphodiesterase type 5, which is inhibited by sildenafil and zaprinast. GTP denotes guanosine triphosphate. Griffiths & Evans. N Engl J Med 2005; 353:")
9
Canaux K+ et Ca2+ Am. J. Respir. Crit. Care Med., Volume 157, Number 4, April 1998, S101-S108 The Pulmonary Circulation Snapshots of Progress JOHN T. REEVES and LEWIS J. RUBIN Figure 1. The effect of redox state on membrane potassium channel activity. Normoxia is associated with open channels, whereas hypoxia results in closing of the potassium channels, leading to membrane depolarization, opening of voltage-gated calcium channels, influx of calcium into the cytosol, and vasoconstriction. Oxidizing compounds mimic normoxia, while reducing agents mimic the effects of hypoxia. Reeves & Rubin. Am J Respir Crit Care Med 1998; 157: S101-8.

10
Glycémie KATP K+ Cellule b Ca2+ Ca (VOC) I ATP I Dépolarisation Ca2+
Glucose Ouvreurs des KATP Sulfamides hypoglycémiants K+ KATP ATP Dépolarisation I I Ca2+ Ca2+ Ca (VOC)
")
11
NO, GMPc, AMPc et canaux potassiques
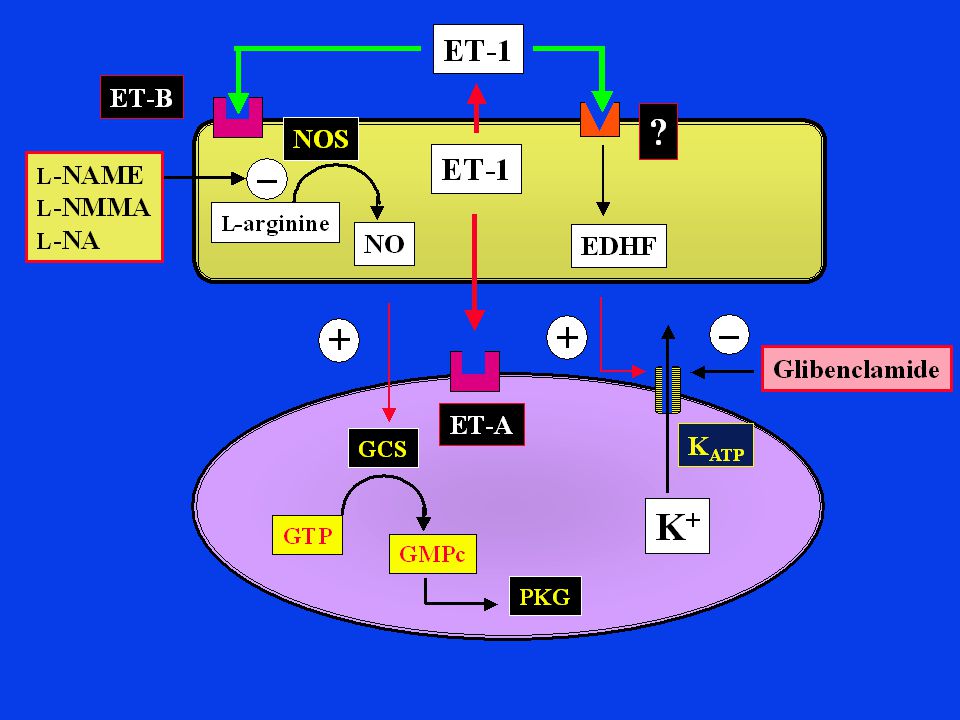
Potassium Channel Function in Vascular Disease Christopher G. Sobey Arteriosclerosis, Thrombosis, and Vascular Biology. 2001;21: Figure 2. Some potential mechanisms involving K+ channel–mediated, endothelium-dependent hyperpolarization. Stimulation of endothelial cell receptors by agonists such as acetylcholine (ACh), bradykinin (BK), and substance P (SP) may cause release of several endothelium-derived relaxing factors. These include NO, EDHF(s), and prostacyclin (PGI2), each of which can induce relaxation of underlying vascular muscle through activation of K+ channels. In the case of NO and PGI2, this may involve the intracellular accumulation of a second messenger (cyclic GMP and cAMP, respectively). Like EDHF, NO may activate K+ channels directly. The production of EDHF may depend on the bioavailability of NO, such that EDHF release may be more significant under conditions in which NO production is impaired. The hyperpolarization occurring in response to K+ channel activation leads to vasodilatation, as described in Figure 1 . Because all 3 endothelial factors may normally activate vascular K+ channels, endothelial dysfunction occurring during cardiovascular disease states may result in vascular depolarization and/or abnormal K+ channel function, leading to increased vascular tone and reduced blood flow. Sobey. Arterio Scler Thromb Vasc Biol 2001; 21:
, bradykinin (BK), and substance P (SP) may cause release of several endothelium-derived relaxing factors. These include NO, EDHF(s), and prostacyclin (PGI2), each of which can induce relaxation of underlying vascular muscle through activation of K+ channels. In the case of NO and PGI2, this may involve the intracellular accumulation of a second messenger (cyclic GMP and cAMP, respectively). Like EDHF, NO may activate K+ channels directly. The production of EDHF may depend on the bioavailability of NO, such that EDHF release may be more significant under conditions in which NO production is impaired. The hyperpolarization occurring in response to K+ channel activation leads to vasodilatation, as described in Figure 1 . Because all 3 endothelial factors may normally activate vascular K+ channels, endothelial dysfunction occurring during cardiovascular disease states may result in vascular depolarization and/or abnormal K+ channel function, leading to increased vascular tone and reduced blood flow. Sobey. Arterio Scler Thromb Vasc Biol 2001; 21:")
12
2 4 5 6 7 14 6 7 Fig. 1. Amino acid sequence of human ETs and STXc. Amino acid substitutions with respect to ET-1 are indicated. Pharmacological Reviews. Vol. 51, Issue 3, , September 1999 Autocrine-Paracrine Endothelin System in the Physiology and Pathology of Steroid-Secreting Tissues Gastone G. Nussdorfer1, Gian Paolo Rossi, Ludwik K. Malendowicz and Giuseppina Mazzocchi

13
Fig. 1. Amino acid sequence of human ETs and STXc
Fig. 1. Amino acid sequence of human ETs and STXc. Amino acid substitutions with respect to ET-1 are indicated. Pharmacological Reviews. Vol. 51, Issue 3, , September 1999 Autocrine-Paracrine Endothelin System in the Physiology and Pathology of Steroid-Secreting Tissues Gastone G. Nussdorfer1, Gian Paolo Rossi, Ludwik K. Malendowicz and Giuseppina Mazzocchi

22
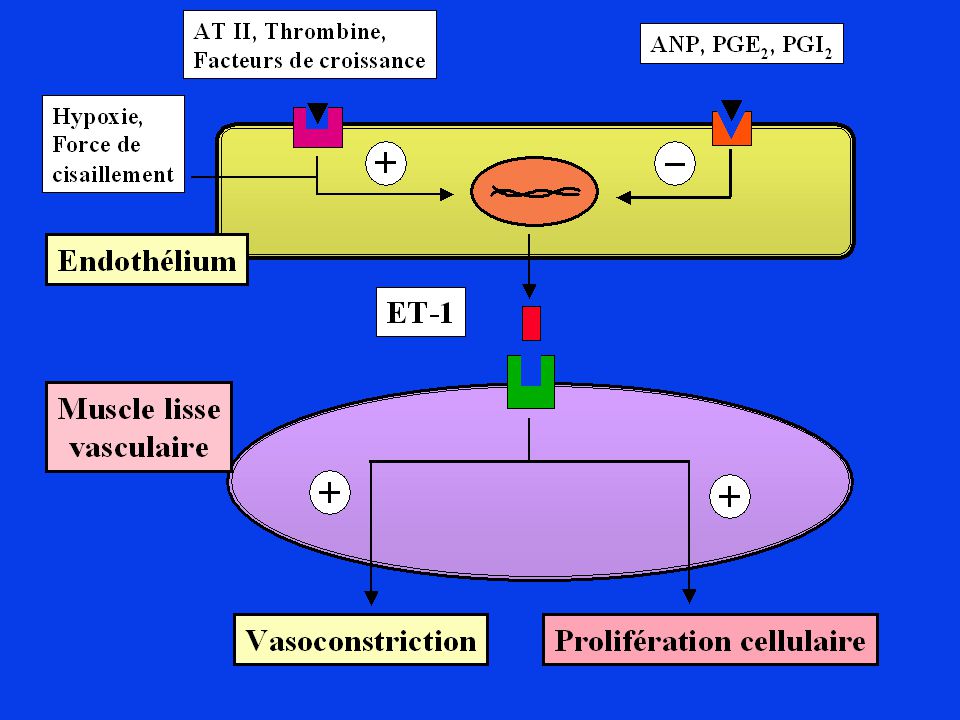
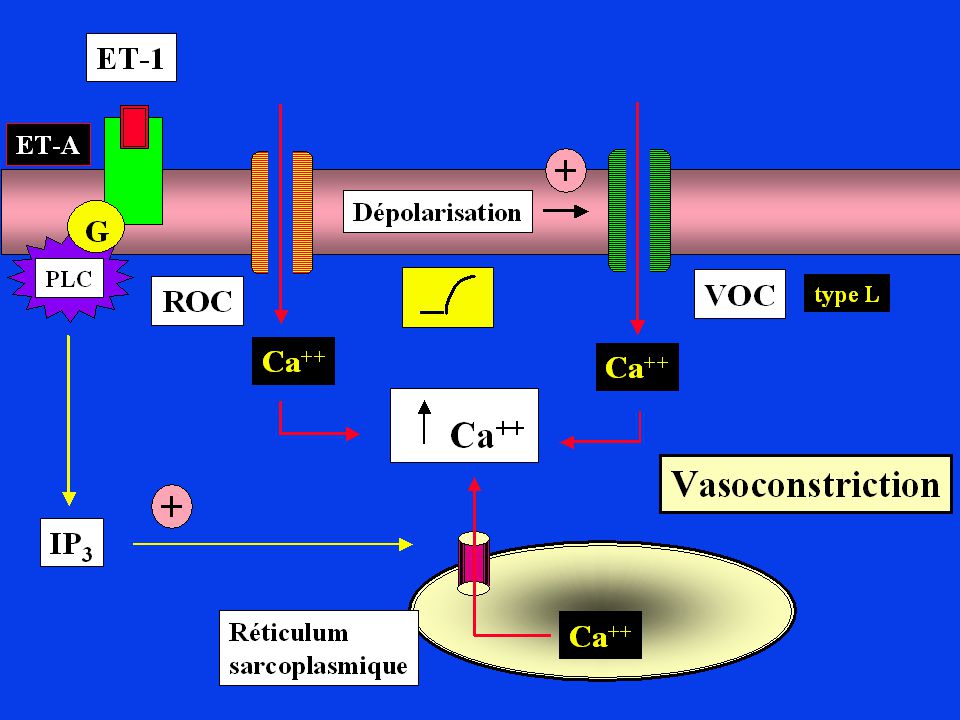
A B C Nature Reviews Drug Discovery 1; (2002); doi: /nrd962 NEW THERAPEUTICS THAT ANTAGONIZE ENDOTHELIN: PROMISES AND FRUSTRATIONS Figure 1 | Regulation of ET-1 synthesis, pathway of ET generation and ET-receptor-mediated actions on smooth muscle cells. Endothelin-1 (ET-1) synthesis is regulated by many factors; stimulators are highlighted in green, and inhibitors are highlighted in red. The product of ET1 transcription is prepro-ET-1, which is cleaved by a neutral endopeptidase to form the active precursor pro-ET-1 or big ET-1. Big ET-1 is converted to the mature peptide by the metalloproteinase endothelin-converting enzyme-1 (ECE-1)1. Two ET receptors have been identified in the vasculature: ET type-A receptors (ETA) reside in vascular smooth muscle cells and mediate vasoconstriction and cell proliferation, whereas ETB receptors reside on endothelial cells and are mainly vasodilatory through NO (which in turn can mediate the anti-apoptotic effects of ET-1), and regulate the synthesis of ET-1. ETB receptors on smooth muscle cells can elicit vessel contraction43. CsA, cyclosporin A; EGF, epidermal growth factor; HGF, hepatocyte growth factor; IL-1, interleukin-1; LDL, low-density lipoprotein; VEGF, vascular endothelial growth factor.
 synthesis is regulated by many factors; stimulators are highlighted in green, and inhibitors are highlighted in red. The product of ET1 transcription is prepro-ET-1, which is cleaved by a neutral endopeptidase to form the active precursor pro-ET-1 or big ET-1. Big ET-1 is converted to the mature peptide by the metalloproteinase endothelin-converting enzyme-1 (ECE-1)1. Two ET receptors have been identified in the vasculature: ET type-A receptors (ETA) reside in vascular smooth muscle cells and mediate vasoconstriction and cell proliferation, whereas ETB receptors reside on endothelial cells and are mainly vasodilatory through NO (which in turn can mediate the anti-apoptotic effects of ET-1), and regulate the synthesis of ET-1. ETB receptors on smooth muscle cells can elicit vessel contraction43. CsA, cyclosporin A; EGF, epidermal growth factor; HGF, hepatocyte growth factor; IL-1, interleukin-1; LDL, low-density lipoprotein; VEGF, vascular endothelial growth factor.")
23
Role of Nitric Oxide in the Pathogenesis of Chronic Pulmonary Hypertension
Václav Hampl and Jan Herget Physiol. Rev. 80: , 2000 Fig. 1. Major mechanisms causing pulmonary hypertension. Hampl & Herget. Physiol Rev 2000; 80:

24
Humbert et al. N Engl J Med 2004; 351: 1425-36.
Targets for Current or Emerging Therapies in Pulmonary Arterial Hypertension Figure 1. Targets for Current or Emerging Therapies in Pulmonary Arterial Hypertension. Three major pathways involved in abnormal proliferation and contraction of the smooth-muscle cells of the pulmonary artery in patients with pulmonary arterial hypertension are shown. These pathways correspond to important therapeutic targets in this condition and play a role in determining which of four classes of drugs — endothelin-receptor antagonists, nitric oxide, phosphodiesterase type 5 inhibitors, and prostacyclin derivatives — will be used. At the top of the figure, a transverse section of a small pulmonary artery (<500 µm in diameter) from a patient with severe pulmonary arterial hypertension shows intimal proliferation and marked medial hypertrophy. Dysfunctional pulmonary-artery endothelial cells (blue) have decreased production of prostacyclin and endogenous nitric oxide, with an increased production of endothelin-1 — a condition promoting vasoconstriction and proliferation of smooth-muscle cells in the pulmonary arteries (red). Current or emerging therapies interfere with specific targets in smooth-muscle cells in the pulmonary arteries. In addition to their actions on smooth-muscle cells, prostacyclin derivatives and nitric oxide have several other properties, including antiplatelet effects. Plus signs denote an increase in the intracellular concentration; minus signs blockage of a receptor, inhibition of an enzyme, or a decrease in the intracellular concentration; and cGMP cyclic guanosine monophosphate. Humbert et al. N Engl J Med 2004; 351:
 from a patient with severe pulmonary arterial hypertension shows intimal proliferation and marked medial hypertrophy. Dysfunctional pulmonary-artery endothelial cells (blue) have decreased production of prostacyclin and endogenous nitric oxide, with an increased production of endothelin-1 — a condition promoting vasoconstriction and proliferation of smooth-muscle cells in the pulmonary arteries (red). Current or emerging therapies interfere with specific targets in smooth-muscle cells in the pulmonary arteries. In addition to their actions on smooth-muscle cells, prostacyclin derivatives and nitric oxide have several other properties, including antiplatelet effects. Plus signs denote an increase in the intracellular concentration; minus signs blockage of a receptor, inhibition of an enzyme, or a decrease in the intracellular concentration; and cGMP cyclic guanosine monophosphate. Humbert et al. N Engl J Med 2004; 351:")
Présentations similaires



>")















