Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez


1
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Correct treatment Safer sexual behavior promotion Condom promotion Tt completed Cured

2
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Correct treatment Partner treatment Education to recognize symptoms Screening at FP, ANC… Tt completed Cured

3
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Staff behavior Health seeking behavior promotion Correct treatment Tt completed Cured

4
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Syndromic approach Include STD drug in essential list Correct treatment Prescribe single dose Counsel for compliance Tt completed Cured

7
Iconographie atlas

8
Iconographie atlas

15
Iconographie atlas

16
Iconographie atlas

17
Iconographie atlas

19
(Czelusta A. J Am Acad Dermatol 2000;43:409-32.)
Fig 5. HIV-positive patient. Chancroid with typical “kissing” ulcers. (Czelusta A. J Am Acad Dermatol 2000;43: )
")
20
Iconographie atlas

24
Chancre mou- une ou plusieurs ulcérations anales, purulentes- adénopathie inguinale inflammatoire évoluant vers la suppuration

25
CHANCRE MOU (chancroid)
Azithromycin 1 g orally in a single dose, OR Ceftriaxone 250 mg intramuscularly (IM) in a single dose, Ciprofloxacin 500 mg orally twice a day for 3 days, Erythromycin base 500 mg orally three times a day for 7 days. (CDC,2006)
 in a single dose, Ciprofloxacin 500 mg orally twice a day for 3 days, Erythromycin base 500 mg orally three times a day for 7 days. (CDC,2006)")
26
CHANCRE MOU (chancroid)
Ciprofloxacin 500 mg orally X 2 j X 3 j, OU Erythromycine base 500 mg p os X 3 x j X 7 j, Azithromycine 1 g p os X 1 Alternative: Ceftriaxone 250 mg intramuscularly (IM) X 1, (OMS, 2004)
 X 1, (OMS, 2004)")
34
Jean-Elie Malkin, Cours IST, IMEA

35
Jean-Elie Malkin, Cours IST, IMEA

36
Jean-Elie Malkin, Cours IST, IMEA

38
Jean-Elie Malkin, Cours IST, IMEA

40
Jean-Elie Malkin, Cours IST, IMEA

41
Bruno Halioua, Institut Alfred Fournier

47
Bruno Halioua, Institut Alfred Fournier

48
Ulcérations herpétiques chez co-infecté VHC/HIV>Fe…Emmanuel

49
Herpes simulant un Chancre ulcéreux, Martinique

50
Ulcérations herpétiques chez co-infecté VHC/HIV>Fe…Emmanuel

51
Herpès atypique chez HIV +: reconstitution Bo….Gérard

52
Herpès atypique chez HIV +: reconstitution Ful Rch

53
Herpès atypique chez HIV +: reconstitution Ful Rch

54
Herpès atypique chez HIV +: reconstitution Ul Brune…

59
Increasing role in HIV susceptibility attributed to HSV-2 (a)
31 studies of HSV-2 seropositive have RR=2.1 of HIV infection when herpes precedes HIV Among HSV-2 sero + persons, 52% of ST HIV infection attributed to HSV Population attributable risk % varies with HSV seroprevalence: 19% for the ST-HIV infection in the general pop (HSV seroprev=22%) and 50% for ST HIV in CSWs (HSV seroprev=80%) Wad. A et al. J Infect Dis, 2002, 185, 45-52)
 and 50% for ST HIV in CSWs (HSV seroprev=80%) Wad. A et al. J Infect Dis, 2002, 185, 45-52)")
60
HSV2 est plus répandu qu’on ne le croyait en Afrique sub-saharienne: responsable de 44% des ulceres génitaux à Rakai. Multiplie par >2x le risque de transmission du VIH Ronald Gray, M.D. Reducing HIV transmission: Lessons Reducing HIV transmission: Lessons from Rakai and other African from Rakai and other African studies. IAS, Rio de Janeiro, 2005

61
Vanmali et al. ICAAC, 2001/ Chen et al 2000/O'Farell, 1994
Increasing role in HIV susceptibility attributed to HSV-2 (c): Etiology of GUD (%) South Afr 94 South Afr. 00 Tanzania T pallidum 30 16.2 15 H ducreyi 12 24.5 10 HSV 9 29.2 45 TP + HD 8 1.7 TP + HSV 1 1.1 HD + HSV 4.8 All 3 agents 0.7 Mixed no HSV 2 LGV 3 C. granulom. Indeterm. 23 21.7 HIV Serop. 40 Vanmali et al. ICAAC, 2001/ Chen et al 2000/O'Farell, 1994
: Etiology of GUD (%) South Afr 94. South Afr. 00. Tanzania. T pallidum H ducreyi HSV TP + HD TP + HSV HD + HSV All 3 agents Mixed no HSV. 2. LGV. 3. C. granulom. Indeterm HIV Serop. 40. Vanmali et al. ICAAC, 2001/ Chen et al 2000/O Farell,")
62
Herpès génital chez des malades africains souffrant d’ulcération génitale : Evolution 1980-1999
Pourcentage de HSV-2 isolé D’après O’Farrell STI 1999 Jean-Elie Malkin, Cours IST, IMEA

63
Increasing role in HIV susceptibility attributed to HSV-2 (b)
Development of nucleic acid amplification technology (M-PCR) facilitate diagnostic of GUD and by its higher sensitivity change the reported proportion of each of the etiologic agent HSV-2 may be responsible for a greater population-attributable risk of HIV infection than previously thought In WHO algorithms of treatment no viral suppressive treatment was scheduled and this had been recently changed Chen CY et al. Sex Transm Dis, 2000, 1, 21-29
 facilitate diagnostic of GUD and by its higher sensitivity change the reported proportion of each of the etiologic agent. HSV-2 may be responsible for a greater population-attributable risk of HIV infection than previously thought. In WHO algorithms of treatment no viral suppressive treatment was scheduled and this had been recently changed. Chen CY et al. Sex Transm Dis, 2000, 1,")
64
HSV-2 and HIV acquisition meta-analysis:
Risk of HIV infection in HSV-2 infected persons: A: 9 Longitudinal & nested case-control studies: RR=2.1 ( ) B: 22 Case-control & cross sectional studies: OR=3.9 ( ) Wald A. JID: 2002;185:45-52
 B: 22 Case-control & cross sectional studies: OR=3.9 ( ) Wald A. JID: 2002;185:")
65
Les patients porteurs de sérologie positive HSV-2 ont une charge virale VIH plus élevée à Rakai
Ronald Gray, M.D. Reducing HIV transmission: Lessons Reducing HIV transmission: Lessons from Rakai and other African from Rakai and other African studies. IAS, Rio de Janeiro, 2005

66
Figure: 1. Prediction of the efficiency of HIV transmission according to HIV burden in the genital tract. A, probability of male-to-female HIV transmission per coital act, as a function of HIV disease stage in the index case. Transmission probabilities are shown for each stage of disease [3–5, 13]. Yellow, Expected distribution of viral burden in semen among men over time; red, theoretical effect of a biological intervention designed to reduce viral excretion; dashed line, a potential threshold for HIV transmission. B, Determinants of high HIV transmission probability: acute infection, sexually transmitted infection (STI), and AIDS. Marie Laga, The synergy between Prevention and Care in Africa. IAS, Rio de Janeiro, 2005
![Figure: 1. Prediction of the efficiency of HIV transmission according to HIV burden in the genital tract. A, probability of male-to-female HIV transmission per coital act, as a function of HIV disease stage in the index case. Transmission probabilities are shown for each stage of disease [3–5, 13]. Yellow, Expected distribution of viral burden in semen among men over time; red, theoretical effect of a biological intervention](http://slideplayer.fr/slide/504641/2/images/66/Figure%3A+1.+Prediction+of+the+efficiency+of+HIV+transmission+according+to+HIV+burden+in+the+genital+tract.+A%2C+probability+of+male-to-female+HIV+transmission+per+coital+act%2C+as+a+function+of+HIV+disease+stage+in+the+index+case.+Transmission+probabilities+are+shown+for+each+stage+of+disease+%5B3%E2%80%935%2C+13%5D.+Yellow%2C+Expected+distribution+of+viral+burden+in+semen+among+men+over+time%3B+red%2C+theoretical+effect+of+a+biological+intervention.jpg "designed to reduce viral excretion; dashed line, a potential threshold for HIV transmission. B, Determinants of high HIV transmission probability: acute infection, sexually transmitted infection (STI), and AIDS. Marie Laga, The synergy between Prevention and Care in Africa. IAS, Rio de Janeiro,")
67
First Clinical Episode
HERPES GENITAL First Clinical Episode Acyclovir 400 mg orally three times a day for days, OR Acyclovir 200 mg orally five times a day for days, Famciclovir 250 mg orally three times a day for days, Valacyclovir 1 g orally twice a day for days. (CDC, 2006,WHO, 2004)
")
68
Episodic Therapy for Recurrent Herpes
HERPES GENITAL Episodic Therapy for Recurrent Herpes Acyclovir 400 mg orally three times a day for 5 days*, OR Acyclovir 200 mg orally five times a day for 5 days*, Acyclovir 800 mg orally twice a day for 5 days*, Famciclovir 125 mg orally twice a day for 5 days*, Valacyclovir 500 mg orally twice a day for 3--5 days*, Valacyclovir 1.0 g orally once a day for 5 days*. (CDC, 2006,WHO, 2004) (5-10 days if HIV+, CDC)
 (5-10 days if HIV+, CDC)")
69
Suppressive Therapy for Recurrent Herpes
HERPES GENITAL Suppressive Therapy for Recurrent Herpes Acyclovir 400 mg orally twice a day, OR Famciclovir 250 mg orally twice a day, Valacyclovir 500 mg orally once a day, Valacyclovir 1.0 gram orally once a day. (CDC, 2006,WHO, 2004)
")
70
Suppressive Therapy for Recurrent Herpes if HIV+
HERPES GENITAL Suppressive Therapy for Recurrent Herpes if HIV+ Acyclovir mg orally twice to three times a day, OR Famciclovir 500 mg orally twice a day, Valacyclovir 500 mg orally twice a day. (CDC, 2006)
")
84
Hart G. Clinical Infectious Diseases 1997;25:24–32
Figure 3. Extensive granulomatous lesions of the buccal mucosa in a 30-year-old Australian Aboriginal woman. The affected gums were tender and bled on gentle contact, some teeth were loose, and a radiograph showed erosion of the underlying maxilla. The patient had been treated for genital donovanosis 2 years previously and had residual scarring (but no active lesions) at the primary site. Reprinted with permission from Australian Dental Journal [37]. Hart G. Clinical Infectious Diseases 1997;25:24–32
 at the primary site. Reprinted with permission from Australian Dental Journal [37]. Hart G. Clinical Infectious Diseases 1997;25:24–32.")
85
Hart G. Clinical Infectious Diseases 1997;25:24–32
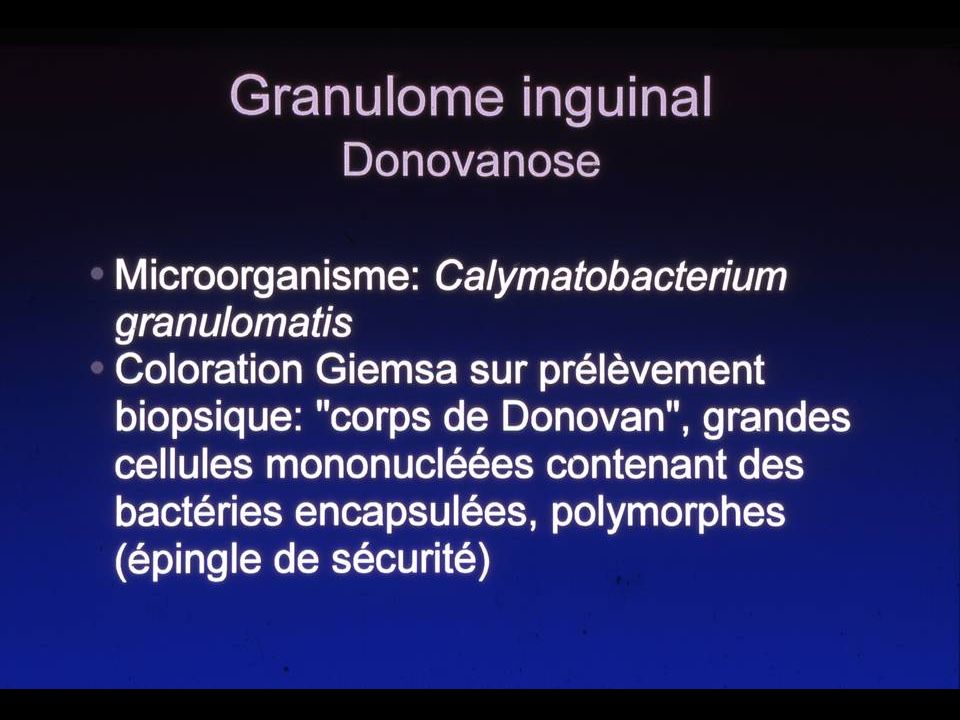
Figure 4. Typical bipolar black-staining Donovan bodies are seen in a mononuclear cell in the center of this slide. Several cells on the periphery show characteristic palisading or clustering of organisms lining the cytoplasmic vacuoles. (Stain, Warthin-Starry silver stain; original magnification, 1400.) Reproduced with permission fromCurrent Medcine [27]. Hart G. Clinical Infectious Diseases 1997;25:24–32
 Reproduced with permission fromCurrent Medcine [27]. Hart G. Clinical Infectious Diseases 1997;25:24–32.")
87
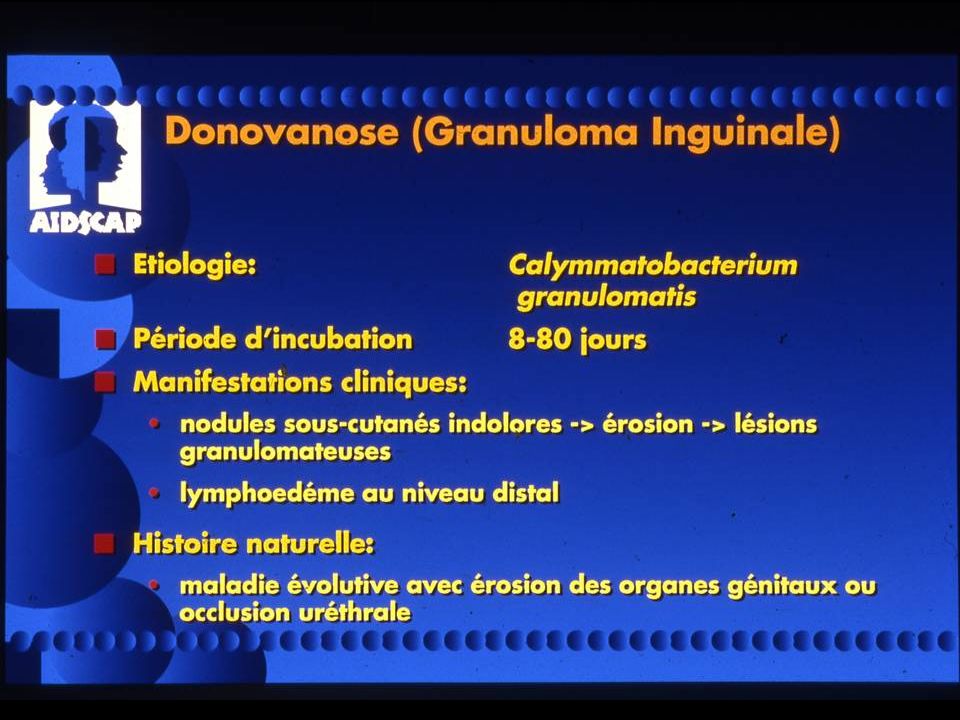
GRANULOMA INGUINALE Co-trimoxazole: 160/800 mg p os x 2 x 14j
(DONOVANOSE) Co-trimoxazole: /800 mg p os x 2 x 14j Alternatives: Doxycycline mg p os x 2 x 14 j Tetracycline 500 mg p os x 4 x 14 j + Streptomycine 1g IM x 1 x 14j (WHO, 1992)
 Co-trimoxazole: 160/800 mg p os x 2 x 14j. Alternatives: Doxycycline 100 mg p os x 2 x 14 j Tetracycline 500 mg p os x 4 x 14 j + Streptomycine 1g IM x 1 x 14j. (WHO, 1992)")
88
GRANULOMA INGUINALE Azithromycine:1g p os x 1/j
(DONOVANOSE) Azithromycine:1g p os x 1/j + 500mg p os x 1/j * Ou Doxycycline: 100 mg p os x 2/j * Alternatives: Erythromycine: 500 mg p os x 4 x/j * Tetracycline 500 mg p os x 4/j x 14 j * Cotrimoxazole 80mg/400 mg x 2 x 2/j x 14 j* (WHO, 2004)
 Azithromycine:1g p os x 1/j mg p os x 1/j * Ou. Doxycycline: 100 mg p os x 2/j * Alternatives: Erythromycine: 500 mg p os x 4 x/j * Tetracycline 500 mg p os x 4/j x 14 j * Cotrimoxazole 80mg/400 mg x 2 x 2/j x 14 j* (WHO, 2004)")
89
GRANULOMA INGUINALE Doxycycline: 100 mg p os x 2/d x ≥3 weeks*
(DONOVANOSE) Doxycycline: 100 mg p os x 2/d x ≥3 weeks* Alternatives: Azithromycine: 1g p os x 1 j ≥3 weeks* OR Ciprofloxacine: 750 mg p os x 2/d x ≥3 weeks* Cotrimoxazole DS (800mg/160mg) p os x2/d x ≥3 weeks* * Up to complete healing (CDC,2006)
 Doxycycline: 100 mg p os x 2/d x ≥3 weeks* Alternatives: Azithromycine: 1g p os x 1 j ≥3 weeks* OR. Ciprofloxacine: 750 mg p os x 2/d x ≥3 weeks* Cotrimoxazole DS (800mg/160mg) p os x2/d x ≥3 weeks* * Up to complete healing. (CDC,2006)")
90
Hart G. Clinical Infectious Diseases 1997;25:24–32

98
Iconographie atlas

100
Fig. 1. Increases in risky behavior and the usage of antiretroviral therapy. (a) Relationship between antiretroviral usage, increases in risky behavior (in both infected and uninfected individuals) and HIV incidence rates after 5 years of antiretroviral usage. HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug resistance strains) are plotted, the data points show the area in which the HIV incidence rates are stable. The green, pink and blue data show prevalence one, 5 and 10 years, respectively, after the introduction of antiretroviral treatment Marie Laga, The synergy between Prevention and Care in Africa. IAS, Rio de Janeiro, 2005

103
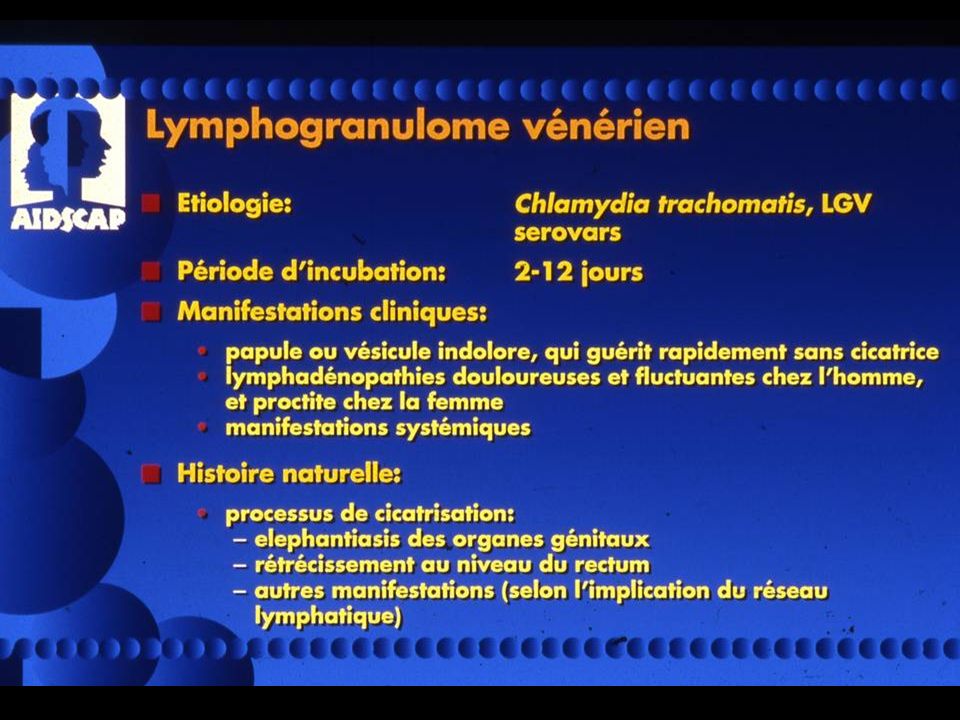
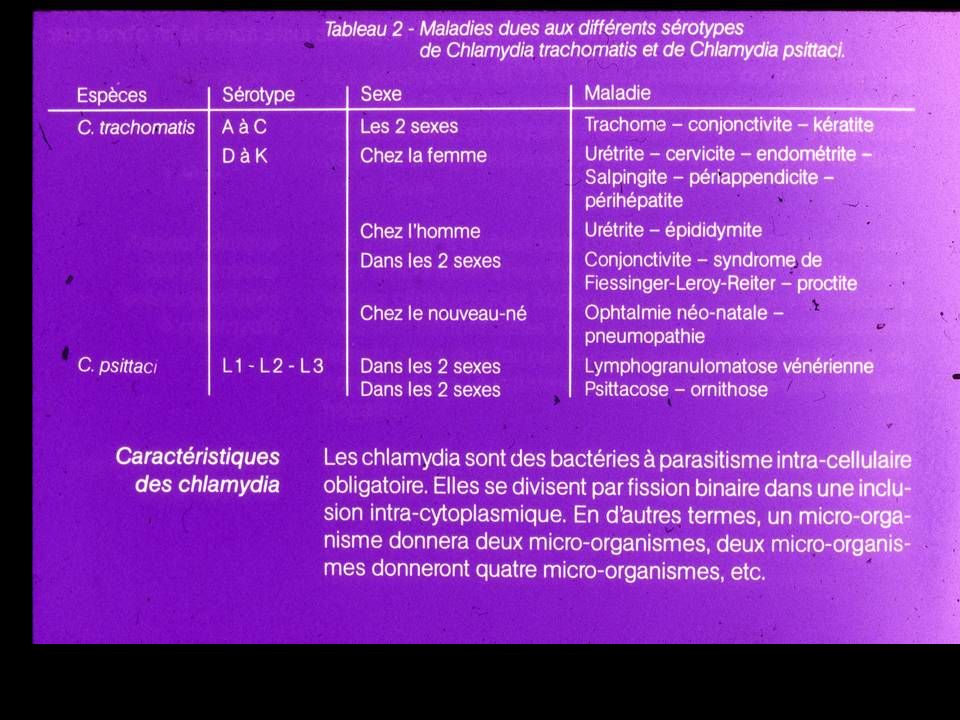
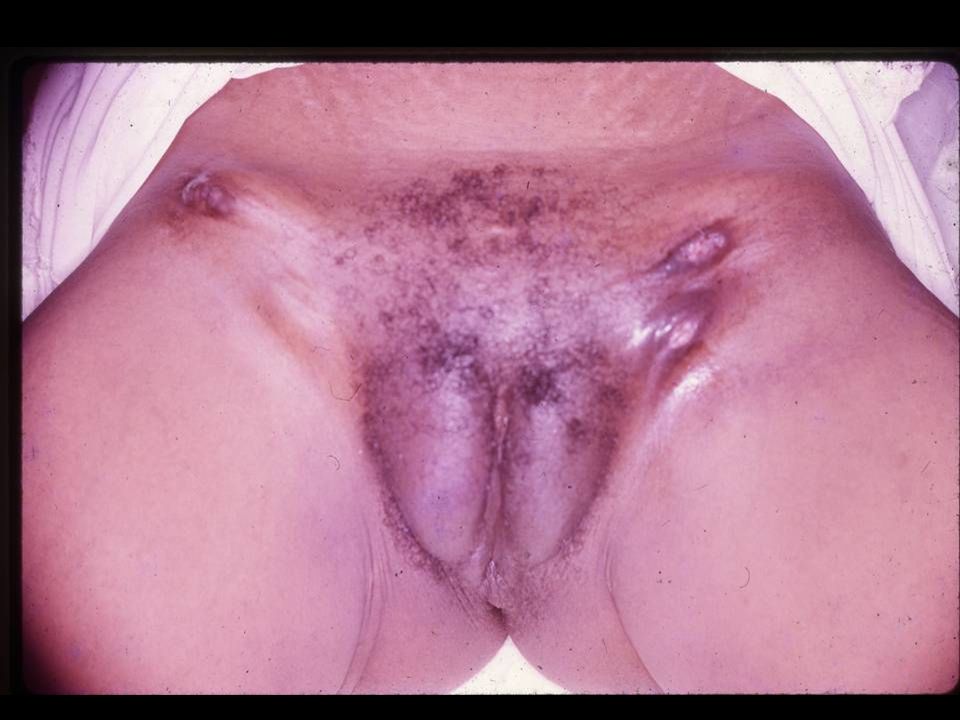
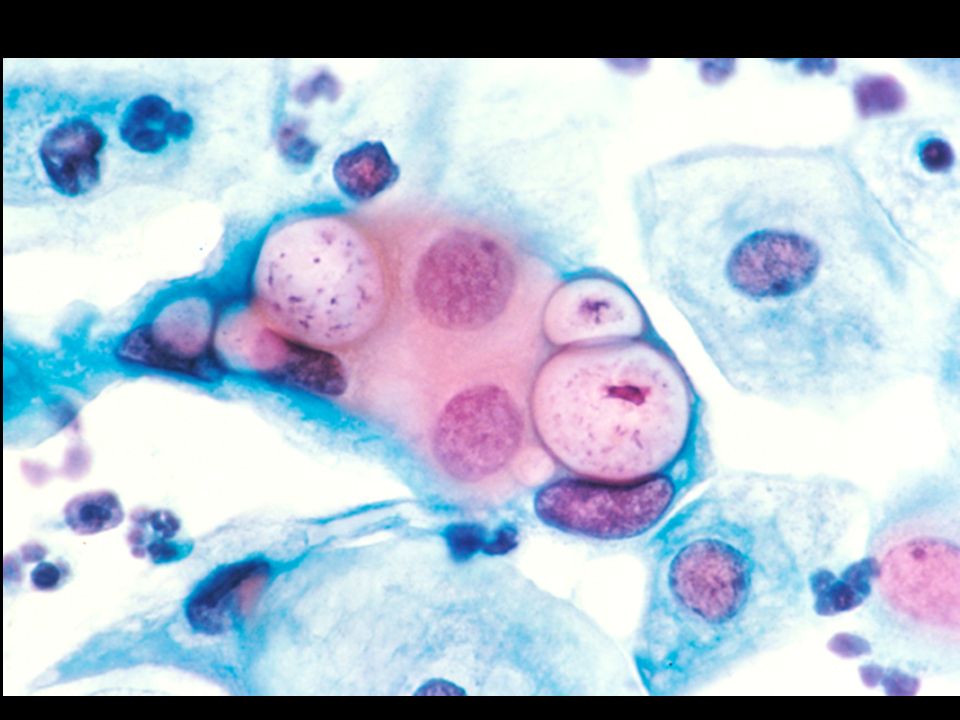
Lymphogranulomatose vénérienne
- fièvre - ténesme - écoulement purulent - adénopathie inguinale le plus souvent unilatérale, unique ou multiple, très inflammatoire avec risque de fistulisation - douleur ano-rectale sévère avec émission sanglante et muco-purulente, ténesme - proctite ou colo-proctite en rapport avec l'évolution de l'inflammation des ganglions lymphatiques péri-rectaux ou périanaux- muqueuse nodulaire et friable, ulcérations diffuses et superficielles

106
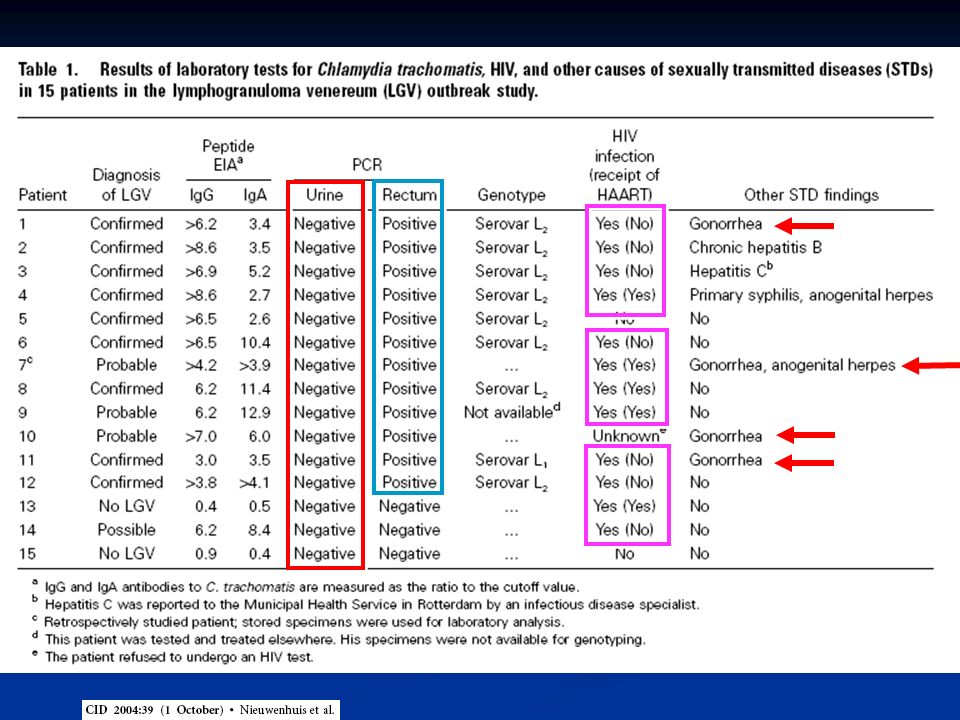
148 patients homo et bisexuels masculins
ayant consulté pour une ano-rectite sur une période de 29 mois (décembre mai 2005) Prélèvement ano-rectal +sérologie Chlamydia par micro-immunofluorescence 1er groupe:(n=26) LGAR (sérotype L2) 2ème groupe: (n=12) Chlamydioses anorectales (sérotype D à K ) 3 ème groupe:(n=110) Anorectites autres origines <256 512 1 1024 2 2048 4096 7 >8192 14 5 2 1 77 7 4 8 Titre des IgG anti-C. trachomatis chez LGAR >2048 chez 88,4% (23/26) Versus 25% (3/12) Chlamydiose anorectales Versus 20% (22/110) Ano-rectites autres origines
 Prélèvement ano-rectal +sérologie Chlamydia par micro-immunofluorescence. 1er groupe:(n=26) LGAR. (sérotype L2) 2ème groupe: (n=12) Chlamydioses anorectales. (sérotype D à K ) 3 ème groupe:(n=110) Anorectites autres origines. < > Titre des IgG anti-C. trachomatis chez LGAR >2048 chez 88,4% (23/26) Versus 25% (3/12) Chlamydiose anorectales. Versus 20% (22/110) Ano-rectites autres origines.")
107
LYMPHOGRANULOMA VENEREUM
(LGV) For 21 days Doxycycline mg p os x 2/d Alternative: Erythromycine 500mg p os x 4/d (CDC,2006)
 For 21 days. Doxycycline 100mg p os x 2/d. Alternative: Erythromycine 500mg p os x 4/d. (CDC,2006)")
108
LYMPHOGRANULOME VENERIEN
(Nicolas et Favre) Pendant 14 jours Doxycycline mg p os x 2 Ou Erythromycine 500mg p os x 4 Alternatives: Tetracycline mg p os x 4 (WHO, 2004)
 Pendant 14 jours. Doxycycline 100mg p os x 2. Ou. Erythromycine 500mg p os x 4. Alternatives: Tetracycline 500mg p os x 4. (WHO, 2004)")
111
Iconographie atlas

123
Chancre mou- une ou plusieurs ulcérations anales, purulentes- adénopathie inguinale inflammatoire évoluant vers la suppuration Bruno Halioua, Institut Alfred Fournier

124
Section MST de la Société Française de Dermatologie
LYMPHOGRANULOMATOSES ANORECTALES : A PROPOS DE 28 CAS DÉPISTÉS DANS UN CENTRE DE MST PARISIEN. B. Halioua (1), M. Herida (2), B. de Barbeyrac (3), P. Sednaoui (1) (1) Institut Alfred Fournier. Paris 75014 (2) INVS Saint Maurice. 94,(3) Centre Nationale de référence de Chlamydia Bordeaux. Section MST de la Société Française de Dermatologie
, M. Herida (2), B. de Barbeyrac (3), P. Sednaoui (1) (1) Institut Alfred Fournier. Paris (2) INVS Saint Maurice. 94,(3) Centre Nationale de référence de Chlamydia Bordeaux. Section MST de la Société Française de Dermatologie.")
125
Classic LGV (serotypes L1, L2, or L3
Bruno Halioua, Institut Alfred Fournier

126
Bruno Halioua, Institut Alfred Fournier

128
Bruno Halioua, Institut Alfred Fournier

129
Bruno Halioua, Institut Alfred Fournier

130
Bilan clinique: Tous les patients présentaient une anorectite sévère (22/28 soit 78% des cas), ulcéré(8/28). Diarrhée glairo-sanglante (8/28 soit 28%). Ecoulement purulent (11/28) Tenesmes (4/2_) 2 présentait un fébricule. 1 adénopathie fistulisée Bruno Halioua, Institut Alfred Fournier
. Ecoulement purulent (11/28) Tenesmes (4/2_) 2 présentait un fébricule. 1 adénopathie fistulisée. Bruno Halioua, Institut Alfred Fournier.")
131
Docteur Bruno Halioua Institut Alfred Fournier Paris 75014
MST ANO-RECTALES Docteur Bruno Halioua Institut Alfred Fournier Paris 75014

132
Herpes anal: Bruno Halioua, Institut Alfred Fournier

133
Condylomes acuminés Bruno Halioua, Institut Alfred Fournier

134
Condylomes acuminés Bruno Halioua, Institut Alfred Fournier

135
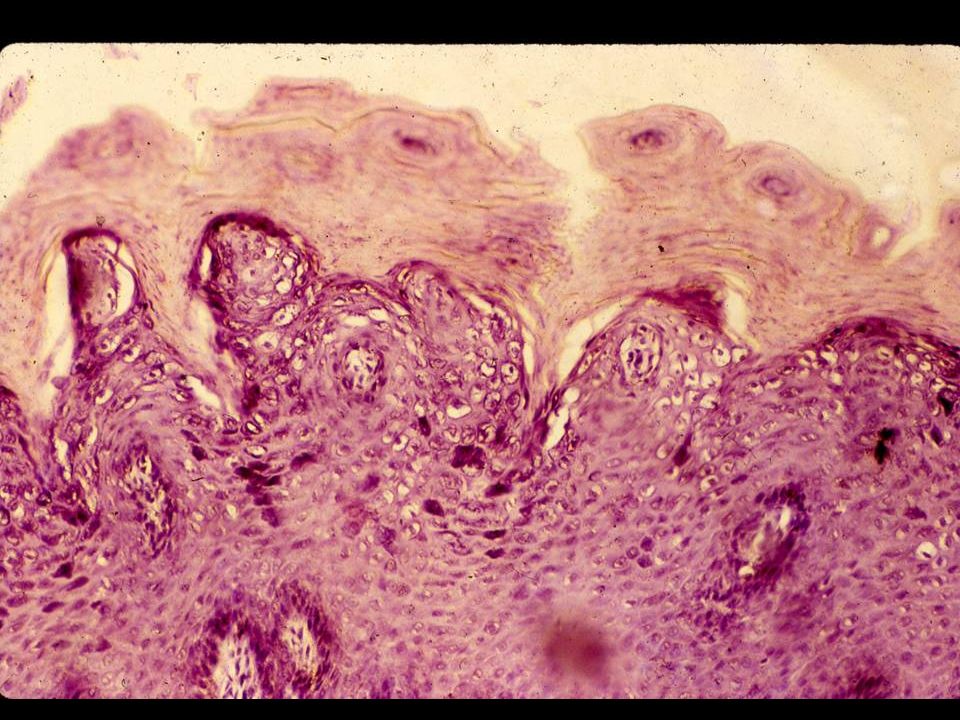
Anal intraepithelial neoplasia Histology
Bruno Halioua, Institut Alfred Fournier

136
Bruno Halioua, Institut Alfred Fournier

137
Bilan clinique: Tous les patients présentaient une anorectite sévère (22/28 soit 78% des cas), ulcéré(8/28). Diarrhée glairo-sanglante (8/28 soit 28%). Ecoulement purulent (11/28) Tenesmes (4/2_) 2 présentait un fébricule. 1 adénopathie fistulisée Bruno Halioua, Institut Alfred Fournier
. Ecoulement purulent (11/28) Tenesmes (4/2_) 2 présentait un fébricule. 1 adénopathie fistulisée. Bruno Halioua, Institut Alfred Fournier.")
138
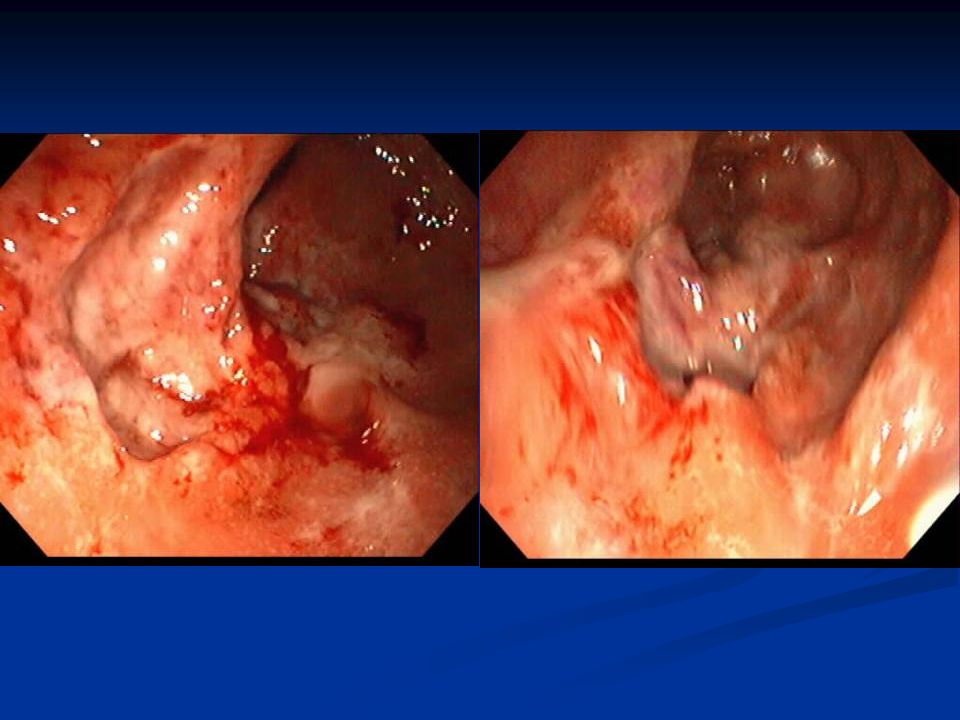
LES SYMPTÔMES SONT VARIABLES Douleurs abdominales Constipation
Diarrhée Ténesmes Épreintes Prurit anal Douleurs rectales Pertes anales muco-purulentes et sanglantes Fièvre Altération de l’état général LE TOUCHER RECTAL MUQUEUSE ÉPAISSIE, RIGIDE AVEC UN ASPECT GRANITÉ. Bruno Halioua, Institut Alfred Fournier

139
INTÉRÊT DANS LE DÉPISTAGE DES PATIENTS À RISQUE
Acceptabilité par les patients Chez les patients asymptomatiques: en cas de titre élevé > 2048 envisager un prélèvement ano-rectal sous anuscopie pour la recherche d’IST Chez les patients souffrant d’anorectites en cas de titre élevé > 2048 : Question que faire si recherche de Chlamydia trachomatis par PCR est négative? Biopsie étagées? Ig CT 2048 8 4096 >8192 7 Bruno Halioua, Institut Alfred Fournier

140
HSV-2 suppressive therapy to prevent HIV transmission
3646 HIV- discordant couples HSV-2 serology & CD4 testing of HIV+ partner Randomize HIV+/HSV2 + persons w/ CD4 > 250 Aciclovir 400 mg bid x 1 yr Placebo x 1 yr 1° endpoint: HIV infection in HIV-negative partners at 1 yr

141
1800 high-risk, HIV-/ HSV2+ MSM
Proof-of-concept trial of HSV-2 suppressive therapy to prevent HIV acquisition 1800 HIV-/ HSV2+ heterosexual women and 1800 high-risk, HIV-/ HSV2+ MSM Harare, Zimbabwe Lusaka, Zambia Johannesburg, SA Lima, Peru Seattle, USA San Francisco, USA New York, USA Randomize Aciclovir 400 mg bid x 1 yr Placebo x 1 yr 1° endpoint: HIV infection (estimated to be 3.5%/yr in placebo arm)
")
Présentations similaires














































>")







>")










