Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
A QUAND LES 3èmes LIGNES D’ARV EN AFRIQUE ?
ARV en Afrique : L’épreuve du temps 29 /11/2010 5’ rencontres Nord Sud Dr Roland Landman IMEA, SMIT Bichat Paris

2
INTRODUCTION (1) * Projections OMS 2010, 10% de PVVIH, traitement de 2nde ligne. Previsions OMS entre et patients VIH en première ligne d’ARV nécessitent un passage en deuxième ligne en 2010 * Recommandations 2006 et 2009 (OMS) traitement 2nde ligne 2NRTIs + IP/r * Recommandations décembre 2009 (OMS) traitement 3ème ligne Utilisation darunavir boosté par le ritonavir associé au raltégravir et/ou à l’etravirine si molécules disponibles dans les pays
 traitement 2nde ligne 2NRTIs + IP/r. * Recommandations décembre 2009 (OMS) traitement 3ème ligne. Utilisation darunavir boosté par le ritonavir associé au raltégravir et/ou à l’etravirine si molécules disponibles dans les pays.")
3
INTRODUCTION (2) Dans les pays ayant instauré la prescription des ARV à la fin des années les praticiens sont confrontés à la prise en charge de patients en échecs de deuxième ligne. - Le risque d’échec du traitement de seconde ligne est d’autant plus élevé que les critères de changement de traitement sont fondés sur la clinique et la numération des CD4 et non sur la charge virale plasmatique. - Retard dans le diagnostic de l’échec en général, une accumulation de résistances et la prescription d’une seconde ligne parfois suboptimale reposant sur une antiprotéase/r et des INRT prescrits en « backbone » parfois déjà résistants.

4
Retard au changement de traitement

5
11 cohortes Africaines , étude cas témoin mortalité après échec de première ligne
pts sous première ligne 2.33% passage en en deuxième ligne 1.9% maintien malgré un échec clinique ou immunologique Mortalité a un an: 4.2% chez les pts en seconde ligne vs 11.7% chez les pts maintenu en première ligne vs 2.2% chez les pts en succès de première ligne P< différence non expliquée par age, nadir de CD4 , ou différence de PDV Keiser et al Trop Med Int Health 2010 Feb

6
Mortalité à 6 mois sous seconde ligne
46% échec > 2nde ligne après1ère line. 1648 patients en 2nd ligne A total of 34 (5%) patients died and 23 (4%) were LFU. At 30 months of SLT death rate was 4/100 PY (95% CI 3-6) and attrition rate 8/100 PY (95% CI 6-10). (Figure 2) Mortality rates on SLT were higher in patients who met criteria of treatment failure. Death rates were lower in rural sites and in women. (Table 3) Table 3: Associations between mortality and selected factorsIn our programs, rates of failure on SLT were 46% higher than those observed in patients receiving first line therapy. Results were similar when using different definitions of treatment failure and when cohort attrition instead of death was examined (data not shown). Patients who met WHO criteria for failure on SLT were at increased risk of death. Strengthening and monitoring patient adherence to ART is specially important for SLT because regimen tolerability is worse than for first line treatment. To prevent deaths among HIV-infected patients, there is a need for increasing availability of new therapeutic options for patients living in RLC. Development of point of care diagnostic tools for early detection of suboptimal ART adherence is also essential. Taux d’échec (virologique, immunologique, ou clinique) M 30, 21/100 PY (95%CI 18-26) chez les patients sous seconde ligne ARV depuis au moins 6 mois. Pujades- Rodriguez M et al, JAMA 2010
 patients died and 23 (4%) were LFU. At 30 months of SLT death rate was 4/100 PY (95% CI 3-6) and attrition rate 8/100 PY (95% CI 6-10). (Figure 2) Mortality rates on SLT were higher in patients who met criteria of treatment failure. Death rates were lower in rural sites and in women. (Table 3) Table 3: Associations between mortality and selected factorsIn our programs, rates of failure on SLT were 46% higher than those observed in patients receiving first line therapy. Results were similar when using different definitions of treatment failure and when cohort attrition instead of death was examined (data not shown). Patients who met WHO criteria for failure on SLT were at increased risk of death. Strengthening and monitoring patient adherence to ART is specially important for SLT because regimen tolerability is worse than for first line treatment. To prevent deaths among HIV-infected patients, there is a need for increasing availability of new therapeutic options for patients living in RLC. Development of point of care diagnostic tools for early detection of suboptimal ART adherence is also essential. Taux d’échec (virologique, immunologique, ou clinique) M 30, 21/100 PY (95%CI 18-26) chez les patients sous seconde ligne ARV depuis au moins 6 mois. Pujades- Rodriguez M et al, JAMA")
8
TREAT Asia HIV observational Database
2446 patients : 447 échecs de première ligne , 7.8 pour 100 p/a ( immunologique, virologique ou clinique selon OMS) Seulement 52% ont changés au moins une molécule ARV après échec Zhou et al HIV Med 2010 janv.
 Seulement 52% ont changés au moins une molécule ARV après échec. Zhou et al HIV Med 2010 janv.")
9
Résistances aux ARV Au Malawi, 397 patients ont été traités par d4T/3TC/NVP pendant 9.5 mois en médiane. L’analyse virologique montre que parmi les 50 patients qui sont en échec virologique, 94% ont un virus résistant à EFV/NVP, 76% à la 3TC, 12% à AZT/d4T et 10% au TDF . Ferradini et al: Lancet 2006;367(9519): Dans la cohorte DART conduite en Afrique australe et de l’Est, la proportion de patients dont les virus étaient porteurs de mutations de résistance aux analogues de la thymidine (TAMs) est passé de 4% après 12 mois de traitement à 39% après 24 mois. Ndembi et al: J.infect Dis. 2010;201(1):106-13 En Cote d’Ivoire a 12 mois de traitement sur 1545 patients ayant debuté un traitement par d4T ou ZDV+3TC+NVP ou EFV, sur les 941 vivants. 232 patients (25%) ont une charge virale détectable, avec 51% ayant au moins une mutation de resistance (resistance aux NNRTI 91.5%, à 3TC/FTC 69% et à ZDV et/ou d4T 9.4%). Messou et al CROI 2010 abstract 587
: Dans la cohorte DART conduite en Afrique australe et de l’Est, la proportion de patients dont les virus étaient porteurs de mutations de résistance aux analogues de la thymidine (TAMs) est passé de 4% après 12 mois de traitement à 39% après 24 mois. Ndembi et al: J.infect Dis. 2010;201(1): En Cote d’Ivoire a 12 mois de traitement sur 1545 patients ayant debuté un traitement par d4T ou ZDV+3TC+NVP ou EFV, sur les 941 vivants. 232 patients (25%) ont une charge virale détectable, avec 51% ayant au moins une mutation de resistance (resistance aux NNRTI 91.5%, à 3TC/FTC 69% et à ZDV et/ou d4T 9.4%). Messou et al CROI 2010 abstract 587.")
10
Low levels of antiretroviral resistant HIV infection in Cameroon that use the WHO public health approach to monitor ART and adequacy with the WHO recommendation for second line therapy Kouanfack C, CID 2009

11
Hosseinipour MC, AIDS 2009

12
150 000 pts sous d4T/3TC/NVP au Malawi depuis 2001
periode d’observatiion de 18 mois Criitères échec OMS ( baisse CD4, Stade 4) CV < 1000 c/ml : génotype 203 pts suspicon clinique et immunologique d’échec : 88: cv < 400 c/mL, 6: c/mL 96 patients Mutations NNRTIs 93% M184V 81% K65R ou K70E 23% Analyse phénotypique sur 70 virus : 61% sensible au TDF, 37% AZT, 37% d4T, ABC 33% et ddI 1%. en faveur que le meilleur backbone de NRTIs pour un traitement ultérieur : AZT/3TC/TDF > TDF/3TC > ABC/ddI Hosseinnipour MC et al AIDS 2009
 CV < 1000 c/ml : génotype. 203 pts suspicon clinique et immunologique d’échec : 88: cv < 400 c/mL, 6: c/mL. 96 patients. Mutations NNRTIs 93% M184V 81% K65R ou K70E 23% Analyse phénotypique sur 70 virus : 61% sensible au TDF, 37% AZT, 37% d4T, ABC 33% et ddI 1%. en faveur que le meilleur backbone de NRTIs pour un traitement ultérieur : AZT/3TC/TDF > TDF/3TC > ABC/ddI. Hosseinnipour MC et al AIDS")
13
M184V 72% K65R 4% NNRTIs mutations 23% Y181C NVP 26%
226 pts en échecs de première ligne en Afrique du Sud M184V % K65R % NNRTIs mutations % Y181C NVP 26% EF V 3% p < 0.001 Wallis et al, JAIDS 2010 April

14
Cinétiques d’acquisition de la résistance lors d’échecs virologiques= 3 comportements différents (Clavez V. )
.")
15
Contexte Côte d’Ivoire
Contexte Dakar La file active de Dakar est de 2500 patients. A titre d’exemple sur les 230 patients encore suivis dans la cohorte 1215 la moitié ont déjà reçu un INNTI et une IP et 10% ont une charge virale > 1000 c/mL. Contexte Côte d’Ivoire Décembre 2008, environ 5000 patients sous antiprotéases dont 98% en traitement de seconde ligne ou plus. 1-5%, le nombre de patients en échec de la seconde ligne .

16
Traitement de seconde ligne
Recommandations OMS 2010 Traitement de seconde ligne TDF ATV/RTV 3TC/FTC AZT LPV/RTV

17
3eme ligne d’ARV Les données manquantes dans les pays a faibles ressources
1- le profil de résistance des personnes en échec de 2ème ligne de traitement 2- la réponse virologique à un traitement de troisième ligne d’antirétroviraux 3- le profil d’adhérence des personnes à un régime de 3ème ligne 4- les enjeux de coût et de coût-efficacité.

18
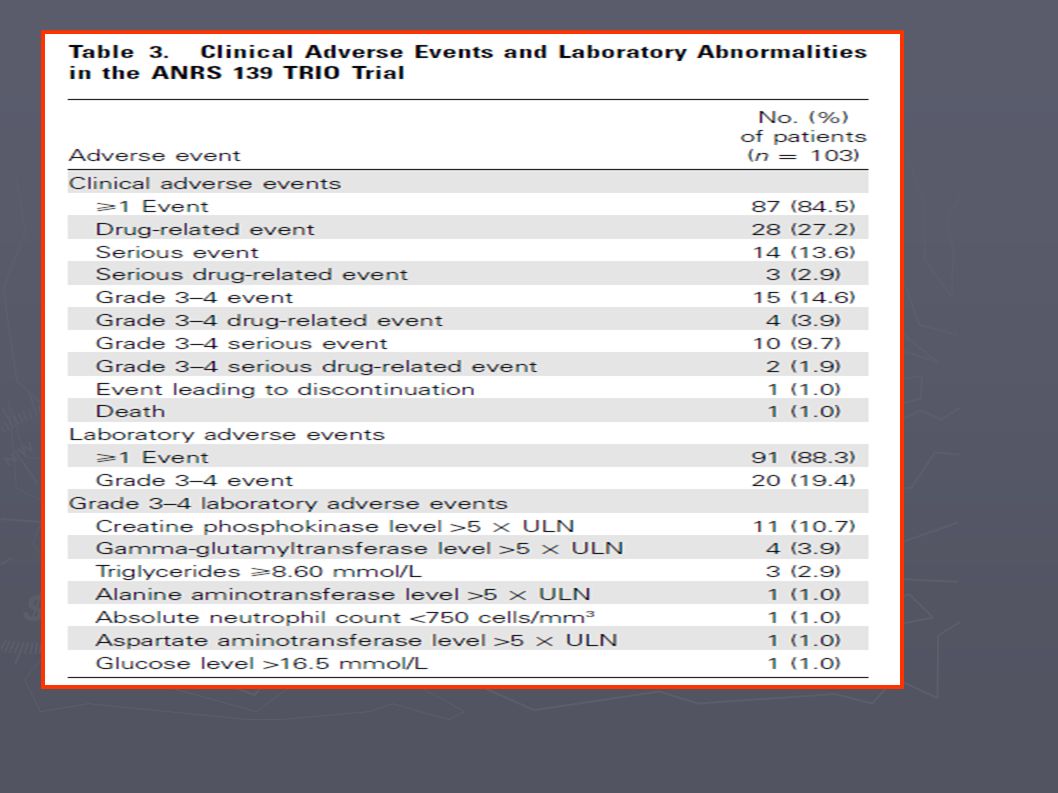
1) Succès virologique du traitement 3ème ligne si combinaison de deux molécules jamais utilisées par le patient - Darunavir (essais Power 1 et 2, De Meyer S, JAIDS 2008) - Raltégravir (Benchmark, Steigbigel RT, NEJM 2008, CID 2010) - Etravirine patients pré-exposés INNTIs, < 3 RAMS (Katlama C (DUET 1 et 2, AIDS 2009) 4) Darunavir + Raltégravir + Etravirine ( Essai ANRS Trio, Y Yazdanpanah CID 2009) Patients en multi-échecs
 Succès virologique du traitement 3ème ligne si combinaison de deux molécules jamais utilisées par le patient - Darunavir (essais Power 1 et 2, De Meyer S, JAIDS 2008) - Raltégravir (Benchmark, Steigbigel RT, NEJM 2008, CID 2010) - Etravirine patients pré-exposés INNTIs, < 3 RAMS (Katlama C (DUET 1 et 2, AIDS 2009) 4) Darunavir + Raltégravir + Etravirine ( Essai ANRS Trio, Y Yazdanpanah CID 2009) Patients en multi-échecs")
20
Third-line regimens 1. National programmes should develop policies for third-line therapy that consider funding, sustainability and the provision of equitable access to ART. (Conditional recommendation, low quality of evidence) 2. Third-line regimens should include new drugs likely to have anti HIV activity such as integrase inhibitors and second generation NNRTIs and PIs. 3. Patients on a failing second-line regimen with no new ARV options, should continue with a tolerated regimen. (Conditional recommendation, very low quality of evidence) Remarks: The panel were concerned by unpublished cohort reports of high mortality among patients failing second-line therapy, but placed high value on balancing the need to develop policies for third-line therapy whilst maintaining increased access to first-line therapy.
 2. Third-line regimens should include new drugs likely to have. anti HIV activity such as integrase inhibitors and second. generation NNRTIs and PIs. 3. Patients on a failing second-line regimen with no new ARV. options, should continue with a tolerated regimen. (Conditional recommendation, very low quality of evidence) Remarks: The panel were concerned by unpublished cohort reports of. high mortality among patients failing second-line therapy, but placed. high value on balancing the need to develop policies for third-line. therapy whilst maintaining increased access to first-line therapy.")
21
Accès aux ARV , si vous pouvez vous l’offrir……
Et si la dernière décennie de scaling-up rapide n’était qu’un mirage passager?

22
Comparaison des prix des combinaisons ARV en fonction des lignes de traitements

23
Manufacturer, price, Distribution third line drugs in developing countries (source UTW 2010)
Distributor Darunavir Tibotec US$ 1095 ppy Aspen. For sub-saharan african (SSA) countries and least developed countries. No fixed/reduced price for middle income countries Ritonavir Abbott US$ 83 ppy Price for Africa and Least Developed Countries only Raltegravir Merck US$ 1113 ppy Specific list of countries Etravirine US$ 913 ppy No regulatory approvals yet in SSA. Pre-approval access program managed by Aspen Pharmacare for SSA. Total US$ 3204 ppy
 countries and least developed countries. No fixed/reduced price for middle income countries. Ritonavir. Abbott. US$ 83 ppy. Price for Africa and Least Developed Countries only. Raltegravir. Merck. US$ 1113 ppy. Specific list of countries. Etravirine. US$ 913 ppy. No regulatory approvals yet in SSA. Pre-approval access program managed by Aspen Pharmacare for SSA. Total. US$ 3204 ppy.")
24
Registration dossiers for darunavir 300mg have been filed in 18 SSA countries. We have received approval for darunavir in Botswana, the Democratic Republic of Congo, Ghana, Namibia, Kenya, Senegal, Tanzania, Uganda and Zambia; the product is also readily accessible in Rwanda and Swaziland The first registration dossiers for etravirine have been submitted in Botswana, Burkina Faso, Kenya, Senegal, South Africa, Uganda and Zambia. Tibotec

25
Licenses sur ARV

27
The Indian Patent Office (IPO) has rejected applications from two U. S
The Indian Patent Office (IPO) has rejected applications from two U.S. pharmaceutical companies , raising hopes of a further lowering of prices of two life-saving drugs used by HIV/AIDS patients in the country. Septe 2009 The HINDU
 has rejected applications from two U.S. pharmaceutical companies , raising hopes of a further lowering of prices of two life-saving drugs used by HIV/AIDS patients in the country. Septe 2009 The HINDU.")
28
The treatment timebomb
Report of the inquiry of the All Party Parliamentary Group on AIDS into long-term access to HIV medicines in the developing world. London: 2009 Jul.

29
ARV de 3eme ligne (1) Darunavir: BID chez les prétraités
Efficace après résistance aux IP de première ligne Peu d’expérience au sud, approuvé dans 9 pays africains Raltegravir: BID, OAD en cours d’évaluation Pas de données dans les pays du sud Prix 1113 $/an pour 59 pays, mais enregistré dans 9 Etravirine; Efficacité persistante après résistance NVP et EFV? OAD en cours d’evauation, probablement efficace Rash 9%, hepatotoxicité < NVP Cmin diminuee en présence rifampicine et rifabutine Pas d’experience au sud

30
ARV de 3eme ligne (2) Rilpivirine:
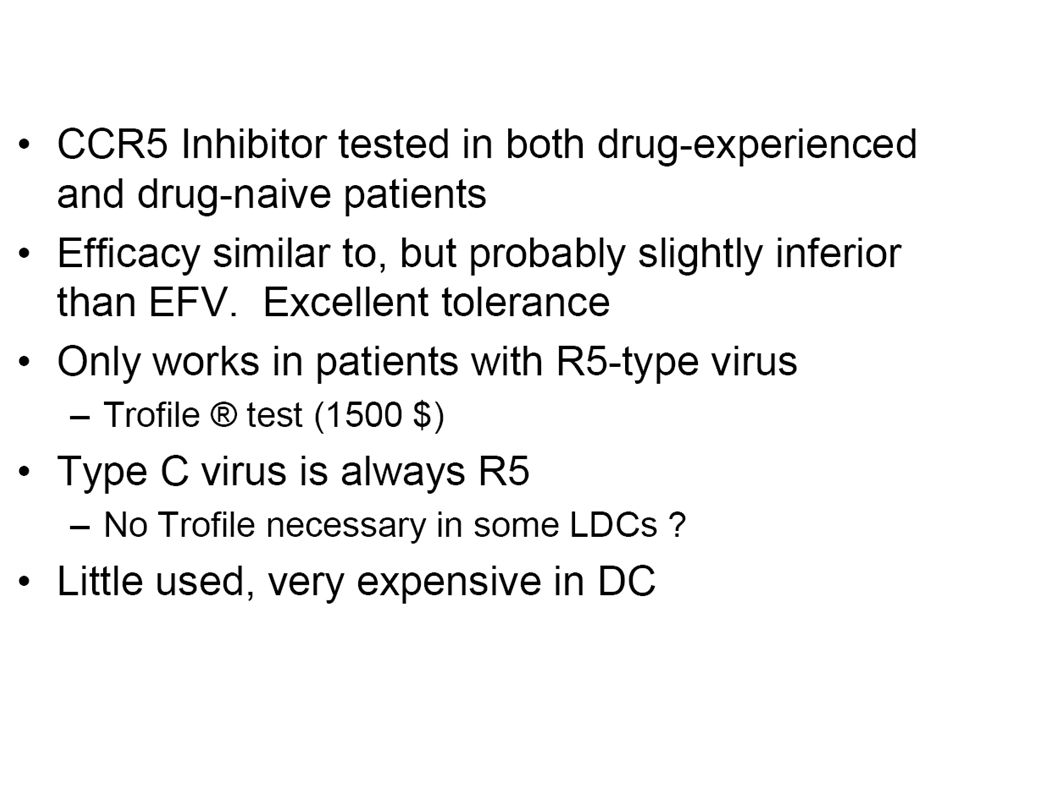
Efficacité persistante après résistance NVP et EFV? Peu d’intolérence sur le SNC Risque de mutations sur les NRTIs > EFV Traitement combiné avec TDF/FTC un comprimé OAD en cours de développement, fin 2011? Pas d’expérience au sud Maraviroc: Efficacité legèrement < EFV Très bonne tolérance Necessité d’un test trophil cher++ ou génotype Sous Type C toujours R5 Pas d’experience au sud

31
Prise en charge des situations d’échec virologique Possibilité de proposer un nouveau schéma actif
Situation optimale = Construire un schéma comportant de préférence 3 ARV actifs sur la base de l’historique thérapeutique et du génotype cumule (AII) Privilégier si possible les combinaisons évaluées dans des essais cliniques Situation de multirésistance Présence d’une résistance aux 3 classes historiques, avec multirésistance aux INTI (≥ 3 TAM + 184V ou K65R + 184V), résistance aux INNTI et mutation(s) majeure(s) de résistance aux IP Objectif idéal = Association de 3 ARV actifs devant comporter 1 IP/r actif (DRV/r ou TPV/r), associé à 2 autres ARV complètement actifs dont : Etravirine Raltegravir : Impératif d’associer au RAL au moins 2 ARV actifs (cf risque élevé (> 80 %) de mutations en cas d’échec virologique) Maraviroc : Si absence de virus de tropisme X4 ou dual/mixte Enfuvirtide : Inconvénient de l’administration sous-cutanée biquotidienne 1 ou plusieurs INTIs Si multi-résistance aux INTIs (≥ 3 TAM + 184V), persistance possible d’une activité résiduelle de ABC et surtout de TDF Maintien d’INTIs en cas de multirésistance à cette classe d’ARV probablement non justifié, si d’autres ARV pleinement actifs disponibles Présence d’INTIs dans tous les essais cliniques réalisés avec les nouveaux ARV de 2002 à 2009 => Possible contribution des INTIS à l’efficacité observée Maintien de 3TC ou FTC, en présence de mutation M184V, peut être envisagé Association de 2 IP/r non recommandée (AII)
 Privilégier si possible les combinaisons évaluées dans des essais cliniques. Situation de multirésistance. Présence d’une résistance aux 3 classes historiques, avec multirésistance aux INTI (≥ 3 TAM + 184V ou K65R + 184V), résistance aux INNTI et mutation(s) majeure(s) de résistance aux IP. Objectif idéal = Association de 3 ARV actifs devant comporter 1 IP/r actif (DRV/r ou TPV/r), associé à 2 autres ARV complètement actifs dont : Etravirine. Raltegravir : Impératif d’associer au RAL au moins 2 ARV actifs (cf risque élevé (> 80 %) de mutations en cas d’échec virologique) Maraviroc : Si absence de virus de tropisme X4 ou dual/mixte. Enfuvirtide : Inconvénient de l’administration sous-cutanée biquotidienne. 1 ou plusieurs INTIs. Si multi-résistance aux INTIs (≥ 3 TAM + 184V), persistance possible d’une activité résiduelle de ABC et surtout de TDF. Maintien d’INTIs en cas de multirésistance à cette classe d’ARV probablement non justifié, si d’autres ARV pleinement actifs disponibles. Présence d’INTIs dans tous les essais cliniques réalisés avec les nouveaux ARV de 2002 à 2009 => Possible contribution des INTIS à l’efficacité observée. Maintien de 3TC ou FTC, en présence de mutation M184V, peut être envisagé. Association de 2 IP/r non recommandée (AII)")
32
Prise en charge des situations d’échec virologique Possibilité de proposer un nouveau schéma actif
Situation de multirésistance (suite) Aucun ou au maximum un seul médicament actif Préférable d’éviter d’utiliser la seule molécule active restante (même si seule classe non utilisée) Avis spécialisé fortement recommandé et possibilité pour ces patients d’accéder à des molécules en développement ( cf essais cliniques) Si CD4 > 200/mm3, et génotype avec résistance a l’ensemble des ARV : Recommandé de ne pas modifier le traitement, en surveillant les CD4, la survenue de manifestations cliniques et en pesant le risque de voir s’accumuler des mutations de résistance supplémentaires Si CD4 < 200/mm3, avec risque de progression clinique Optimiser le traitement en recyclant les ARV déjà utilisées, et en les associant Considérer l’ensemble des ARV déjà utilisés ou supposés d’activité limitée, et maintenir les ARV ayant une activité résiduelle ou diminuant la capacité réplicative (3TC, FTC) Adapter les doses des IP/r, (cf dosages plasmatiques, et concept de GIQ). CV < cp/ml associée a un moindre risque de progression ou de décès, ou de chute des CD4 Si CD4 < 100/mm3, et risque élevé de progression clinique Réduction du risque par addition d’une seule molécule Gagner du temps pour bénéficier ultérieurement d’un nouveau schéma thérapeutique comportant 2 molécules actives (si développement dans des délais raisonnables) Mettre en balance le bénéfice même marginal du maintien d’un traitement ARV non optimal et le risque d’accumulation de mutations de résistance
 Aucun ou au maximum un seul médicament actif. Préférable d’éviter d’utiliser la seule molécule active restante (même si seule classe non utilisée) Avis spécialisé fortement recommandé et possibilité pour ces patients d’accéder à des molécules en développement ( cf essais cliniques) Si CD4 > 200/mm3, et génotype avec résistance a l’ensemble des ARV : Recommandé de ne pas modifier le traitement, en surveillant les CD4, la survenue de manifestations cliniques et en pesant le risque de voir s’accumuler des mutations de résistance supplémentaires. Si CD4 < 200/mm3, avec risque de progression clinique. Optimiser le traitement en recyclant les ARV déjà utilisées, et en les associant. Considérer l’ensemble des ARV déjà utilisés ou supposés d’activité limitée, et maintenir les ARV ayant une activité résiduelle ou diminuant la capacité réplicative (3TC, FTC) Adapter les doses des IP/r, (cf dosages plasmatiques, et concept de GIQ). CV < cp/ml associée a un moindre risque de progression ou de décès, ou de chute des CD4. Si CD4 < 100/mm3, et risque élevé de progression clinique. Réduction du risque par addition d’une seule molécule. Gagner du temps pour bénéficier ultérieurement d’un nouveau schéma thérapeutique comportant 2 molécules actives (si développement dans des délais raisonnables) Mettre en balance le bénéfice même marginal du maintien d’un traitement ARV non optimal et le risque d’accumulation de mutations de résistance.")
33
Durée médiane sous ARV, 13 ans

34
Stratégies de traitement de troisième ligne, infection à VIH-1
Etravirine (< 3 RAMS) TRIO Darunavir Raltegravir + + (NRTI) TDF +FTC? ABC + DDI?
 TRIO. Darunavir. Raltegravir. + + (NRTI) TDF +FTC ABC + DDI")
35
Stratégies de traitement de troisième ligne ?
Darunavir monotherapie? (NRTI) TDF +FTC? ABC + DDI? + Darunavir + Maraviroc ? Etravirine (< 3 RAMS) +
 TDF +FTC ABC + DDI + Darunavir + Maraviroc Etravirine. (< 3 RAMS) +")
36
MINISTERE DE LA LUTTE CONTRE LE SIDA
Cohorte de patients sous traitement antirétroviral de troisième ligne sur les sites ANRS : Cohorte SAVELINC (Salvage Therapy in Low Income Countries) soumission 15/9/2010 Serge Paul Eholié Service des Maladies Infectieuses et Tropicales Pac-ci/site ANRS de Côte d’Ivoire Roland Landman Institut de Médecine d’Epidémiologie Appliquée MINISTERE DE LA LUTTE CONTRE LE SIDA
 soumission 15/9/2010. Serge Paul Eholié. Service des Maladies Infectieuses et Tropicales. Pac-ci/site ANRS de Côte d’Ivoire. Roland Landman. Institut de Médecine d’Epidémiologie Appliquée. MINISTERE DE LA LUTTE CONTRE LE SIDA.")
37
Stratégies de l’étude Difficultés à obtenir des tests génotypiques en routine, intérêt évaluation stratégies thérapeutiques et élaboration algorithme thérapeutique décisionnel, utilisant darunavir + raltegravir Absence de tests génotypiques pour choix des INTIS Combinaison thérapeutique à base de darunavir + raltégravir. Choix des autres molécules (etravirine, ou NRTI(s) « recyclé(s) » ou non utilisés/ libre appréciation des investigateurs des sites.
 « recyclé(s) » ou non utilisés/ libre appréciation des investigateurs des sites.")
38
Equipes Projet Savelink
INVESTIGATEURS COORDONATEURS SUD Pr Serge EHOLIE NORD Dr Roland LANDMAN EQUIPE A (Cote d’Ivoire) EQUIPE B( Sénégal) EQUIPE C( IMEA- Paris-France) Investigateurs: Pr E. Bissagnéné Dr C. Danel Dr X. Anglaret Dr E. Ouattara Investigateurs Cliniciens: Dr I. Ouattara Dr E. Messou Statistique: D. Gabillard Biologie: Dr T. Thomas Dr Y. Vincent Investigateurs: Pr PS. Sow Dr F. Ngome Dr I. N’doye Médecin d’étude clinique: Dr MB. Diallo Attachée de Recherche Clinique: Mme S. Legac Biologie: Pr S. Mboup Dr C. Touré Kane Président du CS Pr P-M. Girard Coordination de l’essai Mme A. Benalycherif EQUIPE E( Modélisation) Pr Y. Yazdanpanah Pr K. Freedberg Dr X .Anglaret Dr E. Ouattara EQUIPE D( Coordination virologique- Paris-France) Dr ML. Chaix Dr J. Ghon
 EQUIPE B( Sénégal) EQUIPE C( IMEA- Paris-France) Investigateurs: Pr E. Bissagnéné. Dr C. Danel. Dr X. Anglaret. Dr E. Ouattara. Investigateurs Cliniciens: Dr I. Ouattara. Dr E. Messou. Statistique: D. Gabillard. Biologie: Dr T. Thomas. Dr Y. Vincent. Investigateurs: Pr PS. Sow. Dr F. Ngome. Dr I. N’doye. Médecin d’étude clinique: Dr MB. Diallo. Attachée de Recherche Clinique: Mme S. Legac. Biologie: Pr S. Mboup. Dr C. Touré Kane. Président du CS. Pr P-M. Girard. Coordination de l’essai. Mme A. Benalycherif. EQUIPE E( Modélisation) Pr Y. Yazdanpanah. Pr K. Freedberg. Dr X .Anglaret. Dr E. Ouattara. EQUIPE D( Coordination virologique- Paris-France) Dr ML. Chaix. Dr J. Ghon.")
40
HYPOTHÈSES DE L’ÉTUDE 1) Peu de données sur les patients en échecs de 2e ligne en Afrique SS 2) Risque d’augmentation rapide du nombre d’adules en échecs de 2e ligne: - absence de monitoring virologique; - retard à l’initiation du traitement de seconde ligne; - accumulation TAMS et NAMS; 3) Succès virologique du traitement 3ème ligne si combinaison de deux molécules jamais utilisées par le patient; - Darunavir (essais Power 1 et 2, De Meyer S, JAIDS 2008, - Raltégravir (Benchmark, Steigbigel RT, NEJM 2008, CID 2010) - Etravirine patients pré-exposés INNTIs, < 3 RAMS (Katlama C (DUET 1 et 2, AIDS 2009) 4) Darunavir + Raltégravir + Etravirine ( Essai Trio, Y Yazdanpanah CID 2009) Patients en multi-échecs (France)
 Peu de données sur les patients en échecs de 2e ligne en Afrique SS 2) Risque d’augmentation rapide du nombre d’adules en échecs de 2e ligne: - absence de monitoring virologique; - retard à l’initiation du traitement de seconde ligne; - accumulation TAMS et NAMS; 3) Succès virologique du traitement 3ème ligne si combinaison de deux molécules jamais utilisées par le patient; - Darunavir (essais Power 1 et 2, De Meyer S, JAIDS 2008, - Raltégravir (Benchmark, Steigbigel RT, NEJM 2008, CID 2010) - Etravirine patients pré-exposés INNTIs, < 3 RAMS (Katlama C (DUET 1 et 2, AIDS 2009) 4) Darunavir + Raltégravir + Etravirine ( Essai Trio, Y Yazdanpanah CID 2009) Patients en multi-échecs (France)")
42
Difficulté de mise en œuvre des traitements de troisième ligne
* Profil de résistance des personnes en échec de 2ème ligne de traitement inconnu dans ce contexte ; * Réponse virologique sous cette association d’antirétroviraux dans ce contexte; * Profil d’adhérence de ces personnes à un régime de 3ème ligne ; * enjeux de cout et de cout-efficacité * Formation des praticiens (cliniciens, biologistes, pharmaciens) * Importance de documenter et évaluer des stratégies de troisième ligne en PED pour renforcer le plaidoyer
 * Importance de documenter et évaluer des stratégies de troisième. ligne en PED pour renforcer le plaidoyer.")
44
Actuellement, très peu de données sont disponibles sur les patients en échec de 2ième ligne de traitement en Afrique Subsaharienne, notamment sur la proportion de patients en échec virologique et le profil de résistance génotypique des virus. Le nombre d’adultes en échec de 2ième ligne augmente rapidement, en raison de l’absence de suivi virologique en routine, du retard à l’initiation du traitement de 2ième ligne et de l’accumulation de TAMs et NAMs (même si à ce jour les patients suivis dans les cohortes ont surtout développé des TAMs). L’utilisation du génotype en technique de routine ne semble pas raisonnable ni même justifiée au Sud. L’OMS recommande en 2009, une 3ième ligne de traitement utilisant DRV/r associé au RAL et/ou étravirine, mais cette recommandation n’est pas réellement appliquée. Compte tenu de l’exposition potentiellement prolongée aux INNTIs chez les patients en échec de 1ère ligne avant le switch en 2ième ligne, les investigateurs ne sont pas favorables à l’utilisation de l’étravirine dans l’arsenal thérapeutique de 1ère intention. L’association DRV/r et raltegravir semble donc être le 1er choix des investigateurs, le DRV étant l’inhibiteur de protéase dont l’activité est la plus constante sur des souches résistantes aux inhibiteurs de protéase de 1ère génération (et notamment au LPV/r). L’utilisation du DRV protègera contre le risque de sélection de souches résistantes au RAL, dont les avantages sont ceux d’une nouvelle classe thérapeutique mais dont la faiblesse est une barrière génétique relativement faible.
. L’utilisation du génotype en technique de routine ne semble pas raisonnable ni même justifiée au Sud. L’OMS recommande en 2009, une 3ième ligne de traitement utilisant DRV/r associé au RAL et/ou étravirine, mais cette recommandation n’est pas réellement appliquée. Compte tenu de l’exposition potentiellement prolongée aux INNTIs chez les patients en échec de 1ère ligne avant le switch en 2ième ligne, les investigateurs ne sont pas favorables à l’utilisation de l’étravirine dans l’arsenal thérapeutique de 1ère intention. L’association DRV/r et raltegravir semble donc être le 1er choix des investigateurs, le DRV étant l’inhibiteur de protéase dont l’activité est la plus constante sur des souches résistantes aux inhibiteurs de protéase de 1ère génération (et notamment au LPV/r). L’utilisation du DRV protègera contre le risque de sélection de souches résistantes au RAL, dont les avantages sont ceux d’une nouvelle classe thérapeutique mais dont la faiblesse est une barrière génétique relativement faible.")
45
© Jonathan Heyer/MSF “The number of people needing HIV treatment will rise over the next two decades and so will the cost of treatment. This is because better, more effective treatments have come on the market and should be offered to patients, and also because, over time, more people will move from first to second (and later) line regimens, which are more expensive.” -- The Treatment Timebomb -- Report of the Enquiry of the UK All Party Parliamentary Group on AIDS4 There is a growing disconnect between the AIDS treatment available to people in developed countries and to their counterparts in developing countries. In wealthy countries, AIDS now resembles a chronic disease, much like heart disease or diabetes, and patients generally have access to an increasing variety of treatment options once they inevitably develop drug resistance. 5 In contrast, people living with HIV/AIDS in developing countries largely have access to only one combination of medicines that causes significant side effects, with few or no alternatives for when their treatment fails. And the youngest people living with AIDS continue to be an afterthought – paediatric treatment still lags behind that for adults, as does the development of appropriate ARVs for children. If people living with HIV/AIDS are to be given the same prospects for survival whether they live in developing countries or in wealthy countries, urgent action must be undertaken to ensure access: · to a less toxic first-line regimen; · to second- and third-line treatment options as patients develop resistance; · better and timely detection of treatment failure through increased access to viral load testing, and · to paediatric AIDS treatment options, which must be prioritised together with the prevention of mother-to-child transmission of the virus. A) Move to a less-toxic and more robust first-line regimen The first line of defence to help slow the pace at which patients need to switch to newer, more expensive ARV treatment regimens is a robust first-line drug combination with few side effects. Today, the majority of people on their first-line of ARVs in low- and middle-income countries receive the combination of lamivudine/stavudine/ nevirapine (3TC/d4T/NVP).6 Thanks to generic competition, this regimen now costs US$ 67 per patient per year (ppy) – 99% less than 10 years ago. This dramatic price drop was possible because of competition among multiple generic manufacturers in countries where these drugs were not patented, such as Brazil, Thailand and India (see graph 1). Notwithstanding the dramatic price drop over the past decade, using this standard combination comes at a high medical cost. The drug stavudine (d4T) causes serious side effects, some intolerable, such as peripheral neuropathy. It can also lead to lactic acidosis, which in rare cases can lead to death. It also causes stigmatisation because over long-term treatment, patients develop easily recognisable facial wasting. **Graph 1: Competition as a catalyst for price reductions** The fall in the price of first-line combinations of stavudine (d4T), lamivudine (3TC), and nevirapine (NVP), since 2000. Stavudine is virtually no longer used in wealthy countries (in 2006, for example, fewer than 2% of patients in Switzerland were taking the drug7). Patients in these countries are offered better-tolerated alternatives, such as tenofovir (TDF) or zidovudine (AZT). Since 2006, WHO has recommended in its HIV/AIDS treatment guidelines that treatment providers begin moving away from stavudine-based regimens because of their long-term irreversible side effects, towards tenofovir or zidovudine-containing regimens.8 This call was repeated in the latest recommendations released by WHO in December 2009 for ART for HIV in adults and adolescents, advising countries to develop a plan to move towards tenofovir or zidovudine-based first-line regimens.9 But until now, the significantly higher costs of these alternatives have largely prevented this switch in many developing countries. Better, less-toxic first-line regimens are still at best nearly double the price of the stavudine-based first-line regimen. However, there has been a noteworthy downward trend in the prices of less-toxic first-line combinations. The price of tenofovir has come down significantly over the past few years, by almost 77%. This means that TDF-based combinations are now nearly the same price as those containing zidovudine (see graph 2). Fixed-dose combinations containing zidovudine (AZT/3TC/NVP) and those containing tenofovir (TDF/3TC/EFV) have both fallen, by 17% and 59% respectively in the past three years. **Graph 2: The Price of Newer, Improved First-line Regimens in 2010.** Generic competition has allowed newer, improved first-line regimens recommended by WHO to fall in price, but in some countries, patent protections means prices stay at unaffordable levels. It is thanks to generic competition that these prices are steadily coming down, and they can be expected to fall further as demand increases. In countries where the drugs are not under patent or where patents owners permit such competition, the one-pill-once-a-day generic triple combination containing tenofovir/lamivudine/efavirenz (TDF/3TC/EFV) is now available for $176 ppy (see graph 2). But in some lower middle-income countries, patent owners do not permit access to generic products, meaning that countries have to rely on the ‘discounted’ price offered by originator companies. For tenofovir/emtricitabine/efavirenz (TDF/FTC/EFV), this means a price almost six times more expensive, at $1,033 ppy. The price of treatment is clearly a critical concern. But the long-term benefits of patients being able to tolerate and stay on their first ARV combination longer can outweigh the costs. A study in Lesotho showed that using a generic tenofovir-based regimen results in better quality of life for patients as compared to a stavudine-based regimen.10 And while shifting treatment programmes to a new first-line regimen brings with it clear logistical challenges on top of cost concerns, it is critical that treatment providers begin moving away from stavudine as has been done for example in Zambia, Lesotho, Guyana, South Africa and Botswana. Design HIV drugs with developing countries needs in mind © P.K. Lee/MSF With 95% of people with HIV/AIDS living in developing countries, it is urgent that research and development take into account the particular needs of these populations. Such considerations must be systematically integrated into the early stages of the drug development process. Over the last three years, there have been significant advances in HIV medicine, which have led to a number of new drugs from older classes, as well as entirely new therapeutic classes being approved for use. The new drug classes have different mechanisms of action to target the HIV virus, providing people living with HIV/AIDS with additional treatment options. However, since ARVs are developed primarily for developed country markets, data relevant to address the specific needs of populations in developing countries, such as pregnant women or people who also need to take drugs for tuberculosis due to co-infection, is not obtained in clinical trials. A further example is the lack of knowledge about the interactions between antimalarials and antiretrovirals,12 even though 80% of people living with HIV live in regions where malaria is endemic.13 Further, there is currently no safety and efficacy data for children for the new drugs etravirine, maraviroc, or raltegravir. For other drugs there are limited data: for efavirenz (no data for children under three years), atazanavir and darunavir (no data for children under six years). This despite the fact that the U.S. Food and Drug Administration (FDA) has included incentives and obligations to encourage submission of data for paediatric use since and the European Medicines Agency (EMA) followed suit in January The need for high-tech monitoring can also affect the availability of antiretrovirals. For instance, the entry inhibitor maraviroc requires a complicated diagnostic test costing more than US$ 1,900 – a factor making its use impracticable and unaffordable in developing country contexts where even simple laboratory monitoring is rarely available. B) Secure access to second- and third–line regimens Lifelong AIDS treatment requires constant access to newer and more potent drug regimens when patients develop side effects or resistance to their medicines over time. Although resistance is an inevitable element of long-term treatment, it can be delayed by using drug combinations with fewer side effects to facilitate adherence, and can be limited by changing treatment soon after viral suppression begins to wane. New WHO guidelines on second-line further simplify and prioritise the choice of regimens. Demand for newer AIDS drugs is growing fast. In one of MSF’s longest running AIDS treatment programmes, in Khayelitsha, South Africa, 14% of patients on treatment for five years needed to switch to a second-line drug combination because of virological failure.24 And 25% of those patients who switched again developed virological failure to their second-line regimen a further two years later.188 “Seeing a patient that you have been treating since 2003, now failing on her second combination, you feel, as a nurse, you are a failure. We are feeling like our hands are tied.” -- Mpumi Mantangana, MSF nurse in Khayelitsha, South Africa MSF’s Khayelitsha data provides a window into the growing need for access to newer AIDS drug regimens across the developing world in the coming years. As some patients in developing countries have already developed resistance to their second-line regimen, it is crucial to secure further treatment options essential to long-term survival. However, the price of newer regimens remains a major barrier to access. The most affordable second-line regimen recommended by new WHO guidelines is today priced at $465 (see graph 3). This is more than three times the most affordable of the improved first-line regimens recommended by WHO. **Graph 3: The treatment timebomb: the impact of switching to second- and third-line regimens on the price of ARV treatment.** Changing a patient’s regimen because of side effects or the emergence of resistance means relying on newer, patented, and therefore more expensive drugs. The price of a possible third-line regimen may cost at least 23 times more than the most affordable first-line regimen, and close to seven times more than the most affordable second-line regimen. Patients and treatment providers are once again faced with the prospect of drugs being priced out of reach. · At the time of going to press, there is no TDF/3TC + ATV+r co-pack. The Clinton Foundation-negotiated price of the individual components of this package comes to $465. CF expects the co-pack to be available by the end of At that stage its price is expected to drop to $425. Death at the doorstep: Thembisa’s story © Global Health TV “I’m so worried now because I don’t know what is going to happen to me,” says Thembisa Mkhosana, a mother of two who lives in Khayelitsha, South Africa. Thembisa discovered she was HIV-positive in 2001 and began receiving ART through MSF’s clinic two years later. She responded well to treatment and was able to return to work and take care of her children. But after showing signs of treatment failure because of drug resistance, Thembisa was switched to a second set of ARVs. Again she developed resistance. Thembisa now needs a third set of ARVs to keep her alive but those newer drugs are unaffordable. “If there’s no such thing that can help me, I know that I’m going to die,” says Thembisa. “And then who is going to look after my children?” Thembisa is but one of many patients who now need access to newer and more potent, but unaffordable ARV regimens. “What we are seeing in Khayelitsha is what we will soon see throughout Africa if there is not a focused push for urgent change,” says Dr. Eric Goemaere, Medical Coordinator for MSF in South Africa. In December 2009, WHO released new recommendations which for the first time raises the need for treatment options after failure of second-line therapy. Many studies are ongoing, and the drugs likely to have anti-HIV activity in third-line regimens are darunavir (boosted with ritonavir), etravirine and raltegravir.9 Because of patent barriers, generic competition on these medicines is severely hampered. Unlike with the first generation of AIDS drugs, patents in key producing countries such as India prevent the production of much more affordable generic versions: many of the newer ARVs will likely be under patent in India, and several such as raltegravir, maraviroc or etravirine already are. The lack of competition among generic manufacturers means that prices cannot be expected to come down the way they did for the first generation of ARVs. There is no generic version of etravirine, for example. Its manufacturer, Tibotec, has just announced a ‘discounted’ price for Sub-Saharan Africa and least-developed countries, at $913 ppy. A potential thirdline regimen could thus be available for developing countries at the prohibitive price of $3,204 ppy (at best, as this price applies to only Africa and least-developed countries).
 line regimens, which are more expensive. -- The Treatment Timebomb -- Report of the Enquiry of the UK All Party Parliamentary Group on AIDS4. There is a growing disconnect between the AIDS treatment available to people in developed countries and to their counterparts in developing countries. In wealthy countries, AIDS now resembles a chronic disease, much like heart disease or diabetes, and patients generally have access to an increasing variety of treatment options once they inevitably develop drug resistance. 5. In contrast, people living with HIV/AIDS in developing countries largely have access to only one combination of medicines that causes significant side effects, with few or no alternatives for when their treatment fails. And the youngest people living with AIDS continue to be an afterthought – paediatric treatment still lags behind that for adults, as does the development of appropriate ARVs for children. If people living with HIV/AIDS are to be given the same prospects for survival whether they live in developing countries or in wealthy countries, urgent action must be undertaken to ensure access: · to a less toxic first-line regimen; · to second- and third-line treatment options as patients develop resistance; · better and timely detection of treatment failure through increased access to viral load testing, and. · to paediatric AIDS treatment options, which must be prioritised together with the prevention of mother-to-child transmission of the virus. A) Move to a less-toxic and more robust first-line regimen. The first line of defence to help slow the pace at which patients need to switch to newer, more expensive ARV treatment regimens is a robust first-line drug combination with few side effects. Today, the majority of people on their first-line of ARVs in low- and middle-income countries receive the combination of lamivudine/stavudine/ nevirapine (3TC/d4T/NVP).6 Thanks to generic competition, this regimen now costs US$ 67 per patient per year (ppy) – 99% less than 10 years ago. This dramatic price drop was possible because of competition among multiple generic manufacturers in countries where these drugs were not patented, such as Brazil, Thailand and India (see graph 1). Notwithstanding the dramatic price drop over the past decade, using this standard combination comes at a high medical cost. The drug stavudine (d4T) causes serious side effects, some intolerable, such as peripheral neuropathy. It can also lead to lactic acidosis, which in rare cases can lead to death. It also causes stigmatisation because over long-term treatment, patients develop easily recognisable facial wasting. **Graph 1: Competition as a catalyst for price reductions** The fall in the price of first-line combinations of stavudine (d4T), lamivudine (3TC), and nevirapine (NVP), since Stavudine is virtually no longer used in wealthy countries (in 2006, for example, fewer than 2% of patients in Switzerland were taking the drug7). Patients in these countries are offered better-tolerated alternatives, such as tenofovir (TDF) or zidovudine (AZT). Since 2006, WHO has recommended in its HIV/AIDS treatment guidelines that treatment providers begin moving away from stavudine-based regimens because of their long-term irreversible side effects, towards tenofovir or zidovudine-containing regimens.8. This call was repeated in the latest recommendations released by WHO in December 2009 for ART for HIV in adults and adolescents, advising countries to develop a plan to move towards tenofovir or zidovudine-based first-line regimens.9. But until now, the significantly higher costs of these alternatives have largely prevented this switch in many developing countries. Better, less-toxic first-line regimens are still at best nearly double the price of the stavudine-based first-line regimen. However, there has been a noteworthy downward trend in the prices of less-toxic first-line combinations. The price of tenofovir has come down significantly over the past few years, by almost 77%. This means that TDF-based combinations are now nearly the same price as those containing zidovudine (see graph 2). Fixed-dose combinations containing zidovudine (AZT/3TC/NVP) and those containing tenofovir (TDF/3TC/EFV) have both fallen, by 17% and 59% respectively in the past three years. **Graph 2: The Price of Newer, Improved First-line Regimens in 2010.** Generic competition has allowed newer, improved first-line regimens recommended by WHO to fall in price, but in some countries, patent protections means prices stay at unaffordable levels. It is thanks to generic competition that these prices are steadily coming down, and they can be expected to fall further as demand increases. In countries where the drugs are not under patent or where patents owners permit such competition, the one-pill-once-a-day generic triple combination containing tenofovir/lamivudine/efavirenz (TDF/3TC/EFV) is now available for $176 ppy (see graph 2). But in some lower middle-income countries, patent owners do not permit access to generic products, meaning that countries have to rely on the ‘discounted’ price offered by originator companies. For tenofovir/emtricitabine/efavirenz (TDF/FTC/EFV), this means a price almost six times more expensive, at $1,033 ppy. The price of treatment is clearly a critical concern. But the long-term benefits of patients being able to tolerate and stay on their first ARV combination longer can outweigh the costs. A study in Lesotho showed that using a generic tenofovir-based regimen results in better quality of life for patients as compared to a stavudine-based regimen.10 And while shifting treatment programmes to a new first-line regimen brings with it clear logistical challenges on top of cost concerns, it is critical that treatment providers begin moving away from stavudine as has been done for example in Zambia, Lesotho, Guyana, South Africa and Botswana. Design HIV drugs with developing countries needs in mind. © P.K. Lee/MSF. With 95% of people with HIV/AIDS living in developing countries, it is urgent that research and development take into account the particular needs of these populations. Such considerations must be systematically integrated into the early stages of the drug development process. Over the last three years, there have been significant advances in HIV medicine, which have led to a number of new drugs from older classes, as well as entirely new therapeutic classes being approved for use. The new drug classes have different mechanisms of action to target the HIV virus, providing people living with HIV/AIDS with additional treatment options. However, since ARVs are developed primarily for developed country markets, data relevant to address the specific needs of populations in developing countries, such as pregnant women or people who also need to take drugs for tuberculosis due to co-infection, is not obtained in clinical trials. A further example is the lack of knowledge about the interactions between antimalarials and antiretrovirals,12 even though 80% of people living with HIV live in regions where malaria is endemic.13. Further, there is currently no safety and efficacy data for children for the new drugs etravirine, maraviroc, or raltegravir. For other drugs there are limited data: for efavirenz (no data for children under three years), atazanavir and darunavir (no data for children under six years). This despite the fact that the U.S. Food and Drug Administration (FDA) has included incentives and obligations to encourage submission of data for paediatric use since and the European Medicines Agency (EMA) followed suit in January The need for high-tech monitoring can also affect the availability of antiretrovirals. For instance, the entry inhibitor maraviroc requires a complicated diagnostic test costing more than US$ 1,900 – a factor making its use impracticable and unaffordable in developing country contexts where even simple laboratory monitoring is rarely available. B) Secure access to second- and third–line regimens. Lifelong AIDS treatment requires constant access to newer and more potent drug regimens when patients develop side effects or resistance to their medicines over time. Although resistance is an inevitable element of long-term treatment, it can be delayed by using drug combinations with fewer side effects to facilitate adherence, and can be limited by changing treatment soon after viral suppression begins to wane. New WHO guidelines on second-line further simplify and prioritise the choice of regimens. Demand for newer AIDS drugs is growing fast. In one of MSF’s longest running AIDS treatment programmes, in Khayelitsha, South Africa, 14% of patients on treatment for five years needed to switch to a second-line drug combination because of virological failure.24 And 25% of those patients who switched again developed virological failure to their second-line regimen a further two years later.188. Seeing a patient that you have been treating since 2003, now failing on her second combination, you feel, as a nurse, you are a failure. We are feeling like our hands are tied. -- Mpumi Mantangana, MSF nurse in Khayelitsha, South Africa. MSF’s Khayelitsha data provides a window into the growing need for access to newer AIDS drug regimens across the developing world in the coming years. As some patients in developing countries have already developed resistance to their second-line regimen, it is crucial to secure further treatment options essential to long-term survival. However, the price of newer regimens remains a major barrier to access. The most affordable second-line regimen recommended by new WHO guidelines is today priced at $465 (see graph 3). This is more than three times the most affordable of the improved first-line regimens recommended by WHO. **Graph 3: The treatment timebomb: the impact of switching to second- and third-line regimens on the price of ARV treatment.** Changing a patient’s regimen because of side effects or the emergence of resistance means relying on newer, patented, and therefore more expensive drugs. The price of a possible third-line regimen may cost at least 23 times more than the most affordable first-line regimen, and close to seven times more than the most affordable second-line regimen. Patients and treatment providers are once again faced with the prospect of drugs being priced out of reach. · At the time of going to press, there is no TDF/3TC + ATV+r co-pack. The Clinton Foundation-negotiated price of the individual components of this package comes to $465. CF expects the co-pack to be available by the end of At that stage its price is expected to drop to $425. Death at the doorstep: Thembisa’s story. © Global Health TV. I’m so worried now because I don’t know what is going to happen to me, says Thembisa Mkhosana, a mother of two who lives in Khayelitsha, South Africa. Thembisa discovered she was HIV-positive in 2001 and began receiving ART through MSF’s clinic two years later. She responded well to treatment and was able to return to work and take care of her children. But after showing signs of treatment failure because of drug resistance, Thembisa was switched to a second set of ARVs. Again she developed resistance. Thembisa now needs a third set of ARVs to keep her alive but those newer drugs are unaffordable. If there’s no such thing that can help me, I know that I’m going to die, says Thembisa. And then who is going to look after my children Thembisa is but one of many patients who now need access to newer and more potent, but unaffordable ARV regimens. What we are seeing in Khayelitsha is what we will soon see throughout Africa if there is not a focused push for urgent change, says Dr. Eric Goemaere, Medical Coordinator for MSF in South Africa. In December 2009, WHO released new recommendations which for the first time raises the need for treatment options after failure of second-line therapy. Many studies are ongoing, and the drugs likely to have anti-HIV activity in third-line regimens are darunavir (boosted with ritonavir), etravirine and raltegravir.9. Because of patent barriers, generic competition on these medicines is severely hampered. Unlike with the first generation of AIDS drugs, patents in key producing countries such as India prevent the production of much more affordable generic versions: many of the newer ARVs will likely be under patent in India, and several such as raltegravir, maraviroc or etravirine already are. The lack of competition among generic manufacturers means that prices cannot be expected to come down the way they did for the first generation of ARVs. There is no generic version of etravirine, for example. Its manufacturer, Tibotec, has just announced a ‘discounted’ price for Sub-Saharan Africa and least-developed countries, at $913 ppy. A potential thirdline regimen could thus be available for developing countries at the prohibitive price of $3,204 ppy (at best, as this price applies to only Africa and least-developed countries).")
50
Cohorte Cambodge Entre 2005 et 2007 , 837 patients Charge virale régulière et genotype si > 1000 c/mL 71 pts considréres en échec NNRTI mutations : 79% M184V : 69% TAMs : 20% K65R: 12.7% Deuxième génotype avant passage au deuxième ligne 54.4% des patients nouvelles mutations Zolfo M et al AIDS Sept 2010

51
Demand for newer AIDS drugs is growing fast
Demand for newer AIDS drugs is growing fast. In one of MSF’s longest running AIDS treatment programmes, in Khayelitsha, South Africa, 14% of patients on treatment for five years needed to switch to a second-line drug combination because of virological failure.24 And 25% of those patients who switched again developed virological failure to their second-line regimen a further two years later.188 Van Cutsem, G. Treatment failure, access to viral load, and challenges to implementing an improved first-line regimen: MSF experience in Khayelitsha and beyond. T he Emergency is not over: Access to Treatment and Challenges of Long Term Survival on Antiretroviral, Cape Town, Cape Town International Convention Centre.International AIDS Conference July

Présentations similaires










>")







 A.Compagnucci-A.Faye.>")





