Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Traumatismes crâniens de l’enfant particularités et prise en charge
Pr. Gilles Orliaguet DAR. Hôpital Necker – Enfants Malades, Paris

2
Les traumatismes de l’enfant
14 % de la traumatologie 1ère cause de mortalité des > 1 an 1/3 mortalité infantile 80 % de trauma fermés 80 % sont associés à un TC 50 % des décès sont dus au TC

3
Délai entre accident et décès traumatique chez l’enfant
Heures Patients (n)
")
4
255 enfants décédés après TC (1979-86) Causes évitables chez 32 % !
Détresse respiratoire circulatoire neurologique Inhalation Arrêt respiratoire Lésions hémorragiques "Talked and died " Hématome intra-crânien n 35 13 21 24 Rupture rate: 7 Lacérations hépatique: 3 Rupture artère iliaque: 1 Rupture organe creux: 2

5
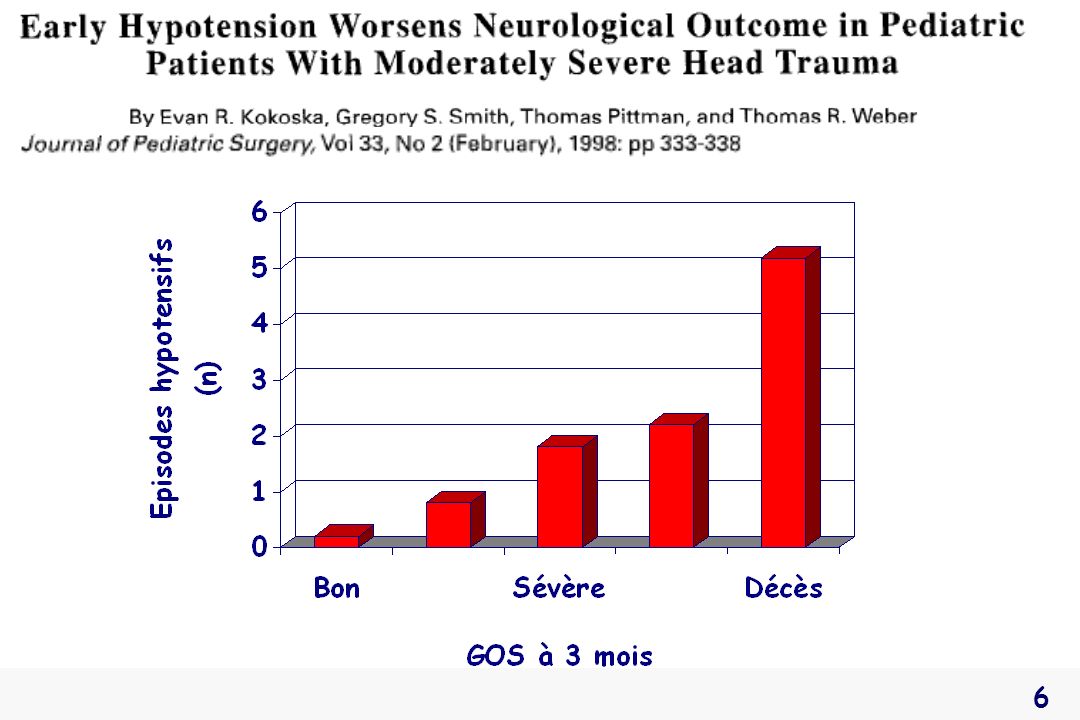
ACSOS : hypotension, hypoxie, hypercapnie, anémie
Mortalité globale = 27 % Un seul épisode hypotensif x 3,8 la mortalité

7
Principes de prise en charge en urgence
Évaluer - réanimer les détresses vitales - évaluer Respiratoire Circulatoire Neurologique Prévention des ACSOS

8
Détresse respiratoire
Éviter: apnée, hypoventilation, SpO2 <90%, PaO2 <60 mmHg Pediatr Crit Care Med 2003, 4: S9-S11 LVA Ponction IT + VA SG Obstacle Hémo-Pneumothorax suffocant Lésions pariétales, contusion pulmonaire Coma, Choc Chez l’enfant : dilatation gastrique +++ 19

10
Intubation préhospitalière en urgence : Comparaison adultes-enfants
Boswell WC. Air Med J 1995

11
Intubation et ventilation
Indications larges Au minimum si GCS < 8 Sédation Précautions pour le rachis cervical

12
Échelle de coma de Glasgow adaptée aux enfants
Simpson. Lancet 1982; II: 450 Score Ouverture des yeux Meilleure réponse verbale Réponse motrice > 2 ans < 2 ans 6 - A la demande 5 Orientée Mots/ babillements Flexion adaptée 4 Spontanée Confuse Cri irritable Flexion inadaptée 3 Au bruit Inappropriée Cri inapproprié Décortication 2 Incompréhensible Gémissement/ Geignement rare Décérébration 1 Absente

13
TC grave et lésion du rachis cervical
Adultes 1272 blessés => TC + lésion cervicale : 1,8 % O' Malley et coll. J Trauma 1988 228 blessés => TC + lésion cervicale : 1,7 % Bayless et al. Am J Emerg Med 1988 Enfants 268 patients => TC + lésion cervicale : 3,7% Laham et coll. Ped Neurosurg 1994 Précautions au ramassage et à l’intubation

14
Y penser en cas d’arrêt cardiaque
rapidement récupéré par des manœuvres de réanimation de base Trabold F, Orliaguet G. AFAR 2002

15
Lésion bulbo-médullaire
13 patients : 9 ACR récupérés (<10 min), 4 arrêts respiratoires Lésion bulbo-médullaire GCS < 8 sans LBM ISS Atteinte tronc (%) Mortalité (%) GOS > 3 à 6 mois (%) 42 * 100 * 69 * 7,7 * 29 1,9 26 56
, 4 arrêts respiratoires. Lésion bulbo-médullaire. GCS < 8 sans. LBM. ISS. Atteinte tronc (%) Mortalité (%) GOS > 3 à 6 mois (%) 42 * 100 * 69 * 7,7 * 29. 1,")
16
Incidents IET : 25 % 188 enfants atteints de TC grave :
Age médian : 7.5 ans GCS médian : 6 ISS médian : 28 Polytraumatisés : 50% Taux de succès de l’intubation trachéale : 98% Incidents IET : 25 % Prehospital tracheal intubation is difficult in the prehospital setting, but good results may be obtain provided that field physicians are trained enough. In this study performed in our institution, and which have included severely head injured children, the success rate for prehospital tracheal intubation by field physicians was ninety eight percent. 16

17
Amélioration : Protocole d’ISR Sédation Amélioration : Capnographie
SpO2 However, They were complications associated with tracheal intubation. Some may be improved using an adequate monitoring, including capnography and pulse oxymetry Why the incidence of coughing, spasms, or aspiration may be decreased with a rapid sequence induction protocol followed by continuous sedation, with a level of sedation adapted to the haemodynamic status. 17

18
Intubation des enfants traumatisés : Induction en séquence rapide
Sauf ACR, instabilité HD ou intubation difficile Etomidate : 0,2-0,4 mg/kg si > 2 ans Kétamine : 3-4 mg/kg si < 2 ans Célocurine (2 mg/kg si < 18 mois sinon 1 mg/kg) + atropine Intubation + stabilisation en ligne du rachis cervical Sédation d’entretien : midazolam + fentanyl Conférence d’Experts SFAR 1999 3
 + atropine. Intubation + stabilisation en ligne du rachis cervical. Sédation d’entretien : midazolam + fentanyl. Conférence d’Experts SFAR")
19
Impact des recommandations sur l’ISR
Etude prospective 88 enfants ; GCS 6 (3-8) Complications/incidents Recommandations : Connues Correctement citées Comparaison étude < 1996 < 1996 Recommandations connues - 67 % Recommandations conformes 2,3 % 64 %* Incidents lors de l’intubation 25 % 8 %* Martinon C. Mémoire DES 2004
 Complications/incidents. Recommandations : Connues Correctement citées. Comparaison étude < < Recommandations connues % Recommandations conformes. 2,3 % 64 %* Incidents lors de l’intubation. 25 % 8 %* Martinon C. Mémoire DES")
20
Signes cliniques d’hémorragie en fonction de la perte sanguine chez l’enfant
Pertes sanguines Signes cliniques < 20 % 25 % 40 % Cardio-vasculaires pouls filant tachycardie hypotension tachy/bradycardie Cutanés peau froide TRC 2-3 s extrémités froides cyanose pâle froid Rénaux oligurie modérée oligurie nette anurie Neuropsychiques Irritable agressif confusion léthargie coma Rasmussen G et coll. Int Anesthesiol Clin 1994 ; 32 :

21
Réponses à l’hémorragie chez l’enfant
Pression artérielle 140 100 60 20 25 50 75 Spoliation sanguine (%) Variation (%) Résistance vasculaire 40 % Débit cardiaque
 Variation (%) Résistance vasculaire. 40 % Débit cardiaque.")
22
Pronostic du collapsus en cas de traumatisme fermé chez l'enfant
2120 enfants polytraumatisés Mortalité globale : 5,2 % 38 enfants (1,8 %) avec hypoPA sévère ou ACR Mortalité : 100 % Hazinski et coll. Ann Emerg Med 1994, 23: 1229.
 avec hypoPA sévère ou ACR. Mortalité : 100 % Hazinski et coll. Ann Emerg Med 1994, 23:")
23
Détresse circulatoire chez l’enfant
Causes de détresse circulatoire Choc hémorragique hémorragie extériorisée hémorragie interne hémorragie intra-abdominale hémorragie intra-thoracique hématome intra-crânien Choc obstructif pneumothorax, tamponnade Choc cardiogénique contusion myocardique Choc distributif anaphylaxie, choc spinal, sepsis

24
Détresse circulatoire
Traiter si signes de choc ou PAS < 70+2 x(âge en ans) mmHg Pediatr Crit Care Med 2003, 4: S9-S11 Contrôle des hémorragies extériorisées : scalp +++ Au moins 1 VVP de bon calibre : 22 G Remplissage vasculaire : 20 mL/kg x 2 SB Soluté glucosé/hypotonique : contre-indiqué Adjuvants : catécholamines, transfusion Monitorage : cathéter artériel +++
 mmHg Pediatr Crit Care Med 2003, 4: S9-S11. Contrôle des hémorragies extériorisées : scalp +++ Au moins 1 VVP de bon calibre : 22 G. Remplissage vasculaire : 20 mL/kg x 2 SB. Soluté glucosé/hypotonique : contre-indiqué. Adjuvants : catécholamines, transfusion. Monitorage : cathéter artériel +++")
25
172 enfants Âge moyen : 7.0 ± 3.9 There is a paucity of data on the definition of hypotension in children, and the fact that blood pressure physiologically increases with age contribute to the lack of a consistent definition of hypotension after severe pediatric head injury. This slide shows you the Risk of Death Associated with a systolic blood pressure less than ninety millimeter of mercury after Severe traumatic brain injury in Children. The main findings of this retrospective study is that, a systolic blood pressure less than ninety millimeter of mercury was associated with poor outcome; the odds for good outcome increased once systolic blood pressure was ninety millimeter of mercury. This result indicate that management should aimed at maintaining systolic blood pressure over at least ninety millimeter of mercury. Adjusted OR: OR ajusté pour hypothermie, lésion intentionnelle, âge et sexe 25

26
Pediatric emergency intravenous access Evaluation of a protocol
Protocole d’abord veineux gradué dans l’ACR Abord veineux périphérique Abord veineux fémoral Dénudation de saphène Voie intra-osseuse Patients les plus instables Obtention d’un abord en 4,5 min vs 10 min si non respecté 66% d’accès veineux pendant les 5 premières minutes Kanter et coll. Am J Dis Child 1986

27
Colloïdes ou cristalloïdes ? En pratique
Débuter par les colloïdes en cas de collapsus Sinon débuter par les cristalloïdes

28
Variations respiratoires de la PA invasive
Choisir un indice (DPP) Valider des seuils Swedlow DB & Raphaely RC 1986
 Valider des seuils. Swedlow DB & Raphaely RC")
30
1

31
Autorégulation vasculaire cérébrale
Autorégulation normale chez l’enfant DSC Perte d'autorégulation Autorégulation normale chez l’adulte PPC (mmHg) 50 150 Pression de perfusion cérébrale (PPC) = PAM – PIC
 Pression de perfusion cérébrale (PPC) = PAM – PIC.")
32
Compliance cérébrale PIC (mmHg) TC Enfant Adulte Compensation VIC (ml)
 TC Enfant Adulte Compensation VIC (ml)")
33
Détresse neurologique
Apprécier les troubles de conscience Score de Glasgow pédiatrique État pupillaire et signes déficitaires Doppler transcrânien précoce Particularités du polytraumatisé Évaluation après stabilisation cardiorespiratoire Analyse du GCS en fonction de la sédation Maintien de la PPC

34
Doppler transcrânien Transcranial Doppler sonography is a non-invasive technique which allows real- time continuous measurements of blood flow velocity in major intracranial vessels within the circle of Willis, especially in the middle cerebral artery. Waveform analysis techniques are widely used, especially in pediatrics. This slide shows a normal TCD recording here. With increasing ICP, the diastolic flow velocity decreases and the systolic peak becomes more and more spiky. When ICP is about the same as diastolic arterial blood pressure, diastolic flow velocity is zero with only high systolic peaks. With a further decrease in CPP, a reversed diastolic flow velocity reappears. 34

35
DTC précoce et pronostic du TC chez l’enfant

36
1.31 25 cm/s

37
Pression de Perfusion Cérébrale = PPC
PPC = PAM – PIC Globalement PPC > 40 mmHg : Nourrisson PPC > 40 mmHg Enfants PPC > 60 mmHg Préhospitalier: PAS > 70 +[2x(âge en ans)] mmHg Pediatr Crit Care Med 2003, 4: S9-S11
] mmHg. Pediatr Crit Care Med 2003, 4: S9-S11.")
38
This other retrospective study confirm that the threshold values, respectively of forty and twenty, for treating a decreased cerebral perfusion pressure or an increased intracranial pressure, appear quiet adapted to the pediatric population with an increased risk of death when cerebral perfusion pressure decreased under forty millimeters of mercury or when intracranial pressure increased over twenty millimeters of mercury 38

39
Normal values of intracranial pressure and arterial blood pressure rise progressively from birth to adulthood. It is important to recognize that these age differences exist. In this study, the authors hypothesize that there may age related differences in the relationship between outcome and intracranial pressure (ICP) and cerebral perfusion pressure (CPP) in the first 6 h of monitoring in a large cohort of head injured children. For the purpose of the study, patients were divided into three age groups (2–6, 7–10 and 11–16 years). Differences were found in the specificity of ICP and CPP for each group and these were more marked for CPP. In summary, there are age related differences in the specificity of intracranial pressure and cerebral perfusion pressure in relation to outcome. These differences may be important in the clinical management of head-injured children. Thus cerebral perfusion pressures of fifty three, sixty three and sixty six mmHg should be the minimum to strive for in these three age groups respectively. 39
 and cerebral perfusion pressure (CPP) in the first 6 h of monitoring in a large cohort of head injured children. For the purpose of the study, patients were divided into three age groups (2–6, 7–10 and 11–16 years). Differences were found in the specificity of ICP and CPP for each group and these were more marked for CPP. In summary, there are age related differences in the specificity of intracranial pressure and cerebral perfusion pressure in relation to outcome. These differences may be important in the clinical management of head-injured children. Thus cerebral perfusion pressures of fifty three, sixty three and sixty six mmHg should be the minimum to strive for in these three age groups respectively. 39.")
40
Monitorage de la PIC Lyons. Mayo Clin. Proc. 1990 Intra-
parenchymateux ventriculaire Lyons. Mayo Clin. Proc. 1990 In pediatric patients requiring ICP monitoring, a ventricular catheter connected to an external strain gauge is the most accurate, low cost, and reliable method of monitoring ICP Parenchymal ICP monitoring with fiberoptic or strain gauge catheter tip transduction is similar to ventricular ICP monitoring, but has potential for measurement drift. However, this method is now largely used Subarachnoid, subdural, epidural devices and externally placed anterior fontanel monitors are less accurate and should not be used

41
PPC = PAM – PIC PA PVC PIC PPC
One major interest of continuous monitoring of ICP is to enable the continuous monitoring of cerebral perfusion pressure, defined as the mean arterial blood pressure minus ICP, provided that MAP is invasively monitored using an arterial catheter PPC

42
Maintien de la PPC 1- Mesures générales : 3- Traiter HIC > 20 mmHg
Idem adulte Tête en rectitude Éviter compression jugulaire Lit surélevé à +30° Analgésie-sédation 3- Traiter HIC > 20 mmHg Hyperventilation Osmothérapie Éviter hyperthermie Barbituriques Craniectomies Hypothermie 2- Maintenir la PAM Normovolémie (C) Vasopresseur si besoin Pediatr Crit Care Med 2003, 4: S9-S11
 Vasopresseur si besoin. Pediatr Crit Care Med 2003, 4: S9-S11.")
43
Effet de l’hyperventilation sur le DSC de l’enfant TCG avec GCS < 8
Skippen et coll. Crit Care Med 1997; 25: 20 40 60 80 100 Fréquence ischémie > 1 région du cerveau (%) 35 25-35 < 25 PaCO2 (mmHg)
 < 25. PaCO2 (mmHg)")
44
Ventilation de l’enfant TC grave : Recommandations (grade C)
HyperV prophylactique (PaCO2 < 35 mmHg) : à éviter PaCO mmHg si HIC réfractaire PaCO2 < 30 mmHg si HIC réfractaire persistante => Détecter ischémie cérébrale (DSC, SvJO2, PtiO2 …) Pediatr Crit Care Med 2003, 4: S9-S11
 : à éviter. PaCO mmHg si HIC réfractaire. PaCO2 < 30 mmHg si HIC réfractaire persistante. => Détecter ischémie cérébrale (DSC, SvJO2, PtiO2 …) Pediatr Crit Care Med 2003, 4: S9-S11.")
45
Use of hypertonic saline in the treatment of severe refractory posttraumatic intracranial hypertension in pediatric traumatic brain injury 10 enfants en HTIC réfractaire =>NaCl 3% : QSP PIC <20 mmHg Khanna S et al. Critical Care Medicine 2000; 28,

46
Khanna S. Crit Care Med. 2000

47
Osmothérapie et HIC post-TC chez l’enfant
Mannitol : efficace pour traiter HIC post-TC - Bolus : 0,25 à 1 g/kg - Osmo P < 320 mOsm/L SSH : efficace pour traiter HIC post-TC SSH 3% : 0,1 à 1 ml/kg/h Dose minimale pour PIC < 20 mmHg Osmolalité plasmatique < 360 mOsm/L Pediatr Crit Care Med 2003, 4: S9-S11

48
Barbituriques à fortes doses (grade C)
A considérer si : Hypertension intracrânienne réfractaire Patients hémodynamiquement stables TC sévère mais " sauvable" Risque majoré d’hypotension artérielle Nécessite un support hémodynamique approprié The recent american guidelines state that high dose barbiturates, may be considered in case of: Refractory intracranial hypertension In hemodynamically stable patients With salvageable severe head injury However, as we all know, there is an Increased risk of systemic hypotension Therefore the use of high dose barbiturates require an appropriate hemodynamic monitoring and cardiovascular support Pediatr Crit Care Med 2003, 4: S9-S11 48

49
Craniectomie décompressive chez l’enfant
Contrôle Étude prospective, randomisée : enfants TC avec HIC Craniectomie à 19,2 h (7,3-29,3 h) 54% de bon pronostic à 6 mois vs 14% PIC (mmHg) Décompression PIC (mmHg) Taylor A. Child ’s Nerv Syst 2001
 54% de bon pronostic à 6 mois vs 14% PIC (mmHg) Décompression. PIC (mmHg) Taylor A. Child ’s Nerv Syst")
50
Craniectomies décompressives : Recommandations (C)
Si gonflement cérébral diffus Avec HTIC réfractaire au traitement médical Détérioration secondaire du GCS et/ou engagement cérébral Pendant les 48 première h après le TC GCS > 3 Aucun épisode de PIC maintenue > 40 mmHg Pediatr Crit Care Med 2003, 4: S9-S11

51
Recently, at least two studies have focused on the effects of decompressive craniectomy on outcome in severely head injured children.

52
Hypothermie modérée Nombre limité d’études chez l’enfant
Hypothermie modérée chez l’adulte = NS Clifton et al. New Engl J Med 2001 Nombre limité d’études chez l’enfant Étude clinique de Phase II de sécurité Adelson P et al. Neurosurgery 2005 Étude d’efficacité HypHIT : 1ers résultats négatifs ! Hutchinson J et al. Dev Neuroscience 2006 The induction of hypothermia to treat patients was originally reported more than fifty years ago, but use of therapeutic hypothermia did not become established because studies lacked sufficient level of evidence. In adult patients, a study by Marion has reported that moderate hypothermia reduced ICP and showed a trend toward improved outcome. However, a more recent study by the same group of investigators reported a lack of effectiveness in adults TBI patients. In children, the data are limited for the moment. The results of the multicenter HypHIT study of the efficacy of hypothermia are not yet published and there is only one Phase II clinical trial that concluded to the safety of the technique. 52

53
Protocoles de prise en charge

54
TC grave de l’enfant et stratégie de transport
En zone urbaine : les enfants TC graves devraient être transportés directement dans un Trauma Center Pédiatrique ou à défaut dans un centre adulte avec du personnel qualifié pour la pédiatrie (grade B) Pediatr Crit Care Med 2003, 4: S5-S8
 Pediatr Crit Care Med 2003, 4: S5-S8.")
55
Enfant TC grave en préhospitalier
Prise en charge sur les lieux par une équipe médicalisée Stabilisation des détresses vitales Rechercher des lésions associées Maintenir l'axe tête-cou-tronc Perfusion: NaCl 0,9% Intubation en séquence rapide > 1 abord veineux périphérique rachis cervical Maintenir la normovolémie PAS > 90 mmHg Ventilation mécanique : 35<PaCO2<38 mmHg Sonde oro-gastrique Entretien de la sédation : benzodiazépine ± morphinique Surveiller: FC, PAS, GCS, EtCO2, SpO2, EtCO2 Centre de Traumatologie Pédiatrique Régulation par le SAMU

56
Enfant TC grave à l’admission
Arrivée au Centre de Traumatologie Pédiatrique Évaluation des fonctions vitales Monitorage invasif de la pression artérielle Stabilisation des détresses vitales Bilan du polytraumatisme potentiel Bilan radiologique minimal : RxP (F) rachis cervical (P), bassin (F), Échographie abdominale, Doppler TC Respiratoire Circulatoire Neurologique Patient stabilisé sous surveillance continue Scanner cérébral Scanner rachis,thorax et abdomen Indications chirurgicales rares Éviter la chirurgie non vitale Monitorage: PAM, PIC, PPC, PVC, diurèse, analgésie-sédation Neuroréanimation
 rachis cervical (P), bassin (F), Échographie abdominale, Doppler TC. Respiratoire. Circulatoire. Neurologique. Patient stabilisé sous surveillance continue. Scanner cérébral. Scanner rachis,thorax et abdomen. Indications chirurgicales rares. Éviter la chirurgie non vitale. Monitorage: PAM, PIC, PPC, PVC, diurèse, analgésie-sédation. Neuroréanimation.")
57
Traumatisme crânien avec score de Glasgow < 8
TDM : œdème ou lésion sans indication chirurgicale Monitorage PIC = Capteur parenchymateux ou DVE Objectif de PPC : mmHg MESURES GENERALES Tête de lit +30°, éviter compression jugulaire Normoxie et normocapnie (35-38mmHg) Analgésie-Sédation Maintien PAM, PIC et PPC Lutte contre l’hyperthermie Hypertension intracrânienne ? PIC > 20 mmHg > 10 min PIC < 20 mmHg Traitements de 1ère ligne : Drainage contrôlé du LCR Mannitol 20% ou SSH 3% Hyperventilation modérée (PaCO mmHg) PIC contrôlée Surveillance continue de la PIC h PIC non contrôlée TDM cérébrale : lésion chirurgicale ? Traitements de seconde ligne
 Analgésie-Sédation Maintien PAM, PIC et PPC Lutte contre l’hyperthermie. Hypertension intracrânienne PIC > 20 mmHg > 10 min. PIC < 20 mmHg. Traitements de 1ère ligne : Drainage contrôlé du LCR Mannitol 20% ou SSH 3% Hyperventilation modérée (PaCO mmHg) PIC contrôlée. Surveillance continue de la PIC h. PIC non contrôlée. TDM cérébrale : lésion chirurgicale Traitements de seconde ligne.")
58
TDM cérébrale : lésion chirurgicale ? Craniectomie décompressive si :
Traitements de seconde ligne : Hyperventilation profonde (PaCO2 < 30 mmHg) « Coma barbiturique » Hypothermie modérée (32-34°C) PIC contrôlée Surveillance de la PIC h TDM cérébrale : lésion chirurgicale ? PIC non contrôlée Craniectomie décompressive si : œdème cérébral diffus, dans les 48 premières heures, sans longues phases de PPC<40 mmHg, sans complications secondaires sans épisode d’engagement PIC contrôlée
 « Coma barbiturique » Hypothermie modérée (32-34°C) PIC contrôlée. Surveillance. de la PIC h. TDM cérébrale : lésion chirurgicale PIC non contrôlée. Craniectomie décompressive si : œdème cérébral diffus, dans les 48 premières heures, sans longues phases de PPC<40 mmHg, sans complications secondaires. sans épisode d’engagement. PIC contrôlée.")
59
Conclusion Petit nombre de patients Possibilité de récupération +++
Limiter décès et séquelles lourdes Trauma Center pédiatrique Équipe multidisciplinaire Prise en charge précoce en rééducation 28 33

60
Trauma Center pédiatrique Rééducation spécialisée Alerte précoce Réanimation préhospitalière

61
Fin

62
SCIWORA chez l’enfant SCIWORA Spinal Cord Injury Whitout Radiographic
Abnormality Revue systématique 15 articles 695 enfants Pang D. Neurosurgery 55: , 2004

Présentations similaires