Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Prévention et diagnostic des infections sur cathéter
Geneve, 8 mars 2007 Prévention et diagnostic des infections sur cathéter Jean-François TIMSIT Réanimation médicale CHU Grenoble Epidémiologie des cancers et des affections graves UJF/Inserm U823

2
Modes de colonisations
Extraluminale Endoluminale

3
Cathéters ou chambres implantables
Onco-hématologie / utilisation séquentielle : CCI>>>KT 0.1 vs 2.77/ 1000 j-cathéter (Groegger 1993) Fréquence d’utilisation des CCI (Astagneau 1999) Cancer 0.17/1000j si 20-40% vs 4.9/1000j si 60-80% journées d’utilisation Utilisation continue, NPT: VIH >>> cancerologie Dénutrition du VIH:CCI vs CVC (NS) (Astagneau 1999) cancer
 Fréquence d’utilisation des CCI (Astagneau 1999) Cancer 0.17/1000j si 20-40% vs 4.9/1000j si 60-80% journées d’utilisation. Utilisation continue, NPT: VIH >>> cancerologie. Dénutrition du VIH:CCI vs CVC (NS) (Astagneau 1999) cancer.")
4
Insertion- Matériel Asepsie chirurgicale à la pose (Ia)
Préférer la voie sous clavière à la voie femorale (Ia) et à la voie jugulaire (Ib) Tunnélisation si la voie fémorale ou jugulaire est utilisée (Ia) Pas de changements systématiques (Ia) Mono=multilumières (Ia) MMWR Aug 2002; 51: 1-31 Consensus SRLF: Réactualisation 2003
 et à la voie jugulaire (Ib) Tunnélisation si la voie fémorale ou jugulaire est utilisée (Ia) Pas de changements systématiques (Ia) Mono=multilumières (Ia) MMWR Aug 2002; 51: Consensus SRLF: Réactualisation")
5
CHX-Ag impregnated catheters for long –term BR-BSI?
Meta-analysis: Silver-sulfadiazine-chlorhexidine 11 studies CVCs (2-10 days) 0.03 0.1 0.3 1.0 RR (95% CI) colonization: ( ) 25.3% vs. 43.5% bacteremia: 0.56 ( ) % vs. 5.2% Veenstra JAMA 1999 BUT: Half-life of impregnation:7 days <7 days: median 6 days 4.1 to 1.9% (OR: % CI: ) >7 days: median 12 days 4.5% to 4.2% (OR: %CI; ) Walder B - Infect Control Hosp Epidemiol 2002; 23:
 RR (95% CI) colonization: 0.44 ( ) 25.3% vs. 43.5% bacteremia: 0.56 ( ) 3.2% vs. 5.2% Veenstra JAMA BUT: Half-life of impregnation:7 days. <7 days: median 6 days 4.1 to 1.9% (OR: % CI: ) >7 days: median 12 days 4.5% to 4.2% (OR: %CI; ) Walder B - Infect Control Hosp Epidemiol 2002; 23:")
6
Catheter-related sepsis and colonization
400 NCC ACC 193 207 CVC inserted 175 188 CVC analyzed 34 (19.4%) 19 (10.1%) Positive CVC cultures 23 (13.2%) 7 (3.7%) Colonization 11 (5) 6.3% 4 (3) 2.1% CRSepsis (CRBacteremia) Brun-Buisson et al – Intensive Care Med May;30(5):837-43
 19 (10.1%) Positive CVC cultures. 23 (13.2%) 7 (3.7%) Colonization. 11 (5) 6.3% 4 (3) 2.1% CRSepsis (CRBacteremia) Brun-Buisson et al – Intensive Care Med May;30(5):")
7
2nd chlorhexidine-sulfadiazine Catheters
9 Hospitals, July 98- June 2001 ICU, Triple lumen Double blind Funding source: Arrow Charact. Control n=393 Arrow-gard n=384 APACHE II 17 MV 305 (78) 288 (75) TPN 124 (32) 131 (34) GWX 4.8 6.5 subclavian 136 (35) 141 (37) Duration (h) 142 (2-709) 123 ( ) Inf suspected 83 (14) 60 (16) Maki or Sheretz + 59 (16.3) 32 (9.3) * CNS 42 * S aureus 10 * CVC-BSI definite 3 (0.8) 1 (0.3) CVC-BSI def and possible 8 (2.2) 6 (1.7) Background: Central venous catheter–related infections are a significant medical problem. Improved preventive measures are needed. Objective: To ascertain 1) effectiveness of a second-generation antiseptic-coated catheter in the prevention of microbial colonization and infection; 2) safety and tolerability of this device; 3) microbiology of infected catheters; and 4) propensity for the development of antiseptic resistance. Design: Multicenter, randomized, double-blind, controlled trial. Setting: 9 university-affiliated medical centers. Patients: 780 patients in intensive care units who required central venous catheterization. Intervention: Patients received either a standard catheter or a catheter coated with chlorhexidine and silver sulfadiazine. Measurements: The authors assessed catheter colonization and catheter-related infection, characterized microbes by molecular typing, and determined their susceptibility to antiseptics. Patient tolerance of the catheter was monitored. Results: Patients with the 2 types of catheters had similar demographic features, clinical interventions, laboratory values, and risk factors for infection. Antiseptic catheters were less likely to be colonized at the time of removal compared with control catheters (13.3 vs colonized catheters per 1000 catheter-days; P < 0.01). The center-stratified Cox regression hazard ratio for colonization controlling for sampling design and potentially confounding variables was 0.45 (95% CI, 0.25 to 0.78). The rate of definitive catheter-related bloodstream infection was 1.24 per 1000 catheter-days (CI, 0.26 to 3.62 per 1000 catheter-days) for the control group versus 0.42 per 1000 catheter-days (CI, 0.01 to 2.34 per 1000 catheter-days) for the antiseptic catheter group (P 0.6). Coagulase-negative staphylococci and other gram-positive organisms were the most frequent microbes to colonize catheters. Noninfectious adverse events were similar in both groups. Antiseptic susceptibility was similar for microbes recovered from either group. Limitations: The antiseptic catheter was not compared with an antibiotic-coated catheter, and no conclusion can be made regarding its effect on bloodstream infection. Conclusions: The second-generation chlorhexidine–silver sulfadiazine catheter is well tolerated. Antiseptic coating appears to reduce microbial colonization of the catheter compared with an uncoated catheter. Ann Intern Med. 2005;143: Rupp ME et al – Ann Intern Med 2005; 143:570 (*) p<0.01
 288 (75) TPN. 124 (32) 131 (34) GWX subclavian. 136 (35) 141 (37) Duration (h) 142 (2-709) 123 ( ) Inf suspected. 83 (14) 60 (16) Maki or Sheretz + 59 (16.3) 32 (9.3) * CNS * S aureus * CVC-BSI definite. 3 (0.8) 1 (0.3) CVC-BSI def and possible. 8 (2.2) 6 (1.7) Background: Central venous catheter–related infections are a. significant medical problem. Improved preventive measures are. needed. Objective: To ascertain 1) effectiveness of a second-generation. antiseptic-coated catheter in the prevention of microbial colonization. and infection; 2) safety and tolerability of this device; 3) microbiology of infected catheters; and 4) propensity for the development. of antiseptic resistance. Design: Multicenter, randomized, double-blind, controlled trial. Setting: 9 university-affiliated medical centers. Patients: 780 patients in intensive care units who required central. venous catheterization. Intervention: Patients received either a standard catheter or a. catheter coated with chlorhexidine and silver sulfadiazine. Measurements: The authors assessed catheter colonization and. catheter-related infection, characterized microbes by molecular. typing, and determined their susceptibility to antiseptics. Patient. tolerance of the catheter was monitored. Results: Patients with the 2 types of catheters had similar demographic. features, clinical interventions, laboratory values, and risk. factors for infection. Antiseptic catheters were less likely to be. colonized at the time of removal compared with control catheters. (13.3 vs colonized catheters per 1000 catheter-days; P < 0.01). The center-stratified Cox regression hazard ratio for colonization. controlling for sampling design and potentially confounding. variables was 0.45 (95% CI, 0.25 to 0.78). The rate of definitive. catheter-related bloodstream infection was 1.24 per catheter-days (CI, 0.26 to 3.62 per 1000 catheter-days) for the. control group versus 0.42 per 1000 catheter-days (CI, 0.01 to per 1000 catheter-days) for the antiseptic catheter group (P. 0.6). Coagulase-negative staphylococci and other gram-positive. organisms were the most frequent microbes to colonize catheters. Noninfectious adverse events were similar in both groups. Antiseptic. susceptibility was similar for microbes recovered from either. group. Limitations: The antiseptic catheter was not compared with an. antibiotic-coated catheter, and no conclusion can be made regarding. its effect on bloodstream infection. Conclusions: The second-generation chlorhexidine–silver sulfadiazine. catheter is well tolerated. Antiseptic coating appears to. reduce microbial colonization of the catheter compared with an. uncoated catheter. Ann Intern Med. 2005;143: Rupp ME et al – Ann Intern Med 2005; 143:570. (*) p<0.01.")
8
Objective: We sought to compare the impact of antimicrobial
Darrouiche RO et al - Ann Surg 2005;242: 193–200) Objective: We sought to compare the impact of antimicrobial impregnation to that of tunneling of long-term central venous catheters on the rates of catheter colonization and catheter-related bloodstream infection. Summary Background Data: Tunneling of catheters constitutes a standard of care for preventing infections associated with long-term vascular access. Although antimicrobial coating of short-term central venous catheters has been demonstrated to protect against catheter-related bloodstream infection, the applicability of this preventive approach to long-term vascular access has not been established. Methods: A prospective, randomized clinical trial in 7 universityaffiliated hospitals of adult patients who required a vascular access for 2 weeks. Patients were randomized to receive a silicone central venous catheter that was either impregnated with minocycline and rifampin or tunneled. The occurrence of catheter colonization and catheter-related bloodstream infection was determined. Results: Of a total of 351 inserted catheters, 346 (186 antimicrobialimpregnated and 160 tunneled) were analyzed for catheter-related bloodstream infection. Clinical characteristics were comparable in the 2 study groups, but the antimicrobial-impregnated catheters remained in place for a shorter period of time (mean, 30.2 versus 43.8 days). Antimicrobial-impregnated catheters were as likely to be colonized as tunneled catheters (7.9 versus 6.3 per 1000 catheterdays). Bloodstream infection was 4 times less likely to originate from antimicrobial-impregnated than from tunneled catheters (0.36 versus 1.43 per 1000 catheter-days). Conclusions: Antimicrobial impregnation of long-term central venous catheters may help obviate the need for tunneling of catheters. linear fit of the data (r ) indicated that the mean zone of inhibition was 10 mm through 60 days. The concentrations of minocycline and rifampin on the surface of catheters decreased with increasing duration of catheter placement and both agents were detectable through 60 days of dwell time. « both agents were detectable through 60 days of dwell time »
 Objective: We sought to compare the impact of antimicrobial. impregnation to that of tunneling of long-term central venous. catheters on the rates of catheter colonization and catheter-related. bloodstream infection. Summary Background Data: Tunneling of catheters constitutes a. standard of care for preventing infections associated with long-term. vascular access. Although antimicrobial coating of short-term central. venous catheters has been demonstrated to protect against. catheter-related bloodstream infection, the applicability of this preventive. approach to long-term vascular access has not been established. Methods: A prospective, randomized clinical trial in 7 universityaffiliated. hospitals of adult patients who required a vascular access. for 2 weeks. Patients were randomized to receive a silicone central. venous catheter that was either impregnated with minocycline and. rifampin or tunneled. The occurrence of catheter colonization and. catheter-related bloodstream infection was determined. Results: Of a total of 351 inserted catheters, 346 (186 antimicrobialimpregnated. and 160 tunneled) were analyzed for catheter-related. bloodstream infection. Clinical characteristics were comparable in. the 2 study groups, but the antimicrobial-impregnated catheters. remained in place for a shorter period of time (mean, 30.2 versus days). Antimicrobial-impregnated catheters were as likely to be. colonized as tunneled catheters (7.9 versus 6.3 per 1000 catheterdays). Bloodstream infection was 4 times less likely to originate. from antimicrobial-impregnated than from tunneled catheters (0.36. versus 1.43 per 1000 catheter-days). Conclusions: Antimicrobial impregnation of long-term central venous. catheters may help obviate the need for tunneling of catheters. linear fit of the data (r2 0.77) indicated that the mean zone. of inhibition was 10 mm through 60 days. The concentrations. of minocycline and rifampin on the surface of catheters. decreased with increasing duration of catheter placement and. both agents were detectable through 60 days of dwell time. « both agents were detectable through 60 days of dwell time »")
9
10.4) for antimicrobial-impregnated catheters and 6.3 (95%
Darrouiche RO et al - Ann Surg 2005;242: 193–200) The rates of catheter colonization per 1000 catheter-days were 7.9 (95% CI 5.5– 10.4) for antimicrobial-impregnated catheters and 6.3 (95% CI 4.4–8.2) for tunneled catheters (P 0.46). A statistically insignificant trend was noted for higher likelihood of fungal colonization of antimicrobial-impregnated versus tunneled catheters (relative risk, 2.94; 95% CI 0.82–10; P 0.09), whereas gram-negative bacteria (relative risk, 2.56; 95% CI 0.80–8.13; P 0.15) and polymicrobes (relative risk, 2.27; 95% CI 0.80–6.50; P 0.19) tended to colonize tunneled catheters more than antimicrobial-impregnated catheters. Ten cases (6.3%) of bloodstream infection were related to tunneled catheters, as compared with 2 cases (1.1%) associated with antimicrobialimpregnated catheters (relative risk, 5.81; 95% CI 1.29 –26.1; P ). The rates of catheterrelated bloodstream infection per 1000 catheter-days were 0.36 (95% CI 0–0.85) for antimicrobial-impregnated catheters and 1.43 (95% CI 0.54 –2.32) for tunneled catheters (P 0.13). Although there was a trend toward a lower risk of nosocomial bacteremia in patients who received antimicrobial- impregnated versus tunneled catheters (26% versus 37%), the difference was not significant (P 0.26). There were no significant differences between the 2 groups in the proportions receiving therapy with vancomycin (47% versus 56%) or antibiotics in general (95% versus 96%). CVC col vs 6.3/1000 cvc-days, p=0.46 Fungi col 3 vs 10, RR=2.94, p=0.09 CR-BSI: 10 vs 2 RR=5.8, p=0.015 Rate: vs 1.43/1000 cvc-days, p=0.13 Nos. bact: 26% vs 37 %, p=0.26 Vanco use: 47% vs 56% NS AB use: 95% vs 96% NS
 The rates of catheter colonization per 1000 catheter-days were 7.9 (95% CI 5.5– 10.4) for antimicrobial-impregnated catheters and 6.3 (95% CI 4.4–8.2) for tunneled catheters (P 0.46). A statistically insignificant trend was noted for higher. likelihood of fungal colonization of antimicrobial-impregnated. versus tunneled catheters (relative risk, 2.94; 95% CI. 0.82–10; P 0.09), whereas gram-negative bacteria (relative. risk, 2.56; 95% CI 0.80–8.13; P 0.15) and polymicrobes. (relative risk, 2.27; 95% CI 0.80–6.50; P 0.19) tended to. colonize tunneled catheters more than antimicrobial-impregnated. catheters. Ten cases (6.3%) of bloodstream infection were related to tunneled catheters, as. compared with 2 cases (1.1%) associated with antimicrobialimpregnated. catheters (relative risk, 5.81; 95% CI 1.29 –26.1; P 0.015). The rates of catheterrelated. bloodstream infection per 1000 catheter-days were (95% CI 0–0.85) for antimicrobial-impregnated catheters. and 1.43 (95% CI 0.54 –2.32) for tunneled catheters (P. 0.13). Although there was a trend toward a lower risk of nosocomial bacteremia in patients who received antimicrobial- impregnated versus tunneled catheters (26% versus 37%), the difference was not significant (P 0.26). There were no significant differences between the 2 groups in the proportions receiving therapy with vancomycin (47% versus 56%) or antibiotics in general (95% versus 96%). CVC col. 7.9 vs 6.3/1000 cvc-days, p=0.46. Fungi col 3 vs 10, RR=2.94, p=0.09. CR-BSI: 10 vs 2 RR=5.8, p= Rate: 0.36 vs 1.43/1000 cvc-days, p=0.13. Nos. bact: 26% vs 37 %, p=0.26. Vanco use: 47% vs 56% NS. AB use: 95% vs 96% NS.")
10
Pansements MMWR Aug 2002; 51: 1-31 Asepsie, Gants stériles (Ic)
Pas de solvant organique (éther, acétone) (Ia) Chlorhexidine, teinture d’iode, povidone iodée, alcool 70° (Ia) Pansements stériles transparent semi-perméable ou gazes (Ia) Si saignement (J1) ou sueurs : gaze (II) Changement immédiat du pansement si souillé ou décollé (Ib) Pas de pommade antibiotique ou antiseptique (Ia) Pansement au moins toutes les semaines (transparents) ou toutes les 48 heures (gaze) (II) Pansement daté (IV) MMWR Aug 2002; 51: 1-31
 (Ia) Chlorhexidine, teinture d’iode, povidone iodée, alcool 70° (Ia) Pansements stériles transparent semi-perméable ou gazes (Ia) Si saignement (J1) ou sueurs : gaze (II) Changement immédiat du pansement si souillé ou décollé (Ib) Pas de pommade antibiotique ou antiseptique (Ia) Pansement au moins toutes les semaines (transparents) ou toutes les 48 heures (gaze) (II) Pansement daté (IV) MMWR Aug 2002; 51:")
11
Catheter dressing change frequency and
cutaneous toxicity during high dose chemotherapy E. Benhamou et al Bone marrow transplant 2002; 29: 653 E. Benhamou et al (in press)
")
12
Catheter dressing change frequency and
risk of infection during high dose chemotherapy 15 Day change n = 56 4 Day change S. epidermidis on the initial sample 5 (9 %) 4 (7 %) subsequent cutaneous colonisation 15 (27%) 13 (23%) Bacteremia 6 (11%) 7 (13%) CRS 1 (S. epidermidis) 1 (Klebsiella & E. coli) E. Benhamou et al Bone marrow transplant 2002; 29: 653
 4 (7 %) subsequent cutaneous colonisation. 15 (27%) 13 (23%) Bacteremia. 6 (11%) 7 (13%) CRS. 1 (S. epidermidis) 1 (Klebsiella & E. coli) E. Benhamou et al Bone marrow transplant 2002; 29: 653.")
13
Quel antiseptique? Infections bactériémiques liées aux cathéters
Chaiyakunapruk N - Ann Intern Med 2002; 136:792 Favors PVI Favors CHG Infections bactériémiques liées aux cathéters

14
Betadine (PVI) vs Betadine alcool (A-PVI)
Betadine (PVI) vs Betadine alcool (A-PVI) Parienti et al – CCM : 306 22 GWX 21 <3dys APVI N=149 PVI N=157 19 GWX 21 <3dys 106 CVCs 117 CVCs Colonisation 35% Infection 13.7% Bacteriémies 1% P<0.001 P<0.04 NS Colonisation 13.2% Infection 4.7% Bacteriémies 3% Randomisation des 2 unités par périodes de 3 mois en cross over Beaucoup de desequilibres étonnant entre les populations… Déséquilibre APV I: plus jeune (p<0.001), moins d’OSF>2 (p<0.001) La différence n’existe que pour les Gram + (SCN et autres) Après ajustement: HR colonisation: 0.3 ( ), p<0.001
 vs Betadine alcool (A-PVI) Parienti et al – CCM : GWX. 21 <3dys. APVI. N=149. PVI. N= GWX. 21 <3dys. 106 CVCs. 117 CVCs. Colonisation 35% Infection 13.7% Bacteriémies 1% P< P<0.04. NS. Colonisation 13.2% Infection 4.7% Bacteriémies 3% Randomisation des 2 unités par périodes de 3 mois en cross over. Beaucoup de desequilibres étonnant entre les populations… Déséquilibre APV I: plus jeune (p<0.001), moins d’OSF>2 (p<0.001) La différence n’existe que pour les Gram + (SCN et autres) Après ajustement: HR colonisation: 0.3 ( ), p<")
15
Eponges imprégnées de chlorhexidine (BiopatchTM)
Pansement tous les 2 jours transparents vs tous les 7 jours avec une éponge.Randomisé Apache II 22 idem dans les 2 groupes Controle n=736 KT 216 (29%) 24 (3.3%) Biopatch n=665 KT 109 (16%) 8 (1.2%) Maki+ Maki + 1 HC periph HR: 0.62 ( ) HR: 0.38 ( ) Maki et al, 40th ICAAC 2000; 1430, p422
 24 (3.3%) Biopatch. n=665 KT. 109 (16%) 8 (1.2%) Maki+ Maki + 1 HC periph. HR: 0.62 ( ) HR: 0.38 ( ) Maki et al, 40th ICAAC 2000; 1430, p422.")
16
Lignes et tubulures Changements toutes les 72 heures au moins (Ia)
Changement des tubulures contenant des lipides (NPT, Propofol(Ia)) dans les 24 heures (Ib) Un acces dédié à la NPT si multi-lumières (II) Changement des tubulures de transfusions dans les 24 heures (Ib) Manipulation des rampes: compresses stériles, antiseptiques (Ia), bouchons sur les voies des rampes non utilisées (Ib) MMWR Aug 2002; 51: 1-31 Consensus SRLF: Réactualisation 2003
) dans les 24 heures (Ib) Un acces dédié à la NPT si multi-lumières (II) Changement des tubulures de transfusions dans les 24 heures (Ib) Manipulation des rampes: compresses stériles, antiseptiques (Ia), bouchons sur les voies des rampes non utilisées (Ib) MMWR Aug 2002; 51: Consensus SRLF: Réactualisation")
17
Protections des rampes
Rampes fixées en dehors du lit Bouchons à l’extrémité de toutes les voies non utilisées Raccords désinfectés avant mise en place de toutes les perfusions Pas d’avantages à l’utilisation de boites de protections imprégnés d’antiseptiques Lucet JC et al – ICHE 2000; 21:40

18
Injections-perfusions
Durée de perfusion: Lipides(12h), mélanges ternaires (24h), sang (4h) (Ib) Nutrition: mélanges ternaires ou préparation sous flux laminaire (Ib) Vérifier la transparence et l’absence de dépots (Ib) Mono-dose Pas de filtres antibactériens (Ia) MMWR Aug 2002; 51: 1-31 Consensus SRLF: Réactualisation 2003
, mélanges ternaires (24h), sang (4h) (Ib) Nutrition: mélanges ternaires ou préparation sous flux laminaire (Ib) Vérifier la transparence et l’absence de dépots (Ib) Mono-dose. Pas de filtres antibactériens (Ia) MMWR Aug 2002; 51: Consensus SRLF: Réactualisation")
19
Relationship between thrombosis and infection
Post-mortem study: long term catheter Thrombus of the vein wall in 38% of catheterized veins 7/31 patients with thombosis have had a CR-BSI 0/41 patients with a normal catheterized vein have developped CR-BSI Raad - JAMA 1994; 271:1014

20
Héparine et KT veineux centraux
Meta-analyse: 13 études randomisées (KT imprégnés 4, héparine 8, HBPM 1) RR Héparine et thrombose: 0.43 [ ] Héparine et colonisation de KT: 0.18 [ ] Héparine et bactériémies: 0.26 [ ] Randolph AG - Chest 1998;113:165-71
 RR. Héparine et thrombose: 0.43 [ ] Héparine et colonisation de KT: 0.18 [ ] Héparine et bactériémies: 0.26 [ ] Randolph AG - Chest 1998;113:")
21
Continuous infusion of low dose Unfractionated heparin in Patients with onco-hematologic diseases
Abdelkefi et al – J Clin Oncol 2005; 23:7864 UH: 100 U/Kg/dys vs Saline Subclavian, investigator blinded 210 eligible/ 204 included Thrombosis: 2 vs10, p=0.017 CR-BSI: 7 vs 17, p=0.03 (4.2 vs 2.5/1000 dys) Heparin (102) Control (102) P value Duration of cvc 27 (8-81) 26 (8-74) .1 Reason for removal End of treatment CRThrombosis CRBI 84 2 7 65 10 17 .03 Stem cell transplant 82 81 .2 TPN Abx Blood Asparaginase 62 85 5 54 72 70 6 .6 CRT No CRT CR-BSI 2 22 No 10 170 Purpose Infection is a serious complication of central venous catheters in immunocompromised patients. Catheter-related infection may be caused by fibrin deposition associated with catheters. Interventions designed to decrease fibrin deposition have the potential to reduce catheter-related infections. The purpose of this study was to evaluate the role of low-dose unfractionated heparin in preventing catheter-related bloodstream infection in patients with hemato-oncological disease. Patients and Methods This study was a randomized, controlled trial in which patients with nontunneled catheters were randomly assigned to receive either intravenous unfractionated heparin (continuous infusion of 100 U/kg per day) or 50 mL/day of normal saline solution as a continuous infusion (control group). Heparin was continued until the day of discharge. Catheter-related bloodstream infection was defined according to Infectious Disease Society of America guidelines. Results Two hundred and eight patients were randomly assigned. Four patients were excluded after assignment. Ultimately, 204 patients were analyzed. Catheter-related bloodstream infection occurred in 6.8% (7 of 102 catheters) of those in the heparin group (2.5 events per 1,000 days) and in 16.6% (17 of 102 catheters) of those in the control group (6.4 events per 1,000 days) (P .03). No other risk factors were found for the development of catheter-related bloodstream infection. Four and five patients experienced severe bleeding in the heparin and control groups, respectively (P .2). We did not observe heparin-induced thrombocytopenia. Conclusion The use of continuous infusion of low-dose unfractionated heparin (100 U/kg per day) can be a practical and economical approach to the prevention of catheter-related bloodstream infection in patients with hemato-oncological disease. J Clin Oncol 23: © 2005 by American Society of Clinical Oncology P=0.6
 Heparin (102) Control (102) P value. Duration of cvc. 27 (8-81) 26 (8-74) .1. Reason for removal. End of treatment. CRThrombosis. CRBI Stem cell transplant TPN. Abx. Blood. Asparaginase CRT. No CRT. CR-BSI No Purpose. Infection is a serious complication of central venous catheters in immunocompromised. patients. Catheter-related infection may be caused by fibrin deposition associated with. catheters. Interventions designed to decrease fibrin deposition have the potential to reduce. catheter-related infections. The purpose of this study was to evaluate the role of low-dose. unfractionated heparin in preventing catheter-related bloodstream infection in patients with. hemato-oncological disease. Patients and Methods. This study was a randomized, controlled trial in which patients with nontunneled catheters. were randomly assigned to receive either intravenous unfractionated heparin (continuous. infusion of 100 U/kg per day) or 50 mL/day of normal saline solution as a continuous infusion. (control group). Heparin was continued until the day of discharge. Catheter-related bloodstream. infection was defined according to Infectious Disease Society of America guidelines. Results. Two hundred and eight patients were randomly assigned. Four patients were excluded after. assignment. Ultimately, 204 patients were analyzed. Catheter-related bloodstream infection. occurred in 6.8% (7 of 102 catheters) of those in the heparin group (2.5 events per 1,000. days) and in 16.6% (17 of 102 catheters) of those in the control group (6.4 events per 1,000. days) (P .03). No other risk factors were found for the development of catheter-related. bloodstream infection. Four and five patients experienced severe bleeding in the heparin and. control groups, respectively (P .2). We did not observe heparin-induced thrombocytopenia. Conclusion. The use of continuous infusion of low-dose unfractionated heparin (100 U/kg per day) can be. a practical and economical approach to the prevention of catheter-related bloodstream. infection in patients with hemato-oncological disease. J Clin Oncol 23: © 2005 by American Society of Clinical Oncology. P=0.6.")
22
Urokinase lock Dillon et al - J Clin Oncol. 2004;22(13):2718-23
577 patients, 29 centers 281 ports, 288 external CVCs (86% bi-lumen) Bimodal distribution of age 2y and 15y Hemato 63%, solid tumors 35% CVCs:131 111 days, ports:170 121 days BSI: 16 ports (6%) vs 43 CVCs (16%) Rate of occlusive events: 21 vs 31% p=0.006, logrank test Rate of infections 1.6 vs 2.2 CR-BSI, p=0.07, logrank test Occlusive events 23% v 31%, P .006 Ports The rate of infection for all devices combined was 1.4-fold less in the urokinase group (1.6 events per 1,000 days) than in the heparin group (2.2 events per 1,000 days; P .05), with a log-rank value of P .07 for time to first event (Fig 4). When stratified according to device, only external catheters had evidence of a treatment effect with urokinase (2.6 events per 1,000 days) when compared with heparin (3.9 events per 1,000 days; P .04). The log-rank value was P.10 Department of Surgery, Division of Pediatric Surgery, Penn State College of Medicine, Hershey, PA 17033, USA. PURPOSE: Infection and thrombosis are serious complications of long-term vascular access devices in children undergoing chemotherapy. Since routine fibrinolytic therapy may decrease these complications, the purpose of this study was to compare the efficacy of an every-2-week administration of urokinase with standard heparin flushes in reducing the incidence of device-related infections and occlusions. MATERIALS AND METHODS: This study was a prospective, randomized phase III multicenter trial conducted by the Children's Cancer Group, in which patients with implantable ports or tunneled catheters received either urokinase or heparin every 2 weeks for 12 months. Study end points were time to first occlusion or time to first device-related infection. RESULTS: Five hundred seventy-seven patients from 29 institutions were enrolled, of whom 51% had external catheters and 49% had ports. Urokinase administration resulted in fewer occlusive events than heparin (23% v 31%; P =.02), a longer time to first occlusive event (log-rank analysis, P =.006), and a 1.6-fold difference in the rate of occlusive events (Poisson regression, P =.003). Similar results were noted when comparing ports and tunneled catheters. The urokinase group also had a 1.4-fold difference in the rate of infection (Poisson regression, P =.05) and longer time to first infection (log-rank, P =.07), but the difference was significant only in tunneled catheters. CONCLUSION: Urokinase administration every 2 weeks significantly affects the rate of occlusive events in ports and tunneled catheters and of infectious events in external catheters compared with heparin administration. 2.6 vs 3.9 / 1000 CVCs days External cath.
 Bimodal distribution of age 2y and 15y. Hemato 63%, solid tumors 35% CVCs:131 111 days, ports:170 121 days. BSI: 16 ports (6%) vs 43 CVCs (16%) Rate of occlusive events: 21 vs 31% p=0.006, logrank test. Rate of infections. 1.6 vs 2.2 CR-BSI, p=0.07, logrank test. Occlusive events. 23% v 31%, P Ports. The rate of infection for all devices combined was. 1.4-fold less in the urokinase group (1.6 events per 1,000. days) than in the heparin group (2.2 events per 1,000 days; P .05), with a log-rank value of P .07 for time to first. event (Fig 4). When stratified according to device, only. external catheters had evidence of a treatment effect with. urokinase (2.6 events per 1,000 days) when compared with. heparin (3.9 events per 1,000 days; P .04). The log-rank. value was P.10. Department of Surgery, Division of Pediatric Surgery, Penn State College of Medicine, Hershey, PA 17033, USA. PURPOSE: Infection and thrombosis are serious complications of long-term vascular access devices in children undergoing chemotherapy. Since routine fibrinolytic therapy may decrease these complications, the purpose of this study was to compare the efficacy of an every-2-week administration of urokinase with standard heparin flushes in reducing the incidence of device-related infections and occlusions. MATERIALS AND METHODS: This study was a prospective, randomized phase III multicenter trial conducted by the Children s Cancer Group, in which patients with implantable ports or tunneled catheters received either urokinase or heparin every 2 weeks for 12 months. Study end points were time to first occlusion or time to first device-related infection. RESULTS: Five hundred seventy-seven patients from 29 institutions were enrolled, of whom 51% had external catheters and 49% had ports. Urokinase administration resulted in fewer occlusive events than heparin (23% v 31%; P =.02), a longer time to first occlusive event (log-rank analysis, P =.006), and a 1.6-fold difference in the rate of occlusive events (Poisson regression, P =.003). Similar results were noted when comparing ports and tunneled catheters. The urokinase group also had a 1.4-fold difference in the rate of infection (Poisson regression, P =.05) and longer time to first infection (log-rank, P =.07), but the difference was significant only in tunneled catheters. CONCLUSION: Urokinase administration every 2 weeks significantly affects the rate of occlusive events in ports and tunneled catheters and of infectious events in external catheters compared with heparin administration. 2.6 vs 3.9 / 1000 CVCs days. External cath.")
23
Thrombolysis Urokinase > 5000 IU every 1-2 or 3-4 weeks
Reduced incidence of thrombosis Reduced the incidence of premature IVD loss Tendency of benefit to reduce CR-BSI Cost-benefit analysis? Three recent randomized trials of prophylactic installation of urokinase (5000 IU/mL every 1–2 or 3–4 weeks) into long-termIVDs have shown a reduced incidence of thrombosis and premature IVD loss [57–59]. Of more importance, 2 of these trials also showed a reduction in IVDR BSIs (table 2) [57, 58]. Prophylactic thrombolysis appears to be well tolerated, but a costbenefit analysis of this novel but expensive practice needs to be performed. Adapted From Ray CE 1999, Dillon 2004, Solomon 200, Aquino 2002
 into long-termIVDs. have shown a reduced incidence of thrombosis and premature. IVD loss [57–59]. Of more importance, 2 of these trials also. showed a reduction in IVDR BSIs (table 2) [57, 58]. Prophylactic. thrombolysis appears to be well tolerated, but a costbenefit. analysis of this novel but expensive practice needs to. be performed. Adapted From Ray CE 1999, Dillon 2004, Solomon 200, Aquino")
24
Antibiotic lock therapy
117 Long-term CVCs Hematologic patients with neutropenia 10 UI/ml of heparin + 25µg/ml de Vanco 1 heure/2 days Potential ecological impact The aim of the present study was to determine the efficacy of an antibiotic-lock technique in preventing endoluminal catheter-related infection with gram-positive bacteria in neutropenic patients with hematologic malignancies. Patients with nontunneled, multilumen central venous catheters were assigned in a randomized, double-blinded manner to receive either 10 U of heparin per ml (57 patients) or 10 U of heparin per ml and 25 microg of vancomycin per ml (60 patients), which were instilled in the catheter lumen and which were allowed to dwell in the catheter lumen for 1 h every 2 days. Insertion-site and hub swabs were taken twice weekly. The primary and secondary end points of the trial were significant colonization of the catheter hub and catheter-related bacteremia, respectively. Significant colonization of the catheter hub occurred in nine (15.8%) patients receiving heparin (seven patients were colonized with Staphylococcus epidermidis, one patient was colonized with Staphylococcus capitis, and one patient was colonized with Corynebacterium sp.), whereas the catheter hubs of none of the patients receiving heparin and vancomycin were colonized (P = 0.001). Catheter-related bacteremia developed in four (7%) patients receiving heparin (three patients had S. epidermidis bacteremia and one patient had S. capitis bacteremia), whereas none of the patients in the heparin and vancomycin group had catheter-related bacteremia (P = 0.05). The times to catheter hub colonization and to catheter-related bacteremia by the Kaplan-Meier method were longer in patients receiving heparin and vancomycin than in patients receiving heparin alone (P = and P = 0.06, respectively). Our study shows that a solution containing heparin and vancomycin administered by using an antibiotic-lock technique effectively prevents catheter hub colonization with gram-positive bacteria and subsequent bacteremia during chemotherapy-induced neutropenia in patients with hematologic malignancy. Carratala AAC 1999; 43:2200
 or 10 U of heparin per ml and 25 microg of vancomycin per ml (60 patients), which were instilled in the catheter lumen and which were allowed to dwell in the catheter lumen for 1 h every 2 days. Insertion-site and hub swabs were taken twice weekly. The primary and secondary end points of the trial were significant colonization of the catheter hub and catheter-related bacteremia, respectively. Significant colonization of the catheter hub occurred in nine (15.8%) patients receiving heparin (seven patients were colonized with Staphylococcus epidermidis, one patient was colonized with Staphylococcus capitis, and one patient was colonized with Corynebacterium sp.), whereas the catheter hubs of none of the patients receiving heparin and vancomycin were colonized (P = 0.001). Catheter-related bacteremia developed in four (7%) patients receiving heparin (three patients had S. epidermidis bacteremia and one patient had S. capitis bacteremia), whereas none of the patients in the heparin and vancomycin group had catheter-related bacteremia (P = 0.05). The times to catheter hub colonization and to catheter-related bacteremia by the Kaplan-Meier method were longer in patients receiving heparin and vancomycin than in patients receiving heparin alone (P = and P = 0.06, respectively). Our study shows that a solution containing heparin and vancomycin administered by using an antibiotic-lock technique effectively prevents catheter hub colonization with gram-positive bacteria and subsequent bacteremia during chemotherapy-induced neutropenia in patients with hematologic malignancy. Carratala AAC 1999; 43:2200.")
25
Ab lock therapy Henrickson 2000; J Clin Oncol 18:1269-1278
=Vanco+heparin =Vanco+heparin+cirpo Purpose: To determine whether an antibiotic flush solution containing vancomycin, heparin, and ciprofloxacin (VHC) can prevent the majority of line infections. Patients and Methods: A prospective double-blind study was performed comparing VHC to vancomycin and heparin (VH) to heparin alone in 126 pediatric oncology patients. Results: The 153 assessable lines resulted in 36,944 line days studied. There were 58 blood stream infections (43 Gram-positive, 14 Gram-negative, and one fungal). Forty were defined as line infections (31 heparin, three VH, six VHC). The time to develop a line infection was significantly increased using either antibiotic flush (VH, P ; VHC, P ). The rate of total line infections (VH, P ; VHC, P ), Gram-positive line infections (VH, P ; VHC, P ), and Gram-negative line infections (VH, P ; VHC, P ) was significantly reduced by either VH or VHC. Sixty-two (41%) of the lines developed 119 occlusion episodes (heparin, 3.99 per 1,000 line days; VHC, 1.75 per 1,000 line days; P ). Neither antibiotic could be detected after flushing, and no adverse events were detected, including increased incidence of vancomycin-resistant Enterococcus colonization or disease. Conclusion: The use of either VH or VHC flush solution significantly decreased the complications associated with the use of tunneled central venous lines in immunocompromised children and would save significant health care resources. J Clin Oncol 18: © 2000 by American Society of Clinical Oncology.
 can prevent the majority of line infections. Patients and Methods: A prospective double-blind study was performed comparing VHC to vancomycin and heparin (VH) to heparin alone in 126 pediatric oncology patients. Results: The 153 assessable lines resulted in 36,944 line days studied. There were 58 blood stream infections (43 Gram-positive, 14 Gram-negative, and one fungal). Forty were defined as line infections (31 heparin, three VH, six VHC). The time to develop a line infection was significantly increased using either antibiotic flush (VH, P ; VHC, P ). The rate of total line infections (VH, P ; VHC, P ), Gram-positive line infections (VH, P ; VHC, P ), and Gram-negative line infections (VH, P ; VHC, P ) was significantly reduced by either VH or VHC. Sixty-two (41%) of the lines developed 119 occlusion episodes (heparin, 3.99 per 1,000 line days; VHC, 1.75 per 1,000 line days; P ). Neither antibiotic could be detected after flushing, and no adverse events were detected, including increased incidence of vancomycin-resistant Enterococcus colonization or disease. Conclusion: The use of either VH or VHC flush solution significantly decreased the complications associated with the use of tunneled central venous lines in immunocompromised children and would save significant health care resources. J Clin Oncol 18: © 2000 by American. Society of Clinical Oncology.")
26
Avoir du bon sens…

27
Durée du cathétérisme REACAT

28
Les CVCs ne sont pas toujours justifiés surtout en dehors des réanimations..
Enquête transversale, Hôpital entier CVC justifié si: pas de voies périphériques, surv. hémodynamique, NPT, vasopresseurs, 2 tt IV simultanés, ou justification verbale 320 patients, 74 CVCs, 62 (19%) Pts (46 ICU, 28 non ICU) p=0.007 Ils ont regardé depuis quand le cvc n’etait plus justifie et jusqu’à quand il a été laissé 1: Infect Control Hosp Epidemiol Mar;25(3): Unnecessary use of central venous catheters: the need to look outside the intensive care unit. Trick WE, Vernon MO, Welbel SF, Wisniewski MF, Jernigan JA, Weinstein RA. Division of Healthcare Quality Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USA. We developed criteria for justifiable CVC use and evaluated CVC use in a public hospital. Unjustified CVC-days were more common for non-ICU patients compared with ICU patients. Also, insertion-site dressings were less likely to be intact on non-ICU patients. Interventions to reduce CVC-associated bloodstream infections should include non-ICU patients. Trick et al- ICHE 2004; 25:266
 Pts (46 ICU, 28 non ICU) p= Ils ont regardé depuis quand le cvc n’etait plus justifie et jusqu’à quand il a été laissé. 1: Infect Control Hosp Epidemiol Mar;25(3): Unnecessary use of central venous catheters: the need to look outside the intensive care unit. Trick WE, Vernon MO, Welbel SF, Wisniewski MF, Jernigan JA, Weinstein RA. Division of Healthcare Quality Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USA. We developed criteria for justifiable CVC use and evaluated CVC use in a public hospital. Unjustified CVC-days were more common for non-ICU patients compared with ICU patients. Also, insertion-site dressings were less likely to be intact on non-ICU patients. Interventions to reduce CVC-associated bloodstream infections should include non-ICU patients. Trick et al- ICHE 2004; 25:266.")
29
Utilisation du cathéter
Ratio patients/infirmières Fridkin, Infect Control Hosp Epidemiol 1996 et « qualité » des infirmières Robert, Infect Control Hosp Epidemiol 2000;21:12 Impact d’un « IV-team » (Soifer, Arch Intern Med 1998) Diminution des signes et symptôme d’inflammation Diminution du nombre de sepsis sur cathéter
 Diminution des signes et symptôme d’inflammation. Diminution du nombre de sepsis sur cathéter.")
30
L’éducation Sherertz, Ann Intern Med 2000 Coopersmith, Crit Care Med 2002 Impact d’une stratégie de prévention (Eggimann, Lancet 2000) Diminution des infections sur cathéter Diminution de l’ensemble des infections nosocomiales

31
Les précautions maximales ne sont pas appliquées…
Les précautions maximales ne sont pas appliquées… Rubinson et al – JAMA 2003; 2802 Pratiques des internistes posant des CVCs aux USA Juin 2002: Questionnaires 526 réponses/1000 Gants stériles 99.4% Masques 66.3% Champs stériles larges 35% Les 3 précédentes 28.2% Préparation Antiseptique 99.8% Sous-clavière préférentielle 17% KT imprégnés 16.7% Antibioprophylaxie 2.3% Questionnaires à 1000 internistes aux usa, lettre du JAMA

32
Infect Control Hosp Epidemiol 2005;26:525-533
« … US internists rarely use these practices during CVC insertion. The key reasons for nonadherence are that most internists do not believe that the use of maximal barrier precautions is effective and they have limited access to chlorhexidine gluconate. » BACKGROUND AND OBJECTIVE: High morbidity of CVC-related infections has led to national guidelines for their prevention. Despite recommendations for the use of maximal barrier precautions (mask, sterile gloves, gown, and large drape) and skin antisepsis with 2% chlorhexidine gluconate during CVC insertion, internists in the United States are not implementing these practices frequently. This study sought to identify and characterize the obstacles to and potential opportunities for improving adherence. DESIGN: Cross-sectional survey. PAR TICIPANTS: One thousand randomly selected physician- members of the American College of Physicians–American Society of Internal Medicine. METHODS: Several potential determinants of adherence to maximal barrier precautions were assessed, including awareness of, agreement with, and ability to implement the recommendation, as well as the practice and training characteristics of the respondents. Factors influencing antiseptic selection were also recorded. RESULTS: Of 526 respondents, 178 (34%) had recently inserted CVCs. Clinician experience and subspecialty, awareness of CDC guidelines, and external influences (eg, time to collect equipment) did not affect maximal barrier precautions adherence. The only independent predictor of adherence was high outcome expectancy for the use of large sterile drapes (OR, 5.3; CI95, 2.2–12.6). Availability had the greatest influence on internists’ selection of specific antiseptic agents, whereas cost was the least important determinant. CONCLUSIONS: Despite established efficacy, use of maximal barrier precautions and chlorhexidine gluconate is low among internists. Because improved adherence to these practices will require increased outcome expectancy for maximal barrier precautions and availability of chlorhexidine gluconate, targeting these areas through focused education and systems modifications is essential (Infect Control Hosp Epidemiol 2005;26: ). Infect Control Hosp Epidemiol 2005;26:
 and skin antisepsis with 2% chlorhexidine gluconate during CVC. insertion, internists in the United States are not implementing. these practices frequently. This study sought to identify and characterize. the obstacles to and potential opportunities for improving. adherence. DESIGN: Cross-sectional survey. PAR TICIPANTS: One thousand randomly selected physician- members of the American College of Physicians–American. Society of Internal Medicine. METHODS: Several potential determinants of adherence to. maximal barrier precautions were assessed, including awareness. of, agreement with, and ability to implement the recommendation, as well as the practice and training characteristics of the respondents. Factors influencing antiseptic selection were also recorded. RESULTS: Of 526 respondents, 178 (34%) had recently. inserted CVCs. Clinician experience and subspecialty, awareness. of CDC guidelines, and external influences (eg, time to. collect equipment) did not affect maximal barrier precautions. adherence. The only independent predictor of adherence was. high outcome expectancy for the use of large sterile drapes. (OR, 5.3; CI95, 2.2–12.6). Availability had the greatest influence. on internists’ selection of specific antiseptic agents, whereas. cost was the least important determinant. CONCLUSIONS: Despite established efficacy, use of. maximal barrier precautions and chlorhexidine gluconate is. low among internists. Because improved adherence to these. practices will require increased outcome expectancy for maximal. barrier precautions and availability of chlorhexidine gluconate, targeting these areas through focused education and systems. modifications is essential (Infect Control Hosp Epidemiol. 2005;26: ). Infect Control Hosp Epidemiol 2005;26:")
33
System-based prevention
Little sterile drape + povidone iodine Large sterile drape + CHX 2%-Alcohol CVC-associated BSI rate 11.3 per 1000 CVC-days 3.7 per 1000 CVC-days (P= .01). Background: The central venous catheter (CVC) is a necessary, yet inherently risky, modern medical device. We aimed to carry out a systems-based intervention designed to facilitate the use of maximal sterile barrier precautions and the use of chlorhexidine for skin antisepsis during insertion of CVC. Methods: All patients in whom a CVC was inserted at a medical-surgical intensive care unit at a university-affiliated public hospital were included in a before-after trial. The standard CVC kit in routine use before the intervention included a small sterile drape (24’’ by 36’’) and 10% povidone-iodine for skin antisepsis. We special ordered a customized kit that, instead, included a large sterile drape (41’’ by 55’’) and 2% chlorhexidine gluconate in 70% isopropyl alcohol. Both the standard kit in use before the intervention and the customized kit included identical CVCs. Baseline data included the quarterly CVC-associated bloodstream infection (BSI) rates during the 15 months before the intervention. Comparison data included the quarterly CVC-associated BSI rates during the 15 months after we instituted exclusive use of the customized kit. Results: The mean quarterly CVC-associated BSI rate decreased from a baseline of 11.3 per 1000 CVC-days before the intervention to 3.7 per 1000 CVC-days after the intervention (P , .01). Assuming direct costs of at least $10,000 per CVC-associated BSI, we calculated resultant annualized savings to the hospital of approximately $350,000. Conclusion: Infection control interventions that rely on voluntary changes in human behavior, despite the best intentions of us all, are often unsuccessful. We have demonstrated that a systems-based intervention led to a sustained decrease in the CVC-associated BSI rate, thereby resulting in improved patient safety and decreased cost of care. (Am J Infect Control 2006;34:503-6.) Young EM - Am J Infect Control 2006;34:503-6
. Background: The central venous catheter (CVC) is a necessary, yet inherently risky, modern medical device. We aimed to carry out. a systems-based intervention designed to facilitate the use of maximal sterile barrier precautions and the use of chlorhexidine for. skin antisepsis during insertion of CVC. Methods: All patients in whom a CVC was inserted at a medical-surgical intensive care unit at a university-affiliated public hospital. were included in a before-after trial. The standard CVC kit in routine use before the intervention included a small sterile drape (24’’ by 36’’) and 10% povidone-iodine for skin antisepsis. We special ordered a customized kit that, instead, included a large sterile. drape (41’’ by 55’’) and 2% chlorhexidine gluconate in 70% isopropyl alcohol. Both the standard kit in use before the intervention. and the customized kit included identical CVCs. Baseline data included the quarterly CVC-associated bloodstream infection (BSI) rates during the 15 months before the intervention. Comparison data included the quarterly CVC-associated BSI rates during. the 15 months after we instituted exclusive use of the customized kit. Results: The mean quarterly CVC-associated BSI rate decreased from a baseline of 11.3 per 1000 CVC-days before the intervention. to 3.7 per 1000 CVC-days after the intervention (P , .01). Assuming direct costs of at least $10,000 per CVC-associated BSI, we. calculated resultant annualized savings to the hospital of approximately $350,000. Conclusion: Infection control interventions that rely on voluntary changes in human behavior, despite the best intentions of us all, are often unsuccessful. We have demonstrated that a systems-based intervention led to a sustained decrease in the CVC-associated. BSI rate, thereby resulting in improved patient safety and decreased cost of care. (Am J Infect Control 2006;34:503-6.) Young EM - Am J Infect Control 2006;34:")
34
Improve the bedside behavior
Improve the bedside behavior Coopersmith et al – Arch Surg 2004; 139:131 July 99: comprehensive educational program Nov 2000: First behavioral audit Behavioral intervention: pictures, demonstrations, monthly lectures Feb 2002: 2nd behavioral audit 10.8 The Impact of Bedside Behavior on Catheter-Related Bacteremia in the Intensive Care Unit (comportement) Craig M. Coopersmith, MD; Jeanne E. Zack, BSN; Myrna R. Ward, BSN; Carrie S. Sona, MSN; Marilyn E. Schallom, MSN; Sharon J. Everett, BSN; Way Y. Huey, PharmD; Teresa M. Garrison, MSN; Jan McDonald, BSN; Timothy G. Buchman, PhD, MD; Walter A. Boyle, MD; Victoria J. Fraser, MD; Louis B. Polish, MD Hypothesis: The success of an educational program in July 1999 that lowered the catheter-related bloodstream infection (CRBSI) rate in our intensive care unit (ICU) 3-fold is correlated with compliance with “bestpractice” behaviors. Design: Before-after trial. Setting: Surgical ICU in a referral hospital. Patients: A random sample underwent bedside audits of central venous catheter care (n=187). All ICU admissions during a 39-month period (N=4489) were prospectively followed for bacteremia. Interventions: On the basis of audit results in December 2000, a behavioral intervention was designed to improve compliance with evidenced-based guidelines of central venous catheter management. Main Outcome Measures: Compliance with practices known to decrease CRBSI. Secondary outcome was CRBSI rate on all ICU patients. Results: Multiple deficiencies were identified on bedside audits 18 months after the previous educational program. After the implementation of a separate behavioral intervention in July 2001, a second set of bedside audits in December 2001 demonstrated improvements in documenting the dressing date (11% to 21%; P_.001) and stopcock use (70% to 24%; P_.001), whereas nonsignificant trends were observed in hand hygiene (17% to 30%; P_.99) and maximal sterile barrier precautions (50% to 80%; P=.29). Appropriate practice was observed before and after the behavioral intervention in catheter site placement, dressing type, absence of antibiotic ointment, and proper securing of central venous catheters. Thirty-two CRBSIs occurred in 9353 catheter-days 24 months before the behavioral intervention compared with 17 CRBSIs in 6152 catheter-days during the 15 months after the intervention (3.4/1000 to 2.8/1000 catheter-days; P=.40). Conclusions: Although a previous educational program decreased the CRBSI rate, this was associated with only modest compliance with best practice principles when bedside audits were performed 18 months later. A behavioral intervention improved all identified deficiencies, leading to a nonsignificant decrease in CRBSIs. Arch Surg. 2004;139: 3.4 2.8
 Craig M. Coopersmith, MD; Jeanne E. Zack, BSN; Myrna R. Ward, BSN; Carrie S. Sona, MSN; Marilyn E. Schallom, MSN; Sharon J. Everett, BSN; Way Y. Huey, PharmD; Teresa M. Garrison, MSN; Jan McDonald, BSN; Timothy G. Buchman, PhD, MD; Walter A. Boyle, MD; Victoria J. Fraser, MD; Louis B. Polish, MD. Hypothesis: The success of an educational program in July 1999 that lowered the catheter-related bloodstream. infection (CRBSI) rate in our intensive care unit (ICU) 3-fold is correlated with compliance with bestpractice behaviors. Design: Before-after trial. Setting: Surgical ICU in a referral hospital. Patients: A random sample underwent bedside audits of central venous catheter care (n=187). All ICU admissions. during a 39-month period (N=4489) were prospectively followed for bacteremia. Interventions: On the basis of audit results in December 2000, a behavioral intervention was designed to improve. compliance with evidenced-based guidelines of central venous catheter management. Main Outcome Measures: Compliance with practices known to decrease CRBSI. Secondary outcome was. CRBSI rate on all ICU patients. Results: Multiple deficiencies were identified on bedside audits 18 months after the previous educational program. After the implementation of a separate behavioral intervention in July 2001, a second set of bedside audits. in December 2001 demonstrated improvements in documenting the dressing date (11% to 21%; P_.001) and stopcock. use (70% to 24%; P_.001), whereas nonsignificant trends were observed in hand hygiene (17% to 30%; P_.99) and maximal sterile barrier precautions (50% to 80%; P=.29). Appropriate practice was observed before. and after the behavioral intervention in catheter site placement, dressing type, absence of antibiotic ointment, and. proper securing of central venous catheters. Thirty-two CRBSIs occurred in 9353 catheter-days 24 months before. the behavioral intervention compared with 17 CRBSIs in 6152 catheter-days during the 15 months after the intervention. (3.4/1000 to 2.8/1000 catheter-days; P=.40). Conclusions: Although a previous educational program decreased the CRBSI rate, this was associated with. only modest compliance with best practice principles when bedside audits were performed 18 months later. A. behavioral intervention improved all identified deficiencies, leading to a nonsignificant decrease in CRBSIs. Arch Surg. 2004;139:")
35
5 intervention program Berenholtz et al – CCM 2004; 32:2014-2020
Educating the staff Creating a catheter insertion cart Asking providers daily if catheters should be removed Implementing a checklist to assure adherence to evidence based guidelines Empowering nurse to stop the catheter insertion procedure if protocol violation was observed Control ICU=institutional educational intervention alone Significant decrease in the slope p<0.001 Poisson regression In the control unit the only intervention was the institutionnal educational intervention to increase provider awareness of evidence based infection control practices for inserting and maintaining central catheters Berenholtz et al – CCM 2004; 32:

36
Participation à un réseau de surveillance
Réseau KISS (RFA) Organisation d’un feedback par centre et global (6mois) 25 ICU en 97, 212 en Juin 2001 82 unités avec participation > 24 mois 28.6%, p=0.04 Zuschneid I et al – ICHE 2003; 24:
 Organisation d’un feedback par centre et global (6mois) 25 ICU en 97, 212 en Juin unités avec participation > 24 mois. 28.6%, p=0.04. Zuschneid I et al – ICHE 2003; 24:")
37
Patient education Moller T et la - Journal Hosp
Patient education Moller T et la - Journal Hosp. Infect (2005) 61, 330–341 82 tunneled Hickman cath., hematology Individualized training vs control General information Pratical guidance in principles and techniques Controlled testing of the patients’ theoretical knowledge and behavior 3 modules: sterile dressing + flushing techniques + drawing blood samples Summary A functioning tunnelled central venous catheter (CVC) is a crucial device for patients with haematological malignancies receiving high-dose intravenous chemotherapy. Despite the advantages, CVC infections are a major cause of sepsis and prolonged hospital stay. This study investigated the impact of patient education regarding provision of their own catheter care on the frequency of CVC-related infections (CRIs) and was conducted at a specialized haematological unit at the University Hospital of Copenhagen Rigshospitalet. FromMay to September 2002, 82 patients fitted with tunnelled double-lumen Hickman catheters were randomized consecutively. The intervention group (42 participants) received individualized training and supervision by a clinical nurse specialist, with the aim of becoming independently responsible for their own catheter care. The control group (40 participants) followed the standard CVC procedures carried out by nurses inside and outside the central hospital.Asignificant reduction inCRIswas found in the intervention group, with aO50% reduction in the incidence rate of CRIs. We conclude that systematic individualized, supervised patient education is able to reduce catheter-related infections.
 61, 330– tunneled Hickman cath., hematology. Individualized training vs control. General information. Pratical guidance in principles and techniques. Controlled testing of the patients’ theoretical knowledge and behavior. 3 modules: sterile dressing + flushing techniques + drawing blood samples. Summary A functioning tunnelled central venous catheter (CVC) is a crucial. device for patients with haematological malignancies receiving high-dose. intravenous chemotherapy. Despite the advantages, CVC infections are a. major cause of sepsis and prolonged hospital stay. This study investigated the. impact of patient education regarding provision of their own catheter care on. the frequency of CVC-related infections (CRIs) and was conducted at a. specialized haematological unit at the University Hospital of Copenhagen. Rigshospitalet. FromMay to September 2002, 82 patients fitted with tunnelled. double-lumen Hickman catheters were randomized consecutively. The. intervention group (42 participants) received individualized training and. supervision by a clinical nurse specialist, with the aim of becoming. independently responsible for their own catheter care. The control group (40. participants) followed the standard CVC procedures carried out by nurses. inside and outside the central hospital.Asignificant reduction inCRIswas found. in the intervention group, with aO50% reduction in the incidence rate of CRIs. We conclude that systematic individualized, supervised patient education is. able to reduce catheter-related infections.")
38
Infections liées aux cathéters: indicateur de qualité ….
Fréquence Définition Morbidité EVITABILITE

40
Techniques « cathéters enlevés »
Technique de Maki: Technique de Sherertz Technique de Brun Buisson Mais en dehors des états de choc septique la question est surtout comment conserver le cathéter sans risque…

41
Manifestations cliniques des infections de KT
Rien Rougeur: très fréquent, valeur prédictive faible Douleur: à distance de la pose ++ Ecoulement purulent, tunnelite 70 à 80 % des KT enlevés pour suspicion d'infection sont enlevés à tort 5

42
Surveillance cultures of tunneled cuffed Catheter exit sites in chronic hemodialysis patients are of no benefit – RosenbaumD et al - Hemodialysis International 2006; 10:365–370 Routine swabs performed once a week Group A: randomized to receive topical Abx if positive swab Catheter-related infections are a major cause of morbidity and mortality in hemodialysis (HD) patients. This study evaluated the utility of surveillance swab cultures (Ssc) of tunneled cuffed catheter (TCC) exit sites as a prediction and prevention strategy for infection. A 6-month prospective-controlled trial with 94 chronic HD patients with a TCC who received monthly Ssc and were stratified by dialysis day into topical therapy based on Ssc results (Group A) or no therapy (Group B). Outcomes were exit site infection (ESI) and catheter-associated bacteremia (CAB). The overall monthly prevalence of positive Ssc was 14.9%. There was no difference in the number of positive Ssc (17.7% vs. 11.6%, p40.05) or ESI (19.6% vs.16.3%, p40.05) between Groups A and B, respectively. Catheterassociated bacteremia was higher in Group A (17.7% vs. 4.7%, p=0.05). There were significantly more ESI in the patients treated for a positive Ssc. In Group A, the incidence of ESI was significantly higher in those treated for a positive vs. negative Ssc (55% vs. 12%, p=0.009) and CAB rates trended higher with positive Ssc (22.2% vs. 16.7%, p40.05). The strategy of treating positive surveillance cultures is not beneficial. Positive Ssc do not predict the occurrence of catheter-related infection, and treatment of these cultures may lead to increased infection rates. negative swab: $17.32 (Canadian) positive swab : $43.32.
 patients. This study evaluated the utility of surveillance swab cultures (Ssc) of tunneled cuffed catheter. (TCC) exit sites as a prediction and prevention strategy for infection. A 6-month prospective-controlled. trial with 94 chronic HD patients with a TCC who received monthly Ssc and were stratified by. dialysis day into topical therapy based on Ssc results (Group A) or no therapy (Group B). Outcomes. were exit site infection (ESI) and catheter-associated bacteremia (CAB). The overall monthly prevalence. of positive Ssc was 14.9%. There was no difference in the number of positive Ssc (17.7% vs. 11.6%, p40.05) or ESI (19.6% vs.16.3%, p40.05) between Groups A and B, respectively. Catheterassociated. bacteremia was higher in Group A (17.7% vs. 4.7%, p=0.05). There were significantly. more ESI in the patients treated for a positive Ssc. In Group A, the incidence of ESI was significantly. higher in those treated for a positive vs. negative Ssc (55% vs. 12%, p=0.009) and CAB rates trended. higher with positive Ssc (22.2% vs. 16.7%, p40.05). The strategy of treating positive surveillance. cultures is not beneficial. Positive Ssc do not predict the occurrence of catheter-related infection, and. treatment of these cultures may lead to increased infection rates. negative swab: $17.32 (Canadian) positive swab : $")
43
Prélèvements cutanés orientés
132 Kt, hématologie, culture (Maki +Sheretz) Cultures systématiques tous les mois vs Culture en cas de suspicion d'infection N 87 15 Se 18 75 Sp 83 100 VPP 13 100 VPN 88 92 Systématiques Orientés (*) écouvillon de 24 cm 2, culture quantitative en milieu liquide Raad Clin Infect Dis 1995; 20:593 16
 Cultures systématiques tous les mois vs Culture en cas de suspicion d infection. N Se Sp VPP VPN Systématiques. Orientés. (*) écouvillon de 24 cm 2, culture quantitative en milieu liquide. Raad Clin Infect Dis 1995; 20:")
44
Les prélèvements cutanés et du pavillon
EN CAS DE SUSPICION D’INFECTION+++ Des prélèvements stériles permettent d'éviter une ablation de KT inutile Par contre, des prélèvements positifs n'ont que peu de valeur diagnostique 17

45
Paired quantitative blood cultures
Diagnosis of Catheter - Related Infections Paired quantitative blood cultures Wing (1979): catheter - related infection (E. cloacæ & C. freundii) 25 col. / ml on the blood culture drawn on peripheral vein 104 col. / ml on the blood culture drawn on the catheter N° CVC Setting Method Tip-culture Ratio Sens. Spec. Flynn (1987): Children Direct inoc SQC : ND ND Flynn (1988): Children Isolator SQC : ND ND Fan (1989): Adults/TPN Pour plate SQC & QC 1: % % Capdevila (1992): All hosp. Pour plate SQC : % % Douard (1991): Children Isolator 1.5 ml No cult : % 100% ( technical simplification / pediatric Isolator tubes)
: catheter - related infection (E. cloacæ & C. freundii) 25 col. / ml on the blood culture drawn on peripheral vein. 104 col. / ml on the blood culture drawn on the catheter. N° CVC Setting Method Tip-culture Ratio Sens. Spec. Flynn (1987): 31 Children Direct inoc. SQC 1:5 ND ND. Flynn (1988): 13 Children Isolator SQC 1:5 ND ND. Fan (1989): 24 Adults/TPN Pour plate SQC & QC 1:7 78% 100% Capdevila (1992): 107 All hosp. Pour plate SQC 1:4 94% 100% Douard (1991): 50 Children Isolator 1.5 ml No cult. 1:3 83% 100% ( technical simplification / pediatric Isolator tubes)")
46
Diagnosis of Catheter - Related Infections
CONTINUOUS MONITORING BLOOD CULTURE SYSTEMS IN THE DIAGNOSIS OF CRI Time to positivity of blood cultures hours Clinical study: 7 patients with "probable" CRI Same time to positivity, whether aerobic or anaerobic bottles are used Mean DTP = 4.1 hours Only 3 / 7 cases with DTP > 2 hours (Bact/Alert system) 18 16 14 12 Aer Ana Serial dilutions (coagulase negative staphylococci) MS. Rogers & BA. Oppenheim. J Clin Pathol 1998; 51:
 Aer. Ana Serial dilutions (coagulase negative staphylococci) MS. Rogers & BA. Oppenheim. J Clin Pathol 1998; 51:")
47
Blot F - Lancet ; 354: 14 mois, 93 suspicions d ’ILC CVC courte et longue durée, dispositifs implantables Paires d ’hémocultures et ablation du KT dans les 48 heures Sp: 91 (95% CI %) Se: 94 (95% CI %)
 Se: 94 (95% CI %)")
48
Effets de la durée d’insertion du cathéter sur la valeur diagnostique du DTP
Raad et al – Ann Intern Med 2004; 140:18-25

49
Endoluminal colonization: in which lumen
Endoluminal colonization: in which lumen? Dobbins et al – CCM 2003; 31: 1688 CVCs not suspected No CRBSI (n=50) CVCs suspected (n=25) CRBSI N lumens colonized* 1 2 3 6 4 10 5 N CVCs Maki roll + 28 14 20 (*) endoluminal brushes> 100 CFUs
 CVCs suspected. (n=25) CRBSI. N lumens colonized* N CVCs Maki roll (*) endoluminal brushes> 100 CFUs.")
50
positivity, and endoluminal brushing
In situ diagnosis of intravascular catheter-related bloodstream infection: A comparison of quantitative culture, differential time to positivity, and endoluminal brushing Catton et al – Crit Care Med 2005; 33:787 Objective: To compare the accuracy of three techniques that do not require central venous catheter removal to diagnose catheter- related bloodstream infection. Design: Prospective cohort study of central venous catheters from suspected cases of catheter-related bloodstream infection. Setting: University teaching hospital. Patients: One hundred and twenty-five central venous catheters from patients with suspected catheter-related bloodstream infection (a raised peripheral white blood cell count, temperature >37°C, and/or local signs of infection at the catheter skin entry site) in intensive care and surgical patients in a large teaching hospital were assessed. Interventions: None. Measurements: Three techniques were compared: the differential time to positivity of central venous catheter vs. peripheralblood cultures, quantitative culture of central venous catheter vs. peripheral blood, and the endoluminal brush with peripheral blood culture. Main Results: Central venous catheters with a median dwell time of 11 days were examined. There were 36 episodes of catheter-related bloodstream infection, defined as a positive result from at least two of the three tests in the presence of a peripheral blood culture growing the same microorganism and without an identifiable alternative source of sepsis. The sensitivities of the endoluminal brush, quantitative culture, and differential time to positivity techniques were 100%, 89%, and 72%, respectively, with corresponding specificities of 89%, 97%, and 95%. Blood could be directly aspirated from only 231 of 312 (74%) lumens. In the 20 cases of catheter-related bloodstream infection associated with multiple-lumen central venous catheters, endoluminal brushing was positive for one, two, and three lumens in nine (45%), six (30%), and five (25%) cases, respectively. Conclusions: All three techniques had relatively high sensitivity. However, inability to obtain samples via central venous catheters is a major drawback of the differential time to positivity and quantitative blood culture approaches. Differential time to positivity is simple to perform and has high specificity and therefore could be used as a first line approach, with the endoluminal brush reserved for cases where blood cannot be obtained. All lumens of multiple-lumen central venous catheters must be sampled to ensure maximal sensitivity. (Crit Care Med 2005; 33:787–791) KEY WORDS: central venous catheter; catheter-related bloodstream infection; differential time to positivity; quantitative culture; endoluminal brush Population: One hundred and twenty-five CVCs were examined from 119 patients. No patients had catheters impregnated with antibiotics or antiseptic, and none received immunosuppressive dosages of systemic steroids. The following types of catheter were assessed: 25 Hickman catheters (21 single lumen and four double) and 18 single-, 63 triple-, and 19 quadruple- lumen MLCVCs. The median catheter dwell time was 11 days (range, 2–712).
 in intensive care and surgical patients in a large teaching. hospital were assessed. Interventions: None. Measurements: Three techniques were compared: the differential. time to positivity of central venous catheter vs. peripheralblood. cultures, quantitative culture of central venous catheter vs. peripheral blood, and the endoluminal brush with peripheral blood. culture. Main Results: Central venous catheters with a median dwell. time of 11 days were examined. There were 36 episodes of. catheter-related bloodstream infection, defined as a positive result. from at least two of the three tests in the presence of a. peripheral blood culture growing the same microorganism and. without an identifiable alternative source of sepsis. The sensitivities. of the endoluminal brush, quantitative culture, and differential. time to positivity techniques were 100%, 89%, and 72%, respectively, with corresponding specificities of 89%, 97%, and. 95%. Blood could be directly aspirated from only 231 of 312 (74%) lumens. In the 20 cases of catheter-related bloodstream infection. associated with multiple-lumen central venous catheters, endoluminal. brushing was positive for one, two, and three lumens in. nine (45%), six (30%), and five (25%) cases, respectively. Conclusions: All three techniques had relatively high sensitivity. However, inability to obtain samples via central venous catheters. is a major drawback of the differential time to positivity and. quantitative blood culture approaches. Differential time to positivity. is simple to perform and has high specificity and therefore. could be used as a first line approach, with the endoluminal brush. reserved for cases where blood cannot be obtained. All lumens of. multiple-lumen central venous catheters must be sampled to. ensure maximal sensitivity. (Crit Care Med 2005; 33:787–791) KEY WORDS: central venous catheter; catheter-related bloodstream. infection; differential time to positivity; quantitative culture; endoluminal brush. Population: One hundred and twenty-five. CVCs were examined from 119 patients. No patients had catheters impregnated. with antibiotics or antiseptic, and none. received immunosuppressive dosages of. systemic steroids. The following types of. catheter were assessed: 25 Hickman catheters. (21 single lumen and four double) and 18 single-, 63 triple-, and 19 quadruple- lumen MLCVCs. The median catheter. dwell time was 11 days (range, 2–712).")
51
Test diagnostic rapide
Kite; Lancet 1999; 354:1504 100 µL de sang par le KTC Traitement par l'acide édétique lyse et centrifugation puis pastilles de cytocentrifugation puis coloration acridine orange et Gram 100 champs, 2 colorations Gram + AOLC test Positif Négatif ILC+ 48 2 ILC- 5 57

52
AOLC as a screening test
Bong et al –JPEN 2003; 27:146 Suspected CR-BSI 50 AOLC Positive: 10 Immediate removal Negative 40 CVC left in place 4 CR-BSI 10 CR-BSI Lifespan of CVCs: Med 24 days vs 11 in case of immediate removal (p<0.0001)
")
53
MRSA carriage at insertion
Jean G et al – Nephron 2002; 91:399 No Nasal SA (58) nasal SA (31) Age 68 58.6** Peripheral atherosclerosis 15.5% 39%* History of bact. 40% 65% Months on dialysis 62 59 End of the study CVC surv. 482 720* Nb of bacteremia 0.2 0.6 1.6 1.6*** Bacteremic patients 12% 80%*** Local infect. * p<0.05 **p<0.001 ***p<0.0001
 nasal SA (31) Age ** Peripheral atherosclerosis. 15.5% 39%* History of bact. 40% 65% Months on dialysis End of the study. CVC surv * Nb of bacteremia. 0.2 1.6*** Bacteremic patients. 12% 80%*** Local infect. * p<0.05. **p< ***p<")
54
Mupirocin.(meta-analysis).is effective..
But emergence of resistant strains is frequent Mupirocin Prophylaxis to Prevent Staphylococcus aureus Infection in Patients Undergoing Dialysis: A Meta-analysis Evelina Tacconelli,1 Yehuda Carmeli,1,5 Anthony Aizer,2 Gabriela A systematic review of the English-language literature was performed to determine the overall benefit of mupirocin therapy in reducing the rate of Staphylococcus aureus infection among patients undergoing hemodialysis (HD) or peritoneal dialysis (PD). Included studies met the following criteria: they were randomized clinical trials or cohort studies; cohorts consisted of adults (age, 18 years) requiring HD or PD; mupirocin therapy was administered to the treatment group, and placebo or no therapy was administered to the control group; and the primary outcome of interest was the difference in the number of S. aureus infections among mupirocin-treated and -untreated patients. Ten studies described in 9 articles were analyzed. A total of 2445 patients were included in the analysis. Use of mupirocin reduced the rate of S. aureus infections by 68% (95% confidence interval [CI], 57%76%) among all patients undergoing dialysis; risk reductions were 80% (95% CI, 65%89%) among patients undergoing HD and 63% (95% CI, 50%73%) among patients undergoing PD. When data were stratified by type of infection, S. aureus bacteremia was found to be reduced by 78% among patients undergoing HD, and peritonitis and exit-site infections were found to be reduced by 66% and 62%, respectively, among patients undergoing PD. Mupirocin prophylaxis substantially reduces the rate of S. aureus infection in the dialysis population. Optimal regimens that minimize the emergence of mupirocin resistance need to be explored. Taconelli et al- 2003;37:
 or peritoneal dialysis (PD). Included studies met the following criteria: they were randomized clinical trials or cohort studies; cohorts consisted of adults (age, 18 years) requiring HD or PD; mupirocin therapy was administered to the treatment group, and placebo or no therapy was administered to the control group; and the primary outcome of interest was the difference in the number of S. aureus infections among mupirocin-treated and -untreated patients. Ten studies described in 9 articles were analyzed. A total of 2445 patients were included in the analysis. Use of mupirocin reduced the rate of S. aureus infections by 68% (95% confidence interval [CI], 57%76%) among all patients undergoing dialysis; risk reductions were 80% (95% CI, 65%89%) among patients undergoing HD and 63% (95% CI, 50%73%) among patients undergoing PD. When data were stratified by type of infection, S. aureus bacteremia was found to be reduced by 78% among patients undergoing HD, and peritonitis and exit-site infections were found to be reduced by 66% and 62%, respectively, among patients undergoing PD. Mupirocin prophylaxis substantially reduces the rate of S. aureus infection in the dialysis population. Optimal regimens that minimize the emergence of mupirocin resistance need to be explored. Taconelli et al- 2003;37:")
55
N’y a t-il que la mupirocine???
Randomized, Controlled Trial of Topical Exit-Site Application of Honey (Medihoney) versus Mupirocin for the Prevention of Catheter-Associated Infections in Hemodialysis Patients Johnson et al- J Am Soc Nephrol 16: 1456–1462, 2005. N’y a t-il que la mupirocine??? The clinical usefulness of hemodialysis catheters is limited by increased infectious morbidity and mortality. Topical antiseptic agents, such as mupirocin, are effective at reducing this risk but have been reported to select for antibiotic-resistant strains. The aim of the present study was to determine the efficacy and the safety of exit-site application of a standardized antibacterial honey versus mupirocin in preventing catheter-associated infections. A randomized, controlled trial was performed comparing the effect of thrice-weekly exit-site application of Medihoney versus mupirocin on infection rates in patients who were receiving hemodialysis via tunneled, cuffed central venous catheters. A total of 101 patients were enrolled. The incidences of catheter-associated bacteremias in honey-treated (n 51) and mupirocin-treated (n 50) patients were comparable (0.97 versus 0.85 episodes per 1000 catheter-days, respectively; NS). On Cox proportional hazards model analysis, the use of honey was not significantly associated with bacteremia-free survival (unadjusted hazard ratio, 0.94; 95% confidence interval, 0.27 to 3.24; P 0.92). No exit-site infections occurred. During the study period, 2% of staphylococcal isolates within the hospital were mupirocin resistant. Thrice-weekly application of standardized antibacterial honey to hemodialysis catheter exit sites was safe, cheap, and effective and resulted in a comparable rate of catheter-associated infection to that obtained with mupirocin (although the study was not adequately powered to assess therapeutic equivalence). The effectiveness of honey against antibiotic-resistant microorganisms and its low likelihood of selecting for further resistant strains suggest that this agent may represent a satisfactory alternative means of chemoprophylaxis in patients with central venous catheters.
 versus Mupirocin for the Prevention of Catheter-Associated Infections in Hemodialysis Patients. Johnson et al- J Am Soc Nephrol 16: 1456–1462, N’y a t-il que la mupirocine The clinical usefulness of hemodialysis catheters is limited by increased infectious morbidity and mortality. Topical antiseptic. agents, such as mupirocin, are effective at reducing this risk but have been reported to select for antibiotic-resistant strains. The aim of the present study was to determine the efficacy and the safety of exit-site application of a standardized antibacterial. honey versus mupirocin in preventing catheter-associated infections. A randomized, controlled trial was performed comparing. the effect of thrice-weekly exit-site application of Medihoney versus mupirocin on infection rates in patients who were. receiving hemodialysis via tunneled, cuffed central venous catheters. A total of 101 patients were enrolled. The incidences of. catheter-associated bacteremias in honey-treated (n 51) and mupirocin-treated (n 50) patients were comparable (0.97 versus episodes per 1000 catheter-days, respectively; NS). On Cox proportional hazards model analysis, the use of honey was not. significantly associated with bacteremia-free survival (unadjusted hazard ratio, 0.94; 95% confidence interval, 0.27 to 3.24; P. 0.92). No exit-site infections occurred. During the study period, 2% of staphylococcal isolates within the hospital were. mupirocin resistant. Thrice-weekly application of standardized antibacterial honey to hemodialysis catheter exit sites was. safe, cheap, and effective and resulted in a comparable rate of catheter-associated infection to that obtained with mupirocin. (although the study was not adequately powered to assess therapeutic equivalence). The effectiveness of honey against. antibiotic-resistant microorganisms and its low likelihood of selecting for further resistant strains suggest that this agent may. represent a satisfactory alternative means of chemoprophylaxis in patients with central venous catheters.")
56
Politique D’ACQ: * Communication sur ILC Optimisation de la culture?
Prevention VAP * Background Catheter-related bloodstream infections occurring in the intensive care unit (ICU) are common, costly, and potentially lethal. Methods We conducted a collaborative cohort study predominantly in ICUs in Michigan. An evidence-based intervention was used to reduce the incidence of catheter-related bloodstream infections. Multilevel Poisson regression modeling was used to compare infection rates before, during, and up to 18 months after implementation of the study intervention. Rates of infection per 1000 catheter-days were measured at 3-month intervals, according to the guidelines of the National Nosocomial Infections Surveillance System. Results A total of 108 ICUs agreed to participate in the study, and 103 reported data. The analysis included 1981 ICU-months of data and 375,757 catheter-days. The median rate of catheter-related bloodstream infection per 1000 catheter-days decreased from 2.7 infections at baseline to 0 at 3 months after implementation of the study intervention (P≤0.002), and the mean rate per 1000 catheter-days decreased from 7.7 at baseline to 1.4 at 16 to 18 months of follow-up (P<0.002). The regression model showed a significant decrease in infection rates from baseline, with incidence-rate ratios continuously decreasing from 0.62 (95% confidence interval [CI], 0.47 to 0.81) at 0 to 3 months after implementation of the intervention to 0.34 (95% CI, 0.23 to 0.50) at 16 to 18 months. Conclusions An evidence-based intervention resulted in a large and sustained reduction (up to 66%) in rates of catheter-related bloodstream infection that was maintained throughout the 18-month study period. (*) definitions du NNISS…
 are common, costly, and potentially lethal. Methods. We conducted a collaborative cohort study predominantly in ICUs in Michigan. An. evidence-based intervention was used to reduce the incidence of catheter-related. bloodstream infections. Multilevel Poisson regression modeling was used to compare. infection rates before, during, and up to 18 months after implementation of. the study intervention. Rates of infection per 1000 catheter-days were measured at. 3-month intervals, according to the guidelines of the National Nosocomial Infections. Surveillance System. Results. A total of 108 ICUs agreed to participate in the study, and 103 reported data. The. analysis included 1981 ICU-months of data and 375,757 catheter-days. The median. rate of catheter-related bloodstream infection per 1000 catheter-days decreased. from 2.7 infections at baseline to 0 at 3 months after implementation of the study. intervention (P≤0.002), and the mean rate per 1000 catheter-days decreased from. 7.7 at baseline to 1.4 at 16 to 18 months of follow-up (P<0.002). The regression model. showed a significant decrease in infection rates from baseline, with incidence-rate. ratios continuously decreasing from 0.62 (95% confidence interval [CI], 0.47 to 0.81) at 0 to 3 months after implementation of the intervention to 0.34 (95% CI, 0.23 to. 0.50) at 16 to 18 months. Conclusions. An evidence-based intervention resulted in a large and sustained reduction (up to 66%) in rates of catheter-related bloodstream infection that was maintained throughout. the 18-month study period. (*) definitions du NNISS…")
57
A Multicenter Intervention to Prevent Catheter-Associated Bloodstream Infections David K. Warren et al for the Prevention Epicenter Program Infect Control Hosp Epidemiol 2006; 27: 12 ICU, 1 BMT unit, 6 centers Written policies, 9-page self-study module and self-evaluation, didactic lectures, and incorporation into practice of evidence-based guidelines The percentage of CVCs inserted into the femoral vein 12.9% to 9.4% (relative ratio, 0.73; 95% confidence interval [CI], ) The total proportion of catheter insertion site dressings properly dated 26.6% to 34.4% (relative ratio, 1.29; 95% CI, ), The overall rate of catheter-associated BSI 11.2 to 8.9 infections per 1,000 catheter-days (relative rate, 0.79; 95% CI, ). background. Education-based interventions can reduce the incidence of catheter-associated bloodstream infection. The generalizability of findings from single-center studies is limited. objective. To assess the effect of a multicenter intervention to prevent catheter-associated bloodstream infections. design. An observational study with a planned intervention. setting. Twelve intensive care units and 1 bone marrow transplantation unit at 6 academic medical centers. patients. Patients admitted during the study period. intervention. Updates of written policies, distribution of a 9-page self-study module with accompanying pretest and posttest, didactic lectures, and incorporation into practice of evidence-based guidelines regarding central venous catheter (CVC) insertion and care. measurements. Standard data collection tools and definitions were used to measure the process of care (ie, the proportion of nontunneled catheters inserted into the femoral vein and the condition of the CVC insertion site dressing for both tunneled and nontunneled catheters) and the incidence of catheter-associated bloodstream infection. results. Between the preintervention period and the postintervention period, the percentage of CVCs inserted into the femoral vein decreased from 12.9% to 9.4% (relative ratio, 0.73; 95% confidence interval [CI], ); the total proportion of catheter insertion site dressings properly dated increased from 26.6% to 34.4% (relative ratio, 1.29; 95% CI, ), and the overall rate of catheter-associated bloodstream infections decreased from 11.2 to 8.9 infections per 1,000 catheter-days (relative rate, 0.79; 95% CI, ). The effect of the intervention varied among individual units. conclusions. An education-based intervention that uses evidence-based practices can be successfully implemented in a diverse group of medical and surgical units and reduce catheter-associated bloodstream infection rates. Infect Control Hosp Epidemiol 2006; 27: From the Department of Medicine, Washington University School of Medicine, Saint Louis, Missouri (D.K.W., V.J.F.); the Department of Public Health and Hygiene, Johns Hopkins School of Hygiene and Public Health, Baltimore, Maryland (S.E.G., T.M.P.); the Department of Internal Medicine, University of Iowa College of Medicine, Iowa City, Iowa (D.J.D., L.A.H.); the Department of Medicine (G.Z.) and the Department of Internal Medicine (K.A.S.), Memorial Sloan-Kettering Cancer Center, New York, New York; the Department of Internal Medicine, Hunter Holmes McGuire Veterans Affairs Medical Center, Richmond, Virginia (M.W.C., E.S.W.); the Department of Internal Medicine, Northwestern University, Feinberg School of Medicine, Chicago, Illinois (M.K.B., G.A.N.); and the Division of Healthcare Quality Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia (J.I.T., S.L.S.). Received March 30, 2006; accepted May 25, 2006; electronically published June 9, 2006. 2006 by The Society for Healthcare Epidemiology of America. All rights reserved X/2006/ $15.00. Central venous catheters (CVCs) are indispensable in the care of critically ill patients. However, their use is not without risk. Catheter-associated bloodstream infections (CA-BSIs) are common healthcare-associated infections in intensive care unit (ICU) patients1 and have been estimated to occur in 3%- 7% of all patients with CVCs.2 Nontunneled CVCs are the most frequently used devices in ICUs. Despite being used for relatively brief periods, these catheters are associated with a higher rate of infection than are tunneled catheters or totally implanted ports, which are used for relatively longer periods.3 Use of newer devices such as antimicrobial- and antisepticimpregnated CVCs reduces the risk of CA-BSI4-7; however, use of these devices may not be more effective than ensuring use of appropriate methods for insertion, use, and care of CVCs. Practices that reduce the risk of CA-BSIs include the following: (1) use of maximal barrier precautions during CVC insertion (ie, a surgical mask, sterile gown, sterile gloves, and large sterile drapes),8,9 (2) placement of the catheter in the subclavian vein rather than the internal jugular or femoral vein,10,11 (3) changing catheters only when necessary,12,13 and
 The total proportion of catheter insertion site dressings properly dated. 26.6% to 34.4% (relative ratio, 1.29; 95% CI, ), The overall rate of catheter-associated BSI to 8.9 infections per 1,000 catheter-days (relative rate, 0.79; 95% CI, ). background. Education-based interventions can reduce the incidence of catheter-associated bloodstream infection. The generalizability. of findings from single-center studies is limited. objective. To assess the effect of a multicenter intervention to prevent catheter-associated bloodstream infections. design. An observational study with a planned intervention. setting. Twelve intensive care units and 1 bone marrow transplantation unit at 6 academic medical centers. patients. Patients admitted during the study period. intervention. Updates of written policies, distribution of a 9-page self-study module with accompanying pretest and posttest, didactic. lectures, and incorporation into practice of evidence-based guidelines regarding central venous catheter (CVC) insertion and care. measurements. Standard data collection tools and definitions were used to measure the process of care (ie, the proportion of nontunneled. catheters inserted into the femoral vein and the condition of the CVC insertion site dressing for both tunneled and nontunneled. catheters) and the incidence of catheter-associated bloodstream infection. results. Between the preintervention period and the postintervention period, the percentage of CVCs inserted into the femoral vein. decreased from 12.9% to 9.4% (relative ratio, 0.73; 95% confidence interval [CI], ); the total proportion of catheter insertion site. dressings properly dated increased from 26.6% to 34.4% (relative ratio, 1.29; 95% CI, ), and the overall rate of catheter-associated. bloodstream infections decreased from 11.2 to 8.9 infections per 1,000 catheter-days (relative rate, 0.79; 95% CI, ). The effect of. the intervention varied among individual units. conclusions. An education-based intervention that uses evidence-based practices can be successfully implemented in a diverse group. of medical and surgical units and reduce catheter-associated bloodstream infection rates. Infect Control Hosp Epidemiol 2006; 27: From the Department of Medicine, Washington University School of Medicine, Saint Louis, Missouri (D.K.W., V.J.F.); the Department of Public Health. and Hygiene, Johns Hopkins School of Hygiene and Public Health, Baltimore, Maryland (S.E.G., T.M.P.); the Department of Internal Medicine, University. of Iowa College of Medicine, Iowa City, Iowa (D.J.D., L.A.H.); the Department of Medicine (G.Z.) and the Department of Internal Medicine (K.A.S.), Memorial Sloan-Kettering Cancer Center, New York, New York; the Department of Internal Medicine, Hunter Holmes McGuire Veterans Affairs Medical. Center, Richmond, Virginia (M.W.C., E.S.W.); the Department of Internal Medicine, Northwestern University, Feinberg School of Medicine, Chicago, Illinois. (M.K.B., G.A.N.); and the Division of Healthcare Quality Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia (J.I.T., S.L.S.). Received March 30, 2006; accepted May 25, 2006; electronically published June 9, by The Society for Healthcare Epidemiology of America. All rights reserved X/2006/ $ Central venous catheters (CVCs) are indispensable in the care. of critically ill patients. However, their use is not without risk. Catheter-associated bloodstream infections (CA-BSIs) are. common healthcare-associated infections in intensive care. unit (ICU) patients1 and have been estimated to occur in 3%- 7% of all patients with CVCs.2 Nontunneled CVCs are the. most frequently used devices in ICUs. Despite being used for. relatively brief periods, these catheters are associated with a. higher rate of infection than are tunneled catheters or totally. implanted ports, which are used for relatively longer periods.3. Use of newer devices such as antimicrobial- and antisepticimpregnated. CVCs reduces the risk of CA-BSI4-7; however, use of these devices may not be more effective than ensuring. use of appropriate methods for insertion, use, and care of. CVCs. Practices that reduce the risk of CA-BSIs include the. following: (1) use of maximal barrier precautions during CVC. insertion (ie, a surgical mask, sterile gown, sterile gloves, and. large sterile drapes),8,9 (2) placement of the catheter in the. subclavian vein rather than the internal jugular or femoral. vein,10,11 (3) changing catheters only when necessary,12,13 and.")
Présentations similaires

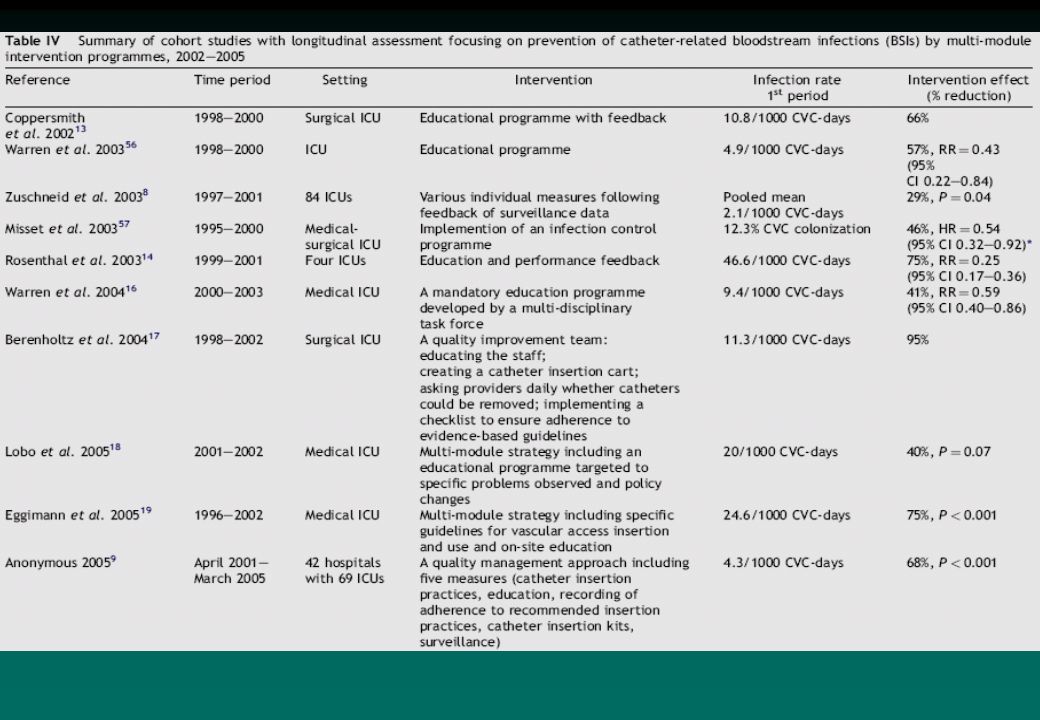




>")














 to the verb: - Il coûte… - Elle coûte… - Ils coûtent… - Elles coûtent…>")