Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Valvulopathies aortiques Le plus souvent : remplacement Prothèse Bioprothèse ROSS : quel avantage ?

2
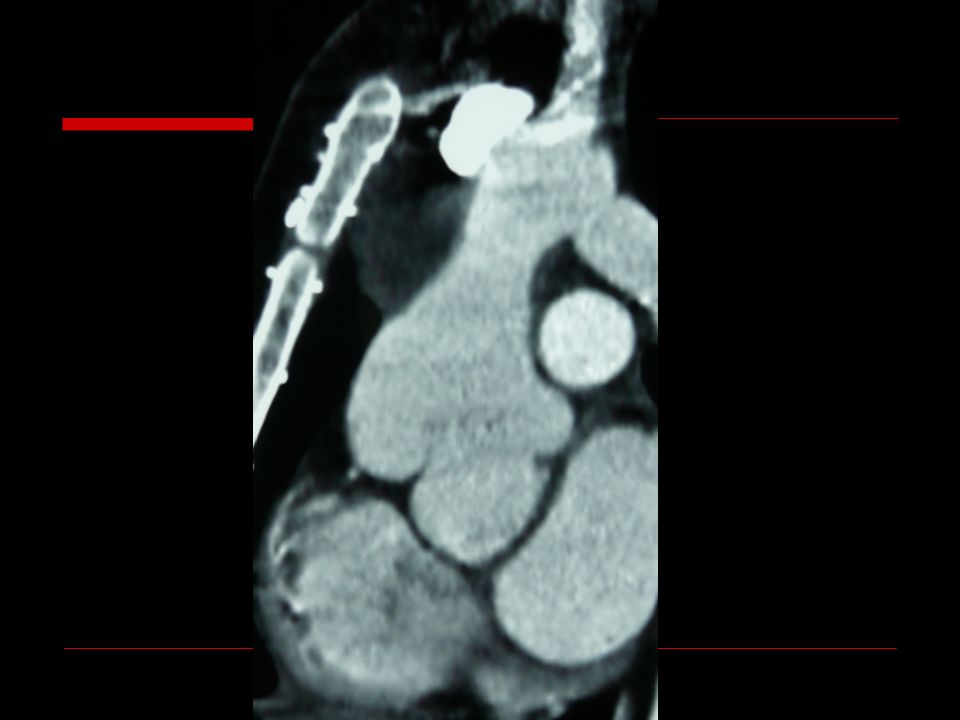
Principe de l’opération de ROSS

4
Ross Procedure replacement of the Aortic Valve or Root with a Pulmonary Autograft Donald ROSS in 1967 First report of US series by Selzer and Elkins in 1987 First done in Strasbourg in 1997 Substantial experiences accumulated worldwide over the last 25 years

5
Avantages attendus Absence d’anticoagulants Résistance aux infections Durabilité Qualités hémodynamiques Croissance potentielle IDEAL ?

6
Strasbourg n=46

7
2 populations ? A B 18 16

8
Population / Age

9
Démographie 21 h 13 f A B Insuffisance ao27 Rétrécissement169 Endocardite23 Antcd cong 6 dilatations (1=2x) 1 / CIV+CIA+Hypopl crosse 2 endovasc « à distance » (Coarctation - Canal) NYHA 1,942,15 IA (1/4) 2,42,6 RA (mmHg) 7063 ns
 1 / CIV+CIA+Hypopl crosse 2 endovasc « à distance » (Coarctation - Canal) NYHA 1,942,15 IA (1/4) 2,42,6 RA (mmHg) 7063 ns")
10
Ross n=46

11
Intervention

12
Results : early and late Mortality : 0 Hemorrhage0 Thromboembolism0 Infection0 Pace maker2 Reoperations5 Dilatation1

13
SURVIE Recul jusqu’à 13 ans Recul cummulé 242 années/patient Recul moyen 6,05 ans Décès tardif = 0 Mais Sujets jeunes Bon VG

14
Problèmes et incidents techniques Valve pulmonaire bicuspide (2) Epaisseur variable du manchon infundibulaire (très fin) Prélèvement au contact d’une cusp pulmonaire Blessure (± nécessaire) artère infundibulaire (2) Incision d’une cusp pulmonaire (1) Déchirure manchon infundibulaire (renfort péricarde: 1) Résection excessive paroi antérieure VD (péricarde : 1) Fragilité, qualité de l’homogreffe pulmonaire 1 BAV anato chirurgie Événements dans notre expérience
 Epaisseur variable du manchon infundibulaire (très fin) Prélèvement au contact d’une cusp pulmonaire Blessure (± nécessaire) artère infundibulaire (2) Incision d’une cusp pulmonaire (1) Déchirure manchon infundibulaire (renfort péricarde: 1) Résection excessive paroi antérieure VD (péricarde : 1) Fragilité, qualité de l’homogreffe pulmonaire 1 BAV anato chirurgie Événements dans notre expérience")
15
Paramètres VG au cours du temps

16
Evolution de IA et « ra » IA/4 RA/mmhg ns

17
Evolution du gradient pulm moyen mmHg

18
Reoperations Aortic root dilatation3 2 Yacoub-David 1 Bentall Autograft insufficiency (AoI 1 trauma, 1 late)2 1 repair 1 Bentall Homograft failure (pulmonary) 11 dilatation
2 1 repair 1 Bentall Homograft failure (pulmonary) 11 dilatation")
20
Autograft dilatation

21
Autograft aortic insufficiency N=2 1 repair1 Bentall

22
Freedom from surgical deterioration

23
Freedom all reoperations (or Dilatation) N = 5/46
 N = 5/46")
24
Results : paediatric vs adult Paediatric Adult AI YD Dilatation P.Homo

25
SURVIE Recul jusqu’à 13 ans Recul cummulé 242 années/patient Recul moyen 6,05 ans Décès tardif = 0 Mais Sujets jeunes Bon VG

26
EXCELLENT ! ??

27
QUESTIONNEMENTS Réserves chirgiens réputés Risque plus élevé sujets jeunes Transformation en maladie bi-valvulaire Menace à long terme

28
Pros Extremely low early mortality at Experiencend centers, in both adults and children Excellent 10-15 year survival, approaching that for age and sex-matched populations Low prevalence of thromboembolic and infectious complications

29
Faut-il étendre les indications ?? Indications limitées par difficulté obtention homogreffes Prélèvement chez donneurs à cœur arrêté ? Discongruence entre Ao et AP Nbre excellents résultats publiés ! Changement réglementation Prélèvement cœur arrêté ? Amplification possile Ajustements chirurgicaux ?

30
Early mortality Systematic Review and Meta-Analysis Takkenberg et al. Circulation 2009;119:222 No. Of patients Early Mortality % Cochran Q Statistics Adults only 1.7493,2 (1,5-6,6)ns Children only 6724,2 (1,4-1,4)ns Combined Ad. + ch. 2.6103,0 (1,8–4,9)ns
ns Children only 6724,2 (1,4-1,4)ns Combined Ad. + ch ,0 (1,8–4,9)ns.")
31
Incidence of other complications Nb PatientsNb events% Thrombo embolism 1660251,5% Endocarditis1660110,7% Takkenberg JJM et al The Ross Procedure: A Systematic Review and Meta-Analysis Circulation 2009;119;222-228

32
Long term survival David et al JTCVS 2010;139:68

33
Long term events David et al JTCVS 2010;139:68

34
Late follow-up David,T.E.; Woo,A.; Armstrong,S.; Maganti,M. When is the Ross operation a good option to treat aortic valve disease? J Thorac Cardiovasc Surg 2010;139:68-73 AT 15y % survival96.6 Freedom reop Pul. autograft 92.1 Fr: AI ≥ 2+62.2 Fr: AI ≥ 3+89.7 212 patients 34y±9 FU: 10.1y (3.1-18) Best results -female -aortic stenosis - Ao annulus ≤ 27mm
 Best results -female -aortic stenosis - Ao annulus ≤ 27mm.")
35
The Ross operation: a Trojan horse? Klieverik,L.M.; Takkenberg,J.J.; Bekkers,J.A.; Roos-Hesselink,J.W.; Witsenburg,M.; Bogers,A.J. The Ross operation: a Trojan horse? Eur Heart J 2007;28:1993-2000

36
Nicholas T. Kouchoukos, Paolo Masetti, Nancy J. Nickerson, Catherine F. Castner, William D. Shannon, and Victor G. Dávila-Román The Ross procedure: Long-term clinical and echocardiographic follow-up Ann. Thorac. Surg., Sep 2004; 78: 773 - 781. 91 91 36 14 9 92 36 14 9 84 35 13 9

37
Freedom from reoperation on the pulmonary autograft. Kouchoukos NT. At all. The Ross Procedure: Long-Term Clinical and Echocardiographic Follow-Up, Ann Thorac Surg 2004;78:773-781

38
Evolution despite technique (a) Actuarial freedom from proximal aorta diameter greater than 40 mm (solid line), 45 mm or greater (broken line), and 50mm or greater (dashed line) in the root group. (b) Actuarial freedom from proximal aorta diameter greater than 40 mm (solid line), 45 mm or greater (broken line), and 50 mm or greater (dashed line) in the inclusion group. De Kerchove L et al: Ross Operation in the Adult: Long-Term Outcomes After Root Replacement and Inclusion Techniques Ann Thorac Surg 2009;87:95-102, replacementinclusion
 Actuarial freedom from proximal aorta diameter greater than 40 mm (solid line), 45 mm or greater (broken line), and 50 mm or greater (dashed line) in the inclusion group. De Kerchove L et al: Ross Operation in the Adult: Long-Term Outcomes After Root Replacement and Inclusion Techniques Ann Thorac Surg 2009;87:95-102, replacementinclusion.")
39
Intervention de ROSS Evolution sur homogreffe

40
Liberté actuarielle

41
Facteurs de risque multivariés DysfonctionEchec (failure) Homogreffe aortique Diamètre < 22 mm Gradient VD/VG > 0.5 post-op Diamètre < 22 mm Âge donneur < 30 ans (!!) Durée ischémie < 2 jours Stérilisation < 12 h
 Homogreffe aortique Diamètre < 22 mm Gradient VD/VG > 0.5 post-op Diamètre < 22 mm Âge donneur < 30 ans (!!) Durée ischémie < 2 jours Stérilisation < 12 h")
42
Ross–Yacoub procedure Luciani GB et al. The Ross–Yacoub procedure for aneurysmal autograft roots: A strategy to preserve autologous pulmonary valves J Thorac Cardiovasc Surg 2010;139:536-542 126 patients FU 7.4 ±9.9 25% dilatation > 40mm or 2.1cm/m2 12 reoperations (8.9y) 2 root replacments 10 remodeling 8 Yacoub 2 sino-tubular aorta asc replacements Freedom of reop : 80% at 14y
 2 root replacments 10 remodeling 8 Yacoub 2 sino-tubular aorta asc replacements Freedom of reop : 80% at 14y.")
43
CONS Progressive dilatation of the autograft when used as a aortic root replacement Progressive ne-aortic regurgitation Either with root replacement Or inclusion techniques Progressive need for reoperation on the autograft and the allograft in the RVOT

44
Conclusions Réserver le ROSS aux enfants S’il n’y a pas de prothèse adaptée Du fait des difficultés du tt anticoagulant Uniquement après tentatives de conservation Exclure tous les autres !!

Présentations similaires





>")













