Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Pneumopathie médicamenteuse
Elodie Blanchard Service des Maladies Respiratoires CHU Bordeaux DES médecine interne 7 mars 2014

2
Plan Notions générales
Présentations cliniques et radiologiques compatibles Démarche d’imputabilité Exemples illustrés Méthotrexate Rituximab Bléomycine Autres exemples: Cyclophosphamide, carmustine …

3
Introduction « Drug-Induced Lung Disease » (DILD)
Fréquence en augmentation Présentations cliniques/radiologiques variables Délai variable par rapport à l’exposition médicamenteuse Gravité variable Diagnostic d’exclusion Diagnostic de certitude difficile à établir sans être délétère Qq jours à qq années après l’intro du médic, même parfois après l’arrêt de la molécule

4
Notions générales Matsuno, Respiratory Research, 2012

5
Tableaux radio-cliniques et anatomopathologiques
Toux isolée Voies aériennes: Bronchospasme Bronchiolite constrictive Pneumopathie infiltrante diffuse Aigüe ou suraigüe Chronique Fibrose pulmonaire Pathologie pleurale Épanchement/fibrose Pathologie vasculaire pulmonaire Embolie pulmonaire Hémorragie alvéolaire HTAP Lésions anatomopathologiques: Dommage alvéolaire diffus (DAD) Pneumopathie interstitielle non spécifique (NSIP) Fibrose pulmonaire dite idiopathique (UIP) Pneumonie organisée (OP) Pneumopathie d’hypersensibilité (HP) Hémorragie alvéolaire diffuse (AH) Granulomatose
 Pneumopathie interstitielle non spécifique (NSIP) Fibrose pulmonaire dite idiopathique (UIP) Pneumonie organisée (OP) Pneumopathie d’hypersensibilité (HP) Hémorragie alvéolaire diffuse (AH) Granulomatose.")
6
Démarche d’imputabilité
Documentation de l’exposition Eventuel bilan respiratoire pré-thérapeutique Chronologie parfois évocatrice Séméiologie clinique, radiologique, biologique, anapath Exclusion autres causes +++: Infections (terrain immunodéprimé) OAP affection sous-jacente Disparition ou diminution des symptômes lors de la diminution ou l’arrêt Episodes antérieurs similaires sous ttt
 OAP. affection sous-jacente. Disparition ou diminution des symptômes lors de la diminution ou l’arrêt. Episodes antérieurs similaires sous ttt.")
7
Critères d’imputabilité
Intrinsèque: Critère chronologique entre l’administration du médicament et la survenue de l’évènement respiratoire (suggestif/compatible/incompatible) Données séméiologiques (très vraisemblable/ vraisemblable/ compatible/ douteux/ incompatible) Extrinsèque Effet notoire (> 10 cas publiés de séméio identique / connu (< 10 cas publiés) / non décrit Mayaud, Rev Pneumol Clin, 2005
 Données séméiologiques. (très vraisemblable/ vraisemblable/ compatible/ douteux/ incompatible) Extrinsèque. Effet notoire (> 10 cas publiés de séméio identique / connu (< 10 cas publiés) / non décrit. Mayaud, Rev Pneumol Clin,")
9
*: cas isolés nécessitant confirmation
**: 10 cas publiés ***: entre 20 et 100 cas publiés ****: > 100 cas publiés

11
Facteurs de risque ? Ages extrêmes Dose Oxygène Radiothérapie
Fumeurs, fonction respiratoire altérée Pré existence de pneumopathie interstitielle Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique Schwaiblmair, Open Resp Med 2012 11

12
LBA: une orientation Formule normale: 150 000 cell/mm3
MC 80-90%, L < 15-20% PNN < 5 %, Eo < 2% Mayaud, Rev Pneumol Clin, 2005

13
Méthotrexate Grande variété des tableaux présentés
Pneumopathies d’hypersensibilité +++ Oedèmes pulmonaires non cardiogéniques Dommages alvéolaires diffus Pneumonie organisée cryptogénique (POC) Fibrose pulmonaire Hémorragies alvéolaires, asthme, … Incidence estimée patients/ Pas de relation avec dose administrée et durée exposition Souvent pendant 1ère année ttt Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique Bonniaud RMR 2006 13
 Fibrose pulmonaire. Hémorragies alvéolaires, asthme, … Incidence estimée patients/ Pas de relation avec dose administrée et durée exposition. Souvent pendant 1ère année ttt. Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique. Bonniaud RMR")
14
Méthotrexate (2) Facteurs de risque:
Âge avancé Diabète Hypoalbuminémie Syndrome restrictif: baisse de la TLCO x 10 risque PID ATCD PID Dyspnée progressive, toux sèche, fièvre GDS: hypoxémie EFR: syndrome restrictif, diminution TLCO LBA : lymphocytaire mais parfois neutrophilique/éosino STERILE +++ Bonniaud RMR 2006 14

15
Rossi S E et al. Radiographics 2000
Methotrexate-induced pulmonary toxicity in a 41-year-old woman with rheumatoid arthritis, dyspnea, and decreased DLCO. (a) Posteroanterior chest radiograph shows bilateral heterogeneous opacities in the mid to lower lung zones. (b) High-resolution CT scan shows scattered areas of ground-glass opacity, with thickened interlobular septa—the so-called crazy-paving appearance. Lung biopsy showed NSIP consistent with methotrexate-induced pulmonary toxicity. Rossi S E et al. Radiographics 2000
 Posteroanterior chest radiograph shows bilateral heterogeneous opacities in the mid to lower lung zones. (b) High-resolution CT scan shows scattered areas of ground-glass opacity, with thickened interlobular septa—the so-called crazy-paving appearance. Lung biopsy showed NSIP consistent with methotrexate-induced pulmonary toxicity. Rossi S E et al. Radiographics")
16
Méthotrexate (4) Proposition des pneumologues aux rhumatologues/internistes Le bilan initial d’une PR pourrait comporter: EFR/TLCO RP permettant de dépister une atteinte pulmonaire de la PR et d’évaluer le risque de PNP médicamenteuse Eviter le MTX si atteinte pulmonaire de la PR OU au moins si TLCO < 50% Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique Bonniaud RMR 2006 16

17
Rituximab Méta-analyse n=45 (lymphome sauf 2 PTI)
Clinique (n=37) Toux Dyspnée Fièvre Crépitants Hypoxémie Pattern radiologique (n=37) Infiltrat alvéolaire focal Verre dépoli Infiltrats alvéolaires diffus Macronodules Pattern histologique (n=11) Pneumonie organisée NSIP Fibrose pulmonaire (UIP) Dommages alvéolaires diffus Hémorragie alvéolaire 16 (43) 30 (85) 23 (62) 13 (35) 15 (37) 19 (54) 12 (34) 3 (8.5) 1 8 (5) 4 (0) 2 (0) Méta-analyse n=45 (lymphome sauf 2 PTI) 15 j après perfusion (7-21) + fréquent après 4è cycle Formes aigües ou subaigües Formes hyperaigües: SDRA Formes tardives: nodules Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique Lioté, ERJ 2010 17
 Toux. Dyspnée. Fièvre. Crépitants. Hypoxémie. Pattern radiologique (n=37) Infiltrat alvéolaire focal. Verre dépoli. Infiltrats alvéolaires diffus. Macronodules. Pattern histologique (n=11) Pneumonie organisée. NSIP. Fibrose pulmonaire (UIP) Dommages alvéolaires diffus. Hémorragie alvéolaire. 16 (43) 30 (85) 23 (62) 13 (35) 15 (37) 19 (54) 12 (34) 3 (8.5) 1. 8 (5) 4 (0) 2 (0) Méta-analyse n=45. (lymphome sauf 2 PTI) 15 j après perfusion (7-21) + fréquent après 4è cycle. Formes aigües ou subaigües. Formes hyperaigües: SDRA. Formes tardives: nodules. Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique. Lioté, ERJ")
18
Rituximab (2) UIP/NSIP/Hémorragie alvéolaire LBA : lymphocytose
6 décès (13.3%) Mécanismes: hyperaigües: relargage cytokine aigües/subaigües: hypersensibilité tardives: toxicité directe Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique Lioté, ERJ 2010 18
 Mécanismes: hyperaigües: relargage cytokine. aigües/subaigües: hypersensibilité. tardives: toxicité directe. Formes aigües ou suraigues: hypersensibilité à l’Ac anti-CD20 chimérique. Lioté, ERJ")
19
Bléomycine Principaux tableaux décrits
Bronchiolite oblitérante avec pneumonie organisée Pneumopathie d’hypersensibilité (éosinophiles) Dommages alvéolaires diffus Nodules/masses pulmonaires Pneumopathie infiltrante diffuse subaigüe Fibrose pulmonaire Pneumomédiastin Sleijfler, Chest 2001
 Dommages alvéolaires diffus. Nodules/masses pulmonaires. Pneumopathie infiltrante diffuse subaigüe. Fibrose pulmonaire. Pneumomédiastin. Sleijfler, Chest")
20
Bléomycine OP + éosinophile
Homme 44 ans Séminome médiastinal Cisplat/eto/bléo (360), cycles Rémission complète 3 mois après fin du ttt Toux, dyspnée Eosinophilie sanguine Pneumonie organisée avec infiltrats éosinophiles Ttt prednisone 70 mg permettant la normalisation Sanjaykumar Hapani, J Med Case reports 2010
, 4 cycles. Rémission complète. 3 mois après fin du ttt. Toux, dyspnée. Eosinophilie sanguine. Pneumonie organisée avec infiltrats éosinophiles. Ttt prednisone 70 mg permettant la normalisation. Sanjaykumar Hapani, J Med Case reports")
22
Bléomycine DAD Homme de 39 ans, tumeur germinale, chimio comportant de la bléomycine Toux productive et dyspnée TDM VD, épaisissement des septa interlobulaire, distorsion architecturale, bronchectasies de traction : fibrose car DAD a 1 stade avancé Épanchement pleural droit Biopsie TB: DAD phase proliférative Bleomycin-induced DAD in a 39-year-old man with a germ cell malignancy, nonproductive cough, and dyspnea. High-resolution CT scan shows scattered areas of ground-glass opacity and thickening of interlobular septa. Architectural distortion and traction bronchiectasis suggest fibrosis due to late-stage DAD. Note right pleural effusion. Transbronchial biopsy revealed findings consistent with late proliferative phase DAD. Rossi S E et al. Radiographics 2000;20:

23
Bléomycine Nodules Homme de 35 ans, tumeur germinale non séminomateuse
Toux, dyspnée, diminition de TLCO TDM: nodules périph mal définis avec halo d’apparition récente Ponction sous TDM: pas de cellules malignes Arrêt de bléo permettant la disparition complète des lésions Bleomycin-induced pulmonary toxicity in a 35-year-old man with nonseminomatous germ cell malignancy, cough, dyspnea, and decreased DLCO. Chest CT scan shows peripheral, poorly defined pulmonary nodules (arrowheads) that were not seen on prior CT scans. Transthoracic needle aspiration biopsy was negative for malignancy, and the nodules resolved after cessation of bleomycin therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 that were not seen on prior CT scans. Transthoracic needle aspiration biopsy was negative for malignancy, and the nodules resolved after cessation of bleomycin therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
24
Pneumopathie induite par la bléomycine (1)
Développement pendant ou après le traitement Toux sèche, dyspnée d’effort, fièvre Crépitants des bases Pathogénèse: Altération endothéliale et alvéolaire (cytokines/radicaux libres) Afflux de MC / L / PNN puis de fibroblastes Modèles animaux +++ Augmentation de l’expression de Fas messenger RNA ds cell endoth pulm et uprégulation du liguand d’où ttt « préventif » possible : Ag soluble Fas/Ac anti-FasL, anti-TNFalpha sécrété par MC Sleijfler, Chest 2001
 Afflux de MC / L / PNN puis de fibroblastes. Modèles animaux +++ Augmentation de l’expression de Fas messenger RNA ds cell endoth pulm et uprégulation du liguand d’où ttt « préventif » possible : Ag soluble Fas/Ac anti-FasL, anti-TNFalpha sécrété par MC. Sleijfler, Chest")
25
Pneumopathie induite par la bléomycine (2)
Homme de 63 ans traités pour tumeur germinale non séminomateuse Toux non productive, dyspnée, diminution de TLCO TDM: VD, lignes septale en regions postero basales Bleomycin-induced pulmonary toxicity in a 63-year-old man with nonseminomatous germ cell malignancy, nonproductive cough, dyspnea, and decreased DLCO. (a) Chest CT scan demonstrates subtle, subpleural areas of ground-glass and linear opacity (arrows), particularly in the posterior lung bases. (b) Follow-up chest CT scan obtained 3 months later shows increasing subpleural areas of reticular and ground-glass opacity, findings compatible with progressive fibrosis. Diagnosis of drug toxicity was based on clinical findings and the temporal relationship to bleomycin therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 Chest CT scan demonstrates subtle, subpleural areas of ground-glass and linear opacity (arrows), particularly in the posterior lung bases. (b) Follow-up chest CT scan obtained 3 months later shows increasing subpleural areas of reticular and ground-glass opacity, findings compatible with progressive fibrosis. Diagnosis of drug toxicity was based on clinical findings and the temporal relationship to bleomycin therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
26
Pneumopathie induite par la bléomycine (3)
TDM 3 mois + tard (sous ttt): majoration du VD, apparition de réticulations intra lobulaires: fibrose évolutive Figure 16b. Bleomycin-induced pulmonary toxicity in a 63-year-old man with nonseminomatous germ cell malignancy, nonproductive cough, dyspnea, and decreased DLCO. (a) Chest CT scan demonstrates subtle, subpleural areas of ground-glass and linear opacity (arrows), particularly in the posterior lung bases. (b) Follow-up chest CT scan obtained 3 months later shows increasing subpleural areas of reticular and ground-glass opacity, findings compatible with progressive fibrosis. Diagnosis of drug toxicity was based on clinical findings and the temporal relationship to bleomycin therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
: majoration du VD, apparition de réticulations intra lobulaires: fibrose évolutive. Figure 16b. Bleomycin-induced pulmonary toxicity in a 63-year-old man with nonseminomatous germ cell malignancy, nonproductive cough, dyspnea, and decreased DLCO. (a) Chest CT scan demonstrates subtle, subpleural areas of ground-glass and linear opacity (arrows), particularly in the posterior lung bases. (b) Follow-up chest CT scan obtained 3 months later shows increasing subpleural areas of reticular and ground-glass opacity, findings compatible with progressive fibrosis. Diagnosis of drug toxicity was based on clinical findings and the temporal relationship to bleomycin therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
27
Pneumopathie induite par la bléomycine (2)
Facteurs de risque Dose cumulée < 300 mg 3/5% > 500 mg 20% Age > 70 ans Insuffisance rénale Fumeur actif Radiothérapie ? Oxygénothérapie ? Traitement précoce = réversibilité Diagnostic précoce EFR : TLCO, CV TDM thorax Exclusion autres dg Traitement CTC mg/j TLCO longtemps considéré comme le marqueur le + précoce mais une étude portant sur des K testiculaires comparant 1 groupe traité par Bléo+eto+cisplat à eto+cisplat a retrouvé une diminution globale de la TLCO non significativement différente dans les 2 groupes DC la règle de stopper le ttt si diminution entre 40 et 60% de la TLCO de base n’est pas très rentable Si le patient survit, les EFR se normalisent Sleijfler, Chest 2001

28
Inhibiteur des tyrosines kinases (EGFR) Gefitinib / Erlotinib
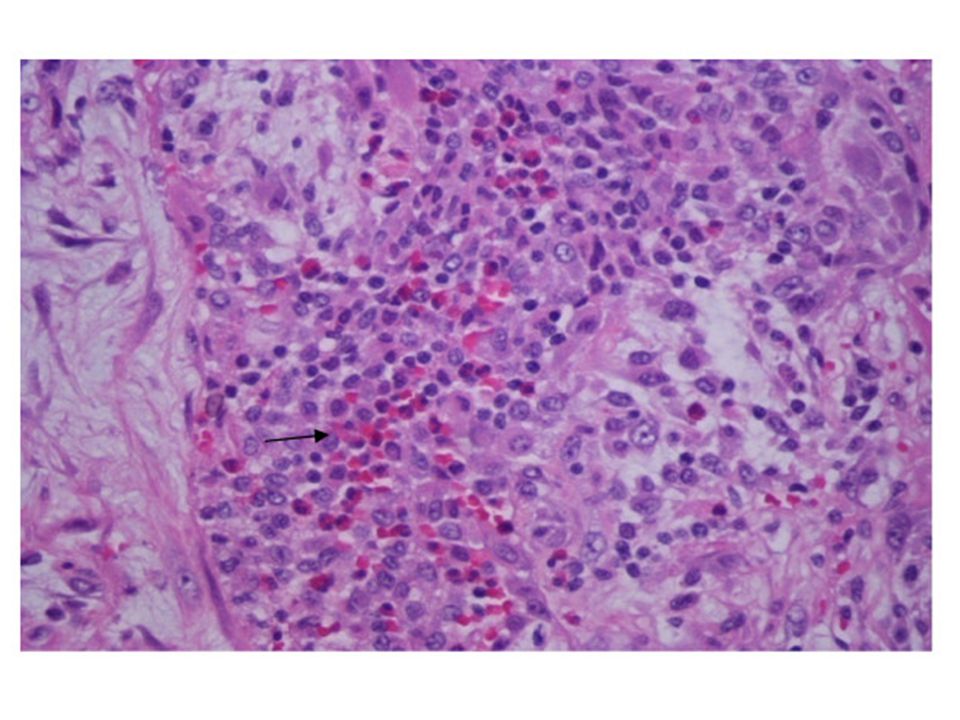
Incidence 1% (0.3-2%) 3-7 sem après début ttt Toux, dyspnée, fièvre PID aigüe Hémorragie alvéolaire Dommages alvéolaires diffus TDM : Verre dépoli Mortalité 40% FDR: japonais, tabac, homme, PID CAT: arrêt ttt + CTC Figure. Bilateral diffuse ground-glass opacities in chest CT of patient 10 (A) and haematoxylin and eosin staining of diffuse alveolar damage in the lung of patient 4 (B; magnification×40) Inoue A, Lancet 2003
 3-7 sem après début ttt. Toux, dyspnée, fièvre. PID aigüe. Hémorragie alvéolaire. Dommages alvéolaires diffus. TDM : Verre dépoli. Mortalité 40% FDR: japonais, tabac, homme, PID. CAT: arrêt ttt + CTC. Figure. Bilateral diffuse ground-glass opacities in chest CT of patient 10 (A) and haematoxylin and eosin staining of diffuse alveolar damage in the lung of patient 4 (B; magnification×40) Inoue A, Lancet")
29
A CT scan through the lung bases demonstrates consolidation with air bronchograms in the left lower lobe, an adjacent 2.4-cm nodule, and smaller nodules as well as ground-glass densities in the right lower lobe (top, A). A CT scan through a similar section of the lung 1 month later demonstrates extensive ground-glass and airspace densities throughout most of the lungs (bottom, B). Previous consolidation at the left base is still present. Liu, Chest 2007

30
Inhibiteur des tyrosines kinases (BCR-ABL) Dasatinib
Shah, JCO 2007 Epanchement pleuraux exsudatifs lymphocytaires PID (NSIP) Résolution souvent spontanée à l’arrêt Traitement diurétique / CTC In this open-label phase III trial, 670 patients with imatinib-resistant or -intolerant CP-CML (LMC, phase chronique) were randomly assigned 1:1:1:1 between four dasatinib treatment groups: 100 mg once daily, 50 mg twice daily, 140 mg once daily, or 70 mg twice daily. Results With minimum follow-up of 6 months (median treatment duration, 8 months; range, < 1 to 15 months), marked and comparable hematologic (complete, 86% to 92%) and cytogenetic (major, 54% to 59%; complete, 41% to 45%) response rates were observed across the four groups. Time to and duration of cytogenetic response were similar, as was progression-free survival (8% to 11% of patients experienced disease progression or died). Compared with the approved 70-mg twice-daily regimen, dasatinib 100 mg once daily resulted in significantly lower rates of pleural effusion (all grades, 7% v 16%; P = .024) and grade 3 to 4 thrombocytopenia (22% v 37%; P = .004), and fewer patients required dose interruption (51% v 68%), reduction (30% v 55%), or discontinuation (16% v 23%). Conclusion Dasatinib 100 mg once daily retains the efficacy of 70 mg twice daily with less toxicity. Intermittent target inhibition with tyrosine kinase inhibitors may preserve efficacy and reduce adverse events. Masiello, J Hematol Oncol, 2009
 Résolution souvent spontanée à l’arrêt. Traitement diurétique / CTC. In this open-label phase III trial, 670 patients with imatinib-resistant or -intolerant CP-CML (LMC, phase chronique) were randomly assigned 1:1:1:1 between four dasatinib treatment groups: 100 mg once daily, 50 mg twice daily, 140 mg once daily, or 70 mg twice daily. Results With minimum follow-up of 6 months (median treatment duration, 8 months; range, < 1 to 15 months), marked and comparable hematologic (complete, 86% to 92%) and cytogenetic (major, 54% to 59%; complete, 41% to 45%) response rates were observed across the four groups. Time to and duration of cytogenetic response were similar, as was progression-free survival (8% to 11% of patients experienced disease progression or died). Compared with the approved 70-mg twice-daily regimen, dasatinib 100 mg once daily resulted in significantly lower rates of pleural effusion (all grades, 7% v 16%; P = .024) and grade 3 to 4 thrombocytopenia (22% v 37%; P = .004), and fewer patients required dose interruption (51% v 68%), reduction (30% v 55%), or discontinuation (16% v 23%). Conclusion Dasatinib 100 mg once daily retains the efficacy of 70 mg twice daily with less toxicity. Intermittent target inhibition with tyrosine kinase inhibitors may preserve efficacy and reduce adverse events. Masiello, J Hematol Oncol,")
31
Different lung high-resolution computed tomography patterns
observed in patients with dasatinib-related lung abnormalities. (A) Right-sided pleural effusion (patient 1); (B) ground-glass opacities in the upper left lobe (patient 2); (C) septal thickening in the right lower lobe (patient 3); (D) alveolar consolidation in the left lower lobe associated with pleural effusion (patient 4). Bergeron, AJRCCM 2007
 Right-sided pleural effusion (patient 1); (B) ground-glass opacities in. the upper left lobe (patient 2); (C) septal thickening in the right lower. lobe (patient 3); (D) alveolar consolidation in the left lower lobe. associated with pleural effusion (patient 4). Bergeron, AJRCCM")
32
Et bien d’autres … Ipilimumab
Anti-CTLA4, 2ème ligne mélanome métastatique 03/12/2013 31/12/2013 32

33
03/12/2013 31/12/2013

34
03/12/2013 31/12/2013

35
Et bien d’autres … anti-TNF (infliximab)
SPA Toux sèche, AEG Attention BK !!!! Régression clinique et TDM à l’arrêt du TTT 01/2012 06/2012 35

36
OP NSIP DAD HP FP VA Nodule Plèvre Autres Bléomycine**** + +++
Busulfan*** ++ DIP Carmustine*** OAP MVO Cyclophosphamide *** Gemcitabine** HA MTX**** Vinblastine*** Dasatinib** Fludarabine** Rituximab** Cytarabin** Docetaxel** Tamoxifène* *: cas isolé **: 10 cas publiés ***: cas ****: > 100 cas

37
Conclusions Y penser devant quasiment toutes pneumopathies infiltrantes diffuses Exclure les autres diagnostics possibles notamment infectieux Etre rigoureux sur la démarche d’imputabilité Consulter « pneumotox » Quoiqu’il en soit, nous contacter ! ATRA Inh mTOR: LIZOT Ginette

38
Mme L.Ginette 75 ans Lymphome B diffus à grandes cellules, stade III (att gg sus et sous-diaphragmatique, Bulk épigastrique) COP de débulking le 30 juin puis mise en route d’une chimiothérapie par R CHOP 21 (C1 le 8 juillet 2011). RC après 8 cures, décision d’inclusion dans protocole d’entretien comportant un inhibiteur m-TOR Janvier 2012 : traitement par un inhibiteur m-TOR Scanners thoraciques de janvier et avril 2012 normaux Juin 2012 apparition d'une toux séche, invalidante, associée à une dyspnée au moindre effort. Initialement mise sous le compte de l'OLMETEC® (symptomatologie similaire lors d’une prise antérieure, cédant à l’arrêt), persistance malgré l’arrêt
. RC après 8 cures, décision d’inclusion dans protocole d’entretien comportant un inhibiteur m-TOR. Janvier 2012 : traitement par un inhibiteur m-TOR Scanners thoraciques de janvier et avril 2012 normaux. Juin 2012 apparition d une toux séche, invalidante, associée à une dyspnée au moindre effort. Initialement mise sous le compte de l OLMETEC® (symptomatologie similaire lors d’une prise antérieure, cédant à l’arrêt), persistance malgré l’arrêt.")
39
Mme L. Ginette Examen clinique Toux sèche, dyspnée d’effort
Discrets crépitants des bases Examens complémentaires NFS: lymphopénie 670/mm3 Fibro bronchique: macroscopiquement normal LBA : éléments, 53% lymphocytes (89% CD4) Bactério, PCR virales/pneumocystis négatives
 Bactério, PCR virales/pneumocystis négatives.")
40
date 31/08/2012 CPT % 92 CV % 102 VEMS % 104 VEMS/CV 83 DEMM % 95 VR % 101 PO2 78 PCO2 33 TLCO % 88 Test de marche 310m réalisés soit 69%th, dyspnée stade 4 tout au long de l'examen. Pas de désaturation (95-98%O2),
,")
41
01/2012 07/2012

42
01/2012 07/2012

43
Mme L. Ginette Aspect clinique et radiologique (NSIP) compatible
Chronologie compatible Imputabilité intrinsèque

44
Mme L. Ginette Imputabilité extrinsèque

45
Daunorubicin-induced DAD in a 43-year-old man with osteosarcoma, fever, dyspnea, and decreased DLCO. High-resolution CT scan shows diffuse thickening of interlobular septa and scattered areas of ground-glass opacity, findings typical of early DAD. No organisms were cultured from transbronchial lavage specimens, and biopsy revealed findings consistent with DAD. Figure 3. Daunorubicin-induced DAD in a 43-year-old man with osteosarcoma, fever, dyspnea, and decreased DLCO. High-resolution CT scan shows diffuse thickening of interlobular septa and scattered areas of ground-glass opacity, findings typical of early DAD. No organisms were cultured from transbronchial lavage specimens, and biopsy revealed findings consistent with DAD. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America

46
Figure 6b. Vincristine and adriamycin-induced NSIP in a 68-year-old woman with myeloma, dyspnea, and fever. Figure 6b. Vincristine and adriamycin-induced NSIP in a 68-year-old woman with myeloma, dyspnea, and fever. (a) Posteroanterior chest radiograph shows bilateral heterogeneous opacities in a lower lung distribution. (b) High-resolution CT scan reveals scattered areas of ground-glass opacity and thickening of interlobular septa. Note minimal architectural distortion. Transbronchial biopsy of the right lower lobe revealed mild, immature fibrosis and mononuclear interstitial infiltrate, findings consistent with NSIP. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 Posteroanterior chest radiograph shows bilateral heterogeneous opacities in a lower lung distribution. (b) High-resolution CT scan reveals scattered areas of ground-glass opacity and thickening of interlobular septa. Note minimal architectural distortion. Transbronchial biopsy of the right lower lobe revealed mild, immature fibrosis and mononuclear interstitial infiltrate, findings consistent with NSIP. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
47
Cytarabine-induced pulmonary hemorrhage in a 30-year-old man with acute leukemia, severe dyspnea, and decreased DLCO. High-resolution CT scan shows scattered areas of ground-glass opacity and small bilateral pleural effusions. Transbronchial biopsy of the right upper lobe showed organizing hemorrhage and mild interstitial fibrosis. Figure 14b. Cytarabine-induced pulmonary hemorrhage in a 30-year-old man with acute leukemia, severe dyspnea, and decreased DLCO. (a) Posteroanterior chest radiograph shows bilateral heterogeneous opacities. (b) High-resolution CT scan shows scattered areas of ground-glass opacity and small bilateral pleural effusions. Transbronchial biopsy of the right upper lobe showed organizing hemorrhage and mild interstitial fibrosis. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 Posteroanterior chest radiograph shows bilateral heterogeneous opacities. (b) High-resolution CT scan shows scattered areas of ground-glass opacity and small bilateral pleural effusions. Transbronchial biopsy of the right upper lobe showed organizing hemorrhage and mild interstitial fibrosis. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
48
Acute carmustine pulmonary toxicity in a 23-year-old woman with grade 3 astrocytoma, dyspnea, and decreased DLCO. High-resolution CT scan filmed with narrow window settings (level, -675; window, 650) accentuates the areas of ground-glass opacity present bilaterally. Diagnosis of drug toxicity was presumed because sputum cultures were negative for infection, and the patient's symptoms resolved with cessation of carmustine therapy and administration of corticosteroids. Figure 15. Acute carmustine pulmonary toxicity in a 23-year-old woman with grade 3 astrocytoma, dyspnea, and decreased DLCO. High-resolution CT scan filmed with narrow window settings (level, -675; window, 650) accentuates the areas of ground-glass opacity present bilaterally. Diagnosis of drug toxicity was presumed because sputum cultures were negative for infection, and the patient's symptoms resolved with cessation of carmustine therapy and administration of corticosteroids. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 accentuates the areas of ground-glass opacity present bilaterally. Diagnosis of drug toxicity was presumed because sputum cultures were negative for infection, and the patient s symptoms resolved with cessation of carmustine therapy and administration of corticosteroids. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
49
Carbotaxol-induced pulmonary toxicity in a 62-year-old man with small cell lung cancer, progressive dyspnea, and fever. High-resolution CT scan shows predominantly left-sided areas of consolidation, thickening of interlobular septa, and traction bronchiectasis. Diagnosis of drug toxicity was based on clinical history, presentation, and exclusion of infection. The patient's symptoms improved following institution of corticosteroid therapy. Figure 21b. Carbotaxol-induced pulmonary toxicity in a 62-year-old man with small cell lung cancer, progressive dyspnea, and fever. (a) Posteroanterior chest radiograph shows new heterogeneous opacities in the left and right upper lobes. (b) High-resolution CT scan shows predominantly left-sided areas of consolidation, thickening of interlobular septa, and traction bronchiectasis. Diagnosis of drug toxicity was based on clinical history, presentation, and exclusion of infection. The patient's symptoms improved following institution of corticosteroid therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 Posteroanterior chest radiograph shows new heterogeneous opacities in the left and right upper lobes. (b) High-resolution CT scan shows predominantly left-sided areas of consolidation, thickening of interlobular septa, and traction bronchiectasis. Diagnosis of drug toxicity was based on clinical history, presentation, and exclusion of infection. The patient s symptoms improved following institution of corticosteroid therapy. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
50
Topotecan-induced pulmonary toxicity in a 45-year-old woman with small cell lung cancer and increasing dyspnea. Chest CT scan shows areas of ground-glass and linear opacity in the right lung and scattered opacities in the left lung. Wedge resection biopsy of the right upper lobe revealed findings of BOOP. Figure 22b. Topotecan-induced pulmonary toxicity in a 45-year-old woman with small cell lung cancer and increasing dyspnea. (a) Posteroanterior chest radiograph shows new heterogeneous opacities in the right lung. Note the mediastinal mass, consistent with small cell lung cancer. (b) Chest CT scan shows areas of ground-glass and linear opacity in the right lung and scattered opacities in the left lung. Wedge resection biopsy of the right upper lobe revealed findings of BOOP. Parfois plutôt bronchiolite constrictive Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 Posteroanterior chest radiograph shows new heterogeneous opacities in the right lung. Note the mediastinal mass, consistent with small cell lung cancer. (b) Chest CT scan shows areas of ground-glass and linear opacity in the right lung and scattered opacities in the left lung. Wedge resection biopsy of the right upper lobe revealed findings of BOOP. Parfois plutôt bronchiolite constrictive. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
51
Figure 9b. Cyclophosphamide-induced BOOP in a 72-year-old woman with malignant thymoma, fever, nonproductive cough, and dyspnea. Figure 9b. Cyclophosphamide-induced BOOP in a 72-year-old woman with malignant thymoma, fever, nonproductive cough, and dyspnea. (a) Posteroanterior chest radiograph shows scattered, poorly defined peripheral opacities (arrows). (b) Follow-up posteroanterior chest radiograph obtained 2 weeks later shows progressive peripheral consolidation. Wedge resection biopsy of the middle lobe revealed findings of BOOP. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
 Posteroanterior chest radiograph shows scattered, poorly defined peripheral opacities (arrows). (b) Follow-up posteroanterior chest radiograph obtained 2 weeks later shows progressive peripheral consolidation. Wedge resection biopsy of the middle lobe revealed findings of BOOP. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
52
Figure 10. Cyclophosphamide-induced BOOP in a 42-year-old man with nodular sclerosing Hodgkin disease who presented with low-grade fever and decreased DLCO. Chest CT scan shows peripheral, poorly defined areas of focal consolidation and bronchial wall thic... Figure 10. Cyclophosphamide-induced BOOP in a 42-year-old man with nodular sclerosing Hodgkin disease who presented with low-grade fever and decreased DLCO. Chest CT scan shows peripheral, poorly defined areas of focal consolidation and bronchial wall thickening. Note moderate pericardial effusion (P). Transbronchial biopsy showed findings of BOOP. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America
. Transbronchial biopsy showed findings of BOOP. Rossi S E et al. Radiographics 2000;20: ©2000 by Radiological Society of North America.")
Présentations similaires





 de l’enfant R. Chiron, J. Donadieu.>")














