Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Evolution des connaissances sur le Reflux Gastro-oesophagien (RGO)
Rouen DES 30 mars 2012 Evolution des connaissances sur le Reflux Gastro-oesophagien (RGO) JP Galmiche
 JP Galmiche.")
2
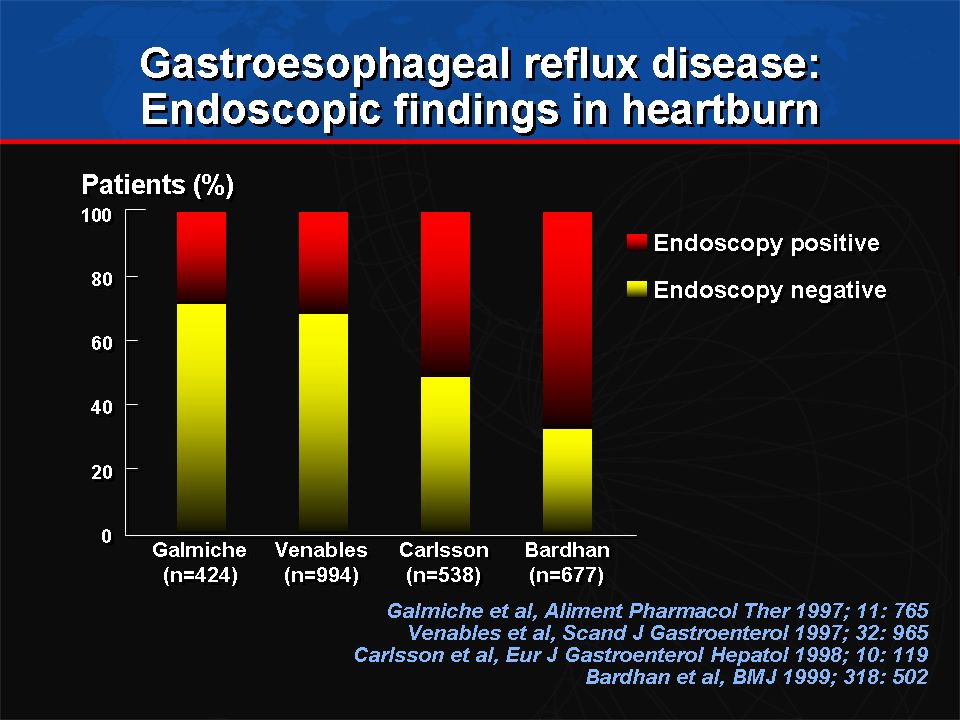
Comment définir le RGO en pratique ?
Symptômes (pyrosis, régurgitations,…) Lésions Oesophagite Complications Sténoses, ulcères Endobrachyoesophage (Barrett’s esophagus, cancer)
 Lésions. Oesophagite. Complications. Sténoses, ulcères. Endobrachyoesophage (Barrett’s esophagus, cancer)")
4
Vers une meilleure définition du RGO
Dent et al Gut 2005; 54: 710-7

5
“ GERD is a condition which develops when the reflux of stomach content causes troublesome symptoms and / or complications” Esophageal Syndromes Extra-esophageal Syndromes Symptomatic Syndromes Syndromes with Esophageal Injury Established Association Proposed Association Typical reflux syndrome Reflux chest pain syndrome Reflux esophagitis Reflux stricture Barrett's esophagus Adenocarcinoma Reflux cough Reflux laryngitis Reflux asthma Reflux dental erosions Sinusitis Pulmonary fibrosis Pharyngitis Recurrent otitis media Vakil et al Am J Gastroenterol (2006)
")
6
La prévalence du RGO dans le monde
Dent et al Gut 2005; 54: 710-7

7
Changing rates of esophageal diseases and H
Changing rates of esophageal diseases and H. pylori incidence in developed countries during the 20th Century There is some evidence that Helicobacter pylori infection protects from GERD, as demonstrated by a lower risk of developing erosions in GERD patients with H. pylori infection,1 and a negative association between H. pylori and the complications of GERD.2 The prevalence of H. pylori has been shown in 20 observational studies to be lower among people with GERD than among people without GERD (38.2% vs 49.5%; OR 0.60).3 In addition, the incidence of GERD and related complications, such as Barrett’s esophagus and adenocarcinoma, has been increasing rapidly since the 1930s, which may be a consequence of decreasing H. pylori prevalence.4 A growing body of evidence suggests that H. pylori is protective against these diseases, for example:2–4 GERD is uncommon in countries in which most adults are colonized by H. pylori (especially cag+ strains) GERD incidence is increasing in Western countries as the prevalence of H. pylori is decreasing The prevalence of H. pylori is lower in people with GERD than in controls. In contrast, there has been a marked decrease in the incidence of most noncardiac gastric adenocarcinoma, which is due at least in part to the decreased prevalence of H. pylori.4 References 1 Labenz J et al. Am J Gastroenterol 2004; 99: 1652–6 2 Delaney B and McColl K Aliment Pharmacol Ther 2005; 22 (Suppl 1):32–40 3 Ragunath A et al. BMJ 2003; 326: 737 4 Blaser MJ. J Infect Dis 1999; 179: 1523–30 Blaser MJ. J Infect Dis 1999; 179: 1523–30
.3 In addition, the incidence of GERD and related complications, such as Barrett’s esophagus and adenocarcinoma, has been increasing rapidly since the 1930s, which may be a consequence of decreasing H. pylori prevalence.4. A growing body of evidence suggests that H. pylori is protective against these diseases, for example:2–4. GERD is uncommon in countries in which most adults are colonized by H. pylori (especially cag+ strains) GERD incidence is increasing in Western countries as the prevalence of H. pylori is decreasing. The prevalence of H. pylori is lower in people with GERD than in controls. In contrast, there has been a marked decrease in the incidence of most noncardiac gastric adenocarcinoma, which is due at least in part to the decreased prevalence of H. pylori.4. References. 1 Labenz J et al. Am J Gastroenterol 2004; 99: 1652–6. 2 Delaney B and McColl K Aliment Pharmacol Ther 2005; 22 (Suppl 1):32–40. 3 Ragunath A et al. BMJ 2003; 326: Blaser MJ. J Infect Dis 1999; 179: 1523–30. Blaser MJ. J Infect Dis 1999; 179: 1523–30.")
8
Influence de l’âge : moins de symptômes et plus de complications
Severe heartburn Sténoses Severe esophagitis Johnson and Fennerty Gastroenterology (2004) Ben Rejeb et al Dig Dis Sci 1992
 Ben Rejeb et al Dig Dis Sci")
9
Risk of reflux symptoms increases across the whole BMI range
Jacobson et al N Eng l J Med (2006)
")
10
Association between overweight or obesity and erosive esophagitis
Hampel et al Ann Intern Med (2005)
")
11
Association of overweight and obesity with esophageal adenocarcinoma
Overweight Obese Hampel et al Ann Intern Med (2005)
")
12
La part de la génétique dans le RGO Les registres de jumeaux
Mohammed et al Gut 2003; 52:

13
Facteurs associés au RGO
conséquence Cause RGO Genetic Demographic Behavioural Comorbidities Dent et al Gut 2005; 54: 710-7

14
Histoire naturelle

15
Trois phénotypes distincts avec des complications spécifiques ?

16
La cohorte ProGERD Une seule maladie lentement progressive
NERD A et B Labenz et al. Am J Gastroenterol 2006; 101: 1477–88

17
En résumé Maladie fréquente, d’incidence croissante
Le plus souvent limitée à des symptômes sans lésions endoscopiques mais dont l’impact sur la qualité de vie est majeur Probablement multifactorielle associant facteurs environnementaux (notamment obésité) et génétiques Maladie chronique, lentement progressive avec de très nombreux phénotypes
 et génétiques. Maladie chronique, lentement progressive avec de très nombreux phénotypes.")
18
Physiopathologie du RGO
Diminution de l’efficacité des contractions de l’œsophage ou de ses défenses naturelles Altération de la barrière anti-reflux HCl Reflux de bile Vidange gastrique lente

19
Préhistoire (i.e. avant 1970)
« Hiatal hernia is the key factor that predisposes to the disease (secondary reflux)…. » « Surgical repair of hiatal hernia is a logical manoeuver... »
…. » « Surgical repair of hiatal hernia is a logical manoeuver... »")
20
Physiologie versus anatomie Le sphincter inférieur de l’œsophage ou la hernie hiatale ?
Cohen and Harris N Eng J Med 1971

21
Les relaxations transitoires du SIO
La découverte majeure des 30 dernières années! Les relaxations transitoires du SIO TLESR Dent et al J Clin Invest (1981)
")
22
Relaxations transitoires du SIO
15 20 25 30 35 40 45 50 24 s 10 s Basal LES pressure = 28 mmHg 4-s IRP= 6.3 mmHg 150 Pressure isocontour 50 -15 mmHg 14 100 Location from the nostril (cm) 22
 22.")
23
Les relaxations transitoires du SIO (TLESRs) représentent
le principal mécanisme responsable du reflux Swallow- LES pressure Absent basal TLESRs induced LES drift LOS pressure relaxation pH Pharynx LOS Stomach 100 80 % Reflux 60 episodes 40 20 Penagini et al., 1996

24
De 1990 à nos jours…. Hernie hiatale : Le retour!
Données épidémiologiques : Significativement associée au RGO « Facilite » les relaxations transitoires du SIO et perturbe le rôle de sphincter externe du pilier droit du diaphragme Facteur de gravité (troubles de la clairance et oesophagite plus fréquente) r
 r.")
25
Un agresseur, l’acide, est responsable des symptômes et des lésions muqueuses
Gastro-Esophageal Reflux PPI Acid, pepsin, bile Caustic-Chemical mucosal injury Basal cell proliferation Papillary cell hyperplasia Mucosal breaks esophagitis

26
Un agresseur, l’acide, est responsable des symptômes et des lésions muqueuses
Gastro-Esophageal Reflux PPI Acid, pepsin, bile 20 à 30 % des malades répondent mal au traitement IPP Les symptômes sont plus résistants que les lésions d’oesophagite Caustic-Chemical mucosal injury Basal cell proliferation Papillary cell hyperplasia Mucosal breaks esophagitis

27
La pHmétrie évalue l’exposition acide (EA) et la relation symptôme/reflux (IS)
cough cough

28
Résultats de la pH métrie de 24h chez des patients ayant
EA + IS + Résultats de la pH métrie de 24h chez des patients ayant un pyrosis sans lésions endoscopiques EA – IS + EA – IS -

29
Normal Esophageal Acid exposure time Functional Heartburn Galmiche et al Gastroenterology (2006)
")
30
Facteurs psychologiques et viscéroperception
Les traits psychologiques anormaux sont plus fréquents chez les patients sans oesophagite1 Le stress, les troubles du sommeil peuvent modifier la viscéroperception 3 Anomalies d’intégration des signaux oesophagiens nociceptifs au niveau cérébral 1 1 Drossman, Aliment Pharmacol Ther 1997; II (suppl. 2): 57 2 Avidan et al, Aliment Pharmacol Ther 2001; 15: 1907 3 Bradley et al, Am J Gastroenterol 1993; 88: 11
: Avidan et al, Aliment Pharmacol Ther 2001; 15: Bradley et al, Am J Gastroenterol 1993; 88: 11.")
31
L’hypersensibilité viscérale dans le RGO
Intestin irritable dyspepsie Efficacité IPP Knowles and Aziz, Gut 2008

32
Des outils nouveaux pourquoi faire?
Faire le diagnostic de RGO dans les formes atypiques sans oesophagite Etablir la responsabilité du RGO dans la pathogénie des symptômes (corrélation symptôme/reflux)
")
33
La prolongation de la durée de l’enregistrement améliore la
performance diagnostique Prakash et al 2005

34
Impédance-métrie : principe
Bolus gazeux Impédance élevée Bolus liquide Impédance basse Impédance = Conductivité 1

35
La pH-impédancemétrie est plus sensible que la pH-métrie
sw sw Impedance 1 sw sw 3 k Impedance 2 3 k Impedance 3 3 k Impedance 4 3 k 7 pH esophagus 4 1 10s 10s 10s Acid reflux Weakly acidic reflux Weakly alkaline reflux Toux

36
Quand et comment faire une pH-impédancemétrie ?
Echec des IPP double dose 2 mois Echec de l’optimisation du traitement RGO jamais démontré Endoscopie pH métrie sans traitement ± impedance ou capsule Bravo RGO préalablement démontré pH-impedancemétrie sous IPP Analyse concordance symptomatique (SI/SAP) Oesophagite Pyrosis Fonctionnel Œsophage acido-sensible NERD Positive Negative
 Oesophagite. Pyrosis. Fonctionnel. Œsophage acido-sensible. NERD. Positive. Negative.")
37
Les objectifs du traitement du RGO en 2012
Soulager les symptômes Cicatriser les lésions, prévenir et, le cas échéant, traiter les complications Prévenir les rechutes

38
La satisfaction des patients est meilleure avec les IPP !
US survey of 11,604 individuals using prescription medication to treat chronic heartburn (PPIs:4109; H2Ras:3782¨;Prokinetics: 3782) Bytzer P. Clin Gastroenterol Hepatol (2009) adapted from Crawley et al J Clin outcomes manage (2000)
 Bytzer P. Clin Gastroenterol Hepatol (2009) adapted from Crawley et al J Clin outcomes manage (2000)")
39
Symptomatic Response to PPI is poorer in NERD Patients
Pooled symptomatic response rate at 4 weeks (%) 9 6 37 56* *p< compared to patients with endoscopic negative reflux disease Tack and Fass. Aliment Pharmacol Ther 2004;19(Suppl. 1):28-34
 * *p< compared to patients with endoscopic negative reflux disease. Tack and Fass. Aliment Pharmacol Ther 2004;19(Suppl. 1):")
40
Existe-t-il des facteurs associées à la non réponse aux IPP ?
100 malades avec symptômes typiques Réponse < 2j/sem symptômes légers sous IPP double dose pH impédancemétrie sans traitement Absence d’oesophagite (p=0.05) BMI < 25kg/m2 (p=0.002) Dyspepsie (p=0.001) Syndrome intestin irritable (P=0.012) Pas de profil pH/ impédancemétrique associé à la non réponse aux IPP Zerbib et al Gut (2011)
 BMI < 25kg/m2 (p=0.002) Dyspepsie (p=0.001) Syndrome intestin irritable (P=0.012) Pas de profil pH/ impédancemétrique associé à la non réponse aux IPP. Zerbib et al Gut (2011)")
41
Limites des IPP Les IPP n’éliminent pas le RGO …ils modifient seulement l’acidité du reflux Il y a matière à amélioration RGO sans oesophagite Symptômes nocturnes Manifestations extra-esophagiennes….

42
The efficacy of PPIs for laryngeal symptoms attributed to GERD: a meta-analysis
Gatta et al Aliment Pharmacol Ther 2007; 25:385-92

43
Treatment with PPI does not Improve Asthma Control
Parallel-group, double-blind controlled trial of esomeprazole 40 mg bid vs placebo (for 24 weeks) in patients with inadequately controlled asthma 412 patients with minimal or no GERD symptoms 40% of participants with abnormal esophageal acid exposure at pH-metry (silent GERD) NO effect of PPI on primary (rate of episodes of poor asthma control) and secondary outcome measures Abnormal pH result did not identify responders to PPI N Engl J Med 2009;369:
 in patients with inadequately controlled asthma. 412 patients with minimal or no GERD symptoms. 40% of participants with abnormal esophageal acid exposure at pH-metry (silent GERD) NO effect of PPI on primary (rate of episodes of poor asthma control) and secondary outcome measures. Abnormal pH result did not identify responders to PPI. N Engl J Med 2009;369:")
44
La Fundoplication par voie Laparoscopique est devenue un standard

45
Schéma général étude LOTUS
Etude ouverte en groupes parallèles, multicentrique, randomisée, conduite dans 11 pays en Europe Traitement Médical Esoméprazole 20 mg qd a Esoméprazole 40 mg qd R Chirurgie b Temps chirurgie -3 mois Baseline 3 ans 5 ans During the 3-mo run-in period all patients received treatment with esomeprazole 40 mg qd to verify symptomatic response and facilitate healing of LA grade C or D esophagitis to grade B or less. At randomization, all patients had to be eligible for LARS with esophagitis of no more than LA grade B and GERD symptoms no more than mild. In the medical treatment arm, patients commenced treatment with esomeprazole 20 mg qd but could be dose-adjusted to 40 mg qd if symptoms were not controlled at 8 weeks, and then to 20 mg bid for a further 8 weeks. LARS was performed according to a standardized procedure, as outlined by Attwood et al. (Standardization of Surgical Technique in Antireflux Surgery: The LOTUS Trial Experience.World J Surgery 2008;32: ). Clinic visits take place on a 6-mo basis during 10 years’ follow-up, surgery patients also having attended a 1-mo postoperative visit. This presentation focuses on the 3-y interim results. a Dose susceptible d’étre augmentée en cas de contrôle incomplet des symptômes par paliers de 20 à 40 mg une fois puis à 20 mg deux fois par jour b Réalisée suivant un protocole standardisé par un opérateur entrainé, et comprenant une fundoplicature complète (Nissen) avec réparation diaphragmatique 45 = randomization 45
. Clinic visits take place on a 6-mo basis during 10 years’ follow-up, surgery patients also having attended a 1-mo postoperative visit. This presentation focuses on the 3-y interim results. a Dose susceptible d’étre augmentée en cas de contrôle incomplet des symptômes par paliers de 20 à 40 mg une fois puis à 20 mg deux fois par jour. b Réalisée suivant un protocole standardisé par un opérateur entrainé, et comprenant une fundoplicature complète (Nissen) avec réparation diaphragmatique. 45. = randomization. 45.")
46
Années après randomisation
Courbes actuarielles de maintien en rémission- Analyse en Intention traitement n=554 Proportion en rémission 80 90 100 92% 85% 70 60 50 40 Esoméprazole 30 Chirurgie 20 p=0.047 (log-rank test) 10 1 2 3 4 5 Années après randomisation Galmiche et al JAMA 2011
 Années après randomisation. Galmiche et al JAMA")
47
Prévalence et séverité des Régurgitations
Proportion de patients % 20 40 60 80 100 -3m 6m 1yr 2yr 3yr 4yr 5yr Chirurgie Esoméprazole Léger Modéré Sévère SH-NEG-0003-C5004

48
LOTUS versus SOPRAN Des progrès évidents à 10 ans d’intervalle!
Esomeprazole (LOTUS) Omeprazole (SOPRAN) LARS (LOTUS) Anti-reflux surgery (SOPRAN) Medical comparison Surgical comparison
 Omeprazole (SOPRAN) LARS (LOTUS) Anti-reflux surgery (SOPRAN) Medical comparison. Surgical comparison.")
49
Comment faire mieux ? Mieux comprendre la physiopathologie du RGO et le mécanisme des échecs thérapeutiques « think out of the box » Développer de nouvelles approches thérapeutiques Médicaments Endoscopie thérapeutique

50
Esophageal mucosal inflammation
Gastro-Esophageal Reflux Acid, pepsin, bile Caustic-Chemical mucosal injury Le modèle caustique implique que les lésions démarrent en surface et progressent ensuite vers la sous-muqueuse Basal cell proliferation Papillary cell hyperplasia Mucosal breaks esophagitis

51
Reflux might cause esophagitis through a cytokine-mediated mechanism rather than caustic acid injury
Distal esophagus 3 days after esophagoduodenostomy Souza et al Gastroenterology, 2009

52
Time course and distribution of IL-8 expression in the distal esophagus
Souza et al Gastroenterology, 2009

53
Effects of colonic fermentation on TLESRs in GERD patients
Test meal with fructo-oligosaccharides TLESRs (mean) * p < 0.01 Placebo 6 5 4 FOS 3 2 1 1h h h h h Piche et al Gastroenterology (2003)
 * p < Placebo FOS h 2h 3h 4h 5h. Piche et al Gastroenterology (2003)")
54
Host phenotype and microbioma types in the distal esophagus
Type 1 Streptococcus genus Type 2 Gram- anaerobes/microaerophiles Normal Esophagus Esophagitis Barrett Esophagus Esophagus inflammation and intestinal metaplasia (BE) are associated with global alteration of the microbioma Yang, Gastroenterology 2009
 are associated with global alteration of the microbioma. Yang, Gastroenterology")
55
Comment inhiber les relaxations
transitoires du SIO? 5-HT3 antagonist GABAB agonist mGLUR5 antagonist (mGLUR8 agonist) GABAB agonist - Fundic mechanoreceptors Vagal afferent - CNS - CCK1 antagonist - NO + + - - Vagal efferent Inhibitory Motor Neuron Interneuron - - Atropine L-NMMA Cannabinoid agonist Morphine
 GABAB agonist. - Fundic mechanoreceptors. Vagal afferent. - CNS. - CCK1 antagonist. - NO Vagal efferent. Inhibitory. Motor Neuron. Interneuron. - - Atropine. L-NMMA. Cannabinoid agonist. Morphine.")
56
GABAB Agonists: Arbaclofen Placarbil
A prodrug of the R-isomer of baclofen Decreases total number of reflux events (Gerson 2010) No significant effect on symptoms as monotherapy (Vakil 2011) Development stopped
 No significant effect on symptoms as monotherapy (Vakil 2011) Development stopped.")
57
GABAB Agonists: Lesogaberan
Reduced TLESR and reflux occurrence (Boeckxstaens 2010) Significant reduction of symptoms (Add-on) (Boeckxstaens 2011) Development stopped
 Significant reduction of symptoms (Add-on) (Boeckxstaens 2011) Development stopped.")
58
mGluR5 antagonists: ADX10059
Reduction of acid/weakly acidic reflux events in healthy subjects and GERD patients (Keywood 2009, Zerbib 2010) Significant reduction of symptoms (monotherapy) (Zerbib 2011) Development stopped Symptoms Reflux
 Significant reduction of symptoms (monotherapy) (Zerbib 2011) Development stopped. Symptoms. Reflux.")
59
Traitements endoscopiques : ne jetez pas le bébé avec l’eau du bain!
A Radiofrequency B Endoscopic suturing C Injection at the LOS 1RCT (+) Withdrawn safety implantation 3 RCT (+) PHRC ? D Prosthesis insertion 2 RCT (+) EndoCinch withdrawn Esophyx ? 10 1 RCT (-) Withdrawn
 Withdrawn. safety. implantation. 3 RCT (+) PHRC D Prosthesis insertion. 2 RCT (+) EndoCinch. withdrawn. Esophyx RCT (-) Withdrawn.")
Présentations similaires