Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Antoine Roch Réanimation Médicale Marseille
Complications respiratoires post-opératoires: physiopathologie et prise en charge Antoine Roch Réanimation Médicale Marseille

2
Epidémiologie et facteurs prédictifs

4
Facteurs pré-operatoires Toutes chirurgies confondues
% 40 30 Complications Complications - 20 10 Tabac ASA>II Age > 70 Obésité BPCO Smetana. NEJM 99

5
Type de chirurgie

6
28 facteurs de risque identifiés !!!
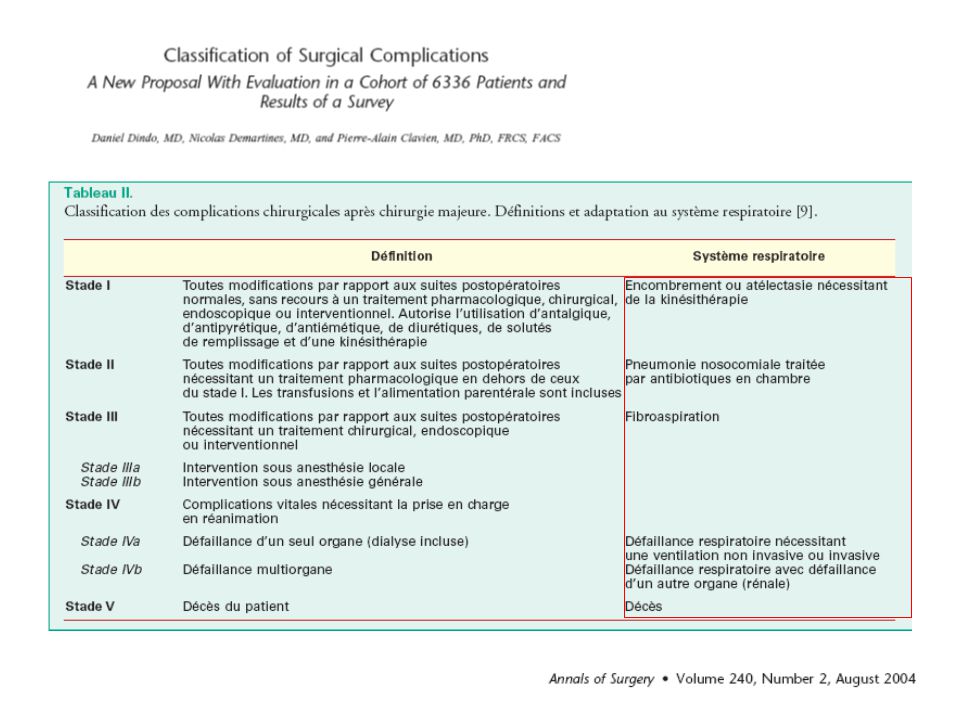
Mortalité J30 = 26.5% si défaillance respiratoire postop (vs 1.4%) 3 points ou plus : ASA > 2 Complexité chir Chir de la bouche Chir du système respiratoire The 30-day mortality of 26.5% among those with RF versus 1.4% among patients without RF illustrates the gravity of the RF as a postoperative complication (Table 3). Of the 17 complications tracked, each one had a higher incidence of RF. The 3 complications with the largest percentage difference between the RF and non-RF patients were pneumonia (35.4% versus 1.2%), systemic sepsis (23.2% versus 0.9%), and cardiac arrest (13.3% versus 0.3%).
 3 points ou plus : ASA > 2. Complexité chir. Chir de la bouche. Chir du système respiratoire. The 30-day mortality of 26.5% among those with RF. versus 1.4% among patients without RF illustrates the. gravity of the RF as a postoperative complication (Table. 3). Of the 17 complications tracked, each one had a. higher incidence of RF. The 3 complications with the. largest percentage difference between the RF and. non-RF patients were pneumonia (35.4% versus 1.2%), systemic sepsis (23.2% versus 0.9%), and cardiac arrest. (13.3% versus 0.3%).")
7
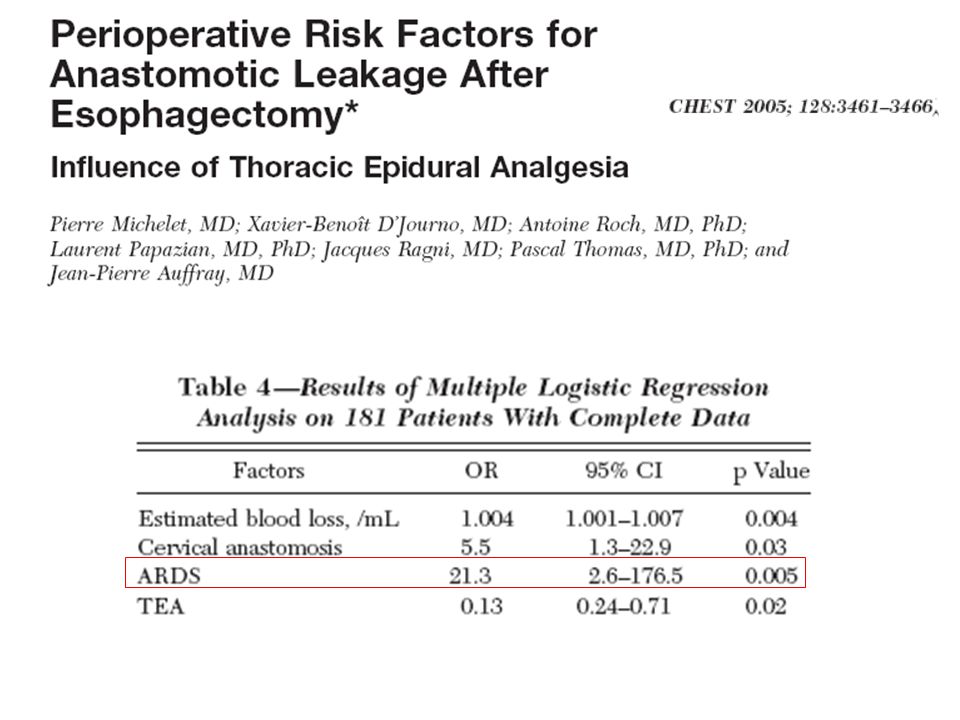
Facteurs de risque de SDRA après oesophagectomie: facteurs per-opératoires !!
Tandon S. et al Br J Anaesth 2001; 86:633-8 Toujours penser à une complication chirurgicale !!!! 7

9
Influence à long terme des CRPO
Kinugasa S et coll. J Surg Onco 2004;88:71-74

10
Physiopathologie

11
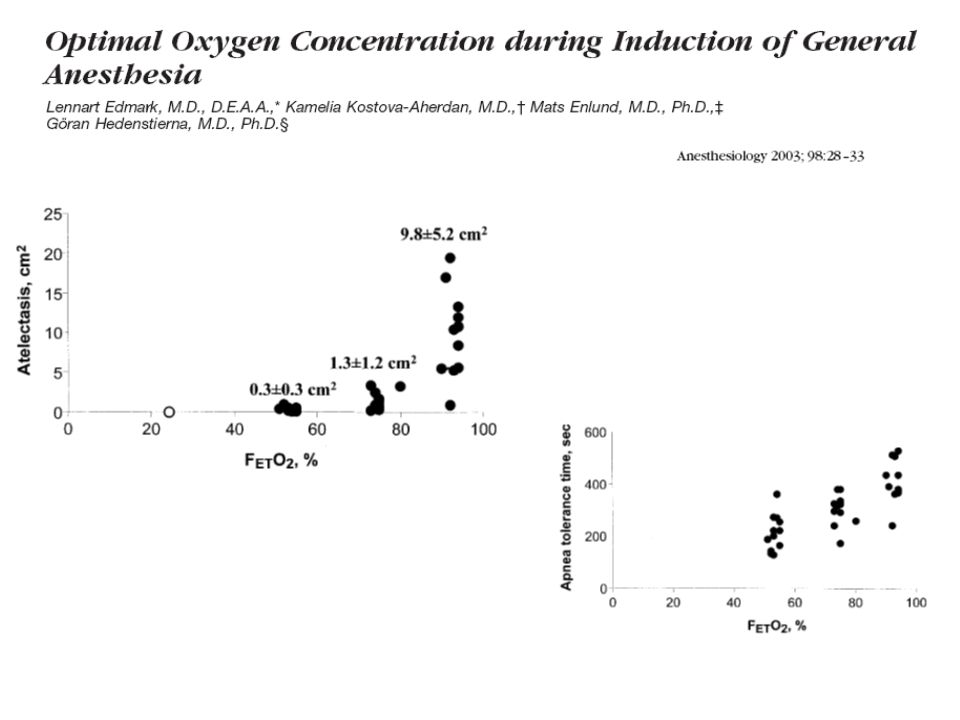
Perte du tonus diaphragmatique Hauts niveaux de FIO2
ANESTHESIE Perte du tonus diaphragmatique Hauts niveaux de FIO2 Ventilation mécanique CHIRURGIE Manipulations des viscères ↑° des pressions trans-murales Réaction inflammatoire COLLAPSUS ALVEOLAIRE Iléus réflexe Douleur DYSFONCTION DIAPHRAGMATIQUE HYPOVENTILATION ALVEOLAIRE ATELECTASIE Infection Hypoxémie SDRA 11

12
Effets sur les volumes pulmonaires
Pendant l’anesthésie Dysfonction diaphragmatique postopératoire

13
Dépression diaphragmatique Augmentation tonus muscles abdominaux
Syndrome restrictif: Dépression diaphragmatique Augmentation tonus muscles abdominaux Tous les anesthesiques, sauf la ketamine, diminuent la CRF, induisant un syndrome restrictif Individu - dépendant

14
Dysfonction diaphragmatique
postopératoire Curarisation résiduelle Douleur Réflexe inhibiteur

15
après chirurgie abdominale
Volumes pulmonaires après chirurgie abdominale 2 4 6 8 10 12 100 80 60 40 % valeur contrôle sus-mésocolique sous-mésocolique capacité vitale jours CRF Diminutuin frc entraine heterogeneite rapports Va/Q et contribue à la formation d’atelectasies Ford et al. ARRD 1983

16
Atélectasies Causes : compression des alvéoles par déplacement céphalique du diaphragme réabsorption des gaz Très fréquente Collapsus alvéolaire réversible

17
Après quelques minutes
Atelectasie = Après quelques minutes 17

18
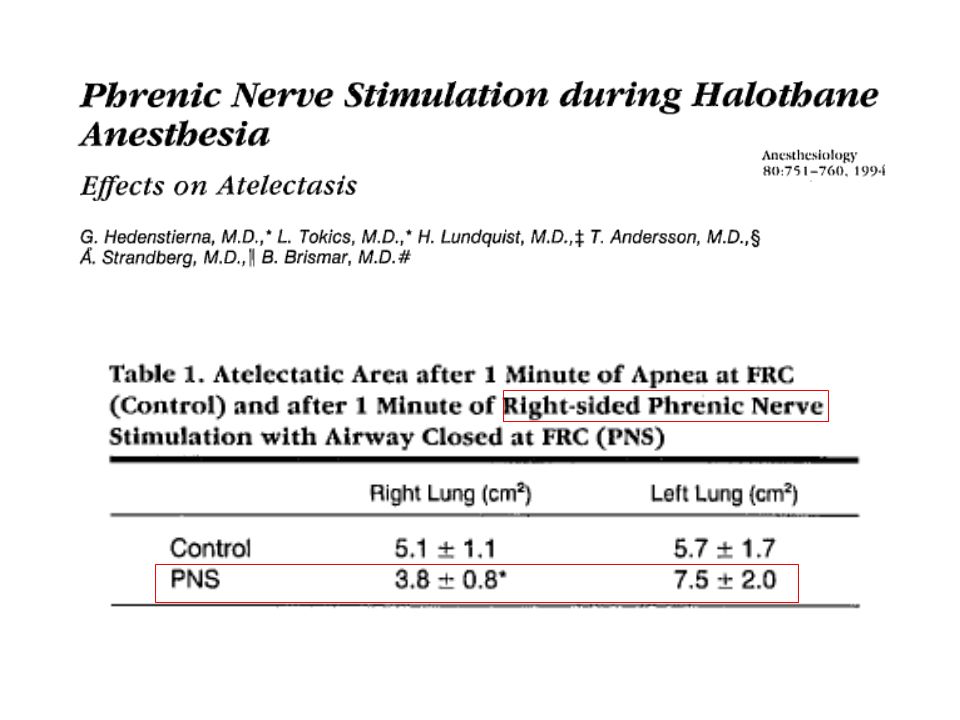
Rôle de l’anesthésie et des curares
6 h de ventilation chez des porcs Roch, Fouche SRLF 2009

20
En chirurgie abdominale
PIA Réduction du volume pulmonaire ventilable Compliance réduite

22
Atélectasies Conséquences : baisse compliance
anomalies échanges gazeux augmentation RVP VILI Pneumonies

23
Paramètres ventilatoires
ARNm de cytokines dans LBA Paramètres ventilatoires Cytokines dans LBA Aspect macroscopique Evalue l’effet de la contraction diaph sans modif de vent minute ou de vt, donc pas de vol assisté delivré si trigger 8 avec curares, 8 sans Table: vt et vm identiques, cycle debutant par une prssion neg dans non curares, et pcrete plus élevée avec compliance plus basse

24
Atélectasie Fuite capillaire Dysfonction cardiaque Dte Oxygénation
Rats poumons sains avec manœuvre recrutement et pep pendant 2.5h Fuite capillaire Atélectasie Oxygénation Dysfonction cardiaque Dte Rats avec manœuvre recrutement et pep pendant 2.5h

25
GBS = streptocoque B

26
Prévention des complications

27
interventions spécifiques sur la réduction du risque respiratoire
Stratégie de réduction Niveau de preuve Type de complications Réexpansion pulmonaire post-op A Atélectasie, pneumonie, bronchite, hypoxémie Décompression gastrique sélective B Atélectasie,pneumonie, inhalation Curares d’action courte Atélectasie, pneumonie Laparoscopie C Atélectasie, pneumonie, toutes complications Arrêt du tabac I Ventilation postopératoire AG-APD combinées Atélectasie, pneumonie IRA Péridurale analgésique A: bon niveau de preuve B: assez bonne évidence C: tendance à ne pas être un facteur de risque I: données insuffisantes pour conclure Lawrence VA Ann Intern Med 2006 27

28
Prise en charge Stratégies pré-operatoires : kinésithérapie, nutrition
Stratégies per-opératoires : ventilation antibioprophylaxie-thérapie Stratégies post-opératoires : kinésithérapie Analgésie CPAP-VNI

29
Ventilation per-opératoire

30
Atelectasie = 30

31
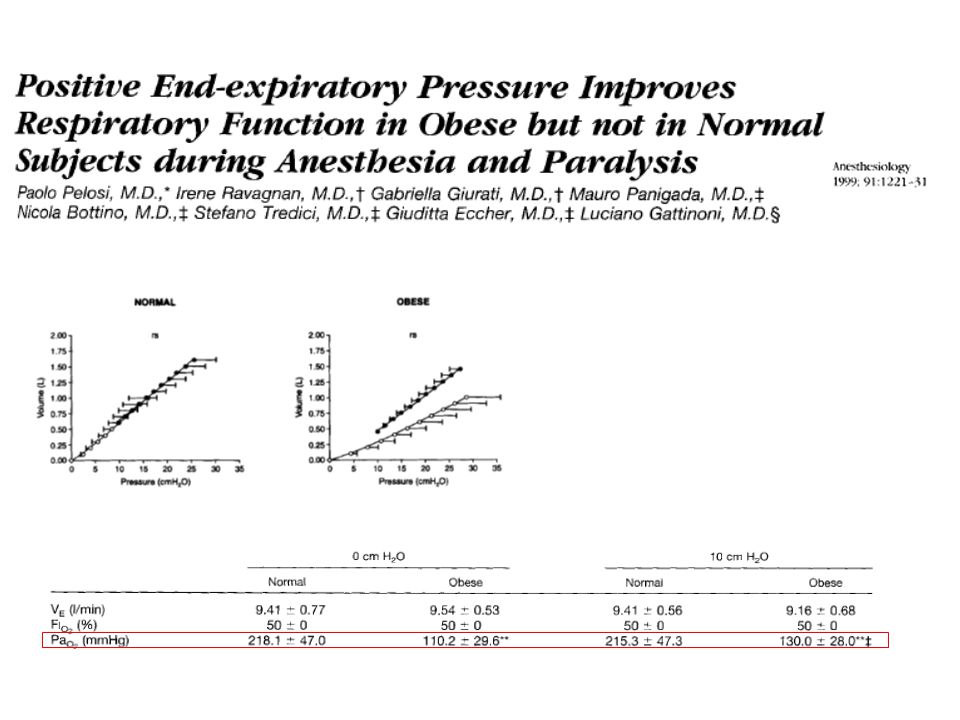
L’application d’une PEEP prévient la survenue d’atélectasie
Positive end-expiratory pressure prevents atelectasis during general anaesthesia even in the presence of a high inspired oxygen concentration Neumann, Rothen, Berglund, Valtysson, Magnusson, Hedenstierna Acta Anaesthesiol Scand 1999; 43: 295–301 Aw awake Ab 15 min après induction Vcm fin de manœuvre en CV L’application d’une PEEP prévient la survenue d’atélectasie durant l’anesthésie générale mais manœuvre de recrutement seule insuffisante 31

33
Étude sur les détresses Respiratoires postopératoires
(80 % de la mortalité) Le volume courant Facteur indépendant de RF 8,3 vs 6,7 ml / kg 33
 Le volume courant. Facteur indépendant de RF. 8,3 vs 6,7 ml / kg. 33.")
34
Patients were randomly assigned to a conventional ventilation strategy (n=26, tidal volume of 9ml.kg-1 during two and one-lung ventilations, no positive end-expiratory pressure) or a protective ventilation strategy (n=26, tidal volume of 9 ml.kg-1 during two-lung ventilation reduced to 5 ml.kg-1 during one-lung ventilation, positive end-expiratory pressure 5 cmH2O throughout the operative time 34

35
Facteurs de dysfonction respiratoire postopératoire (œsophage)
Dysfonctions cognitives et troubles du sommeil Inhalation Souffrance anastomotique et réaction inflammatoire Surdistension du poumon non exclu avec troubles des rapports ventilation/perfusion Ventilation mécanique prolongée Atélectasies postopératoires Dysfonction des muscles respiratoires accessoires Ischémie reperfusion, ventilation monopulmonaire prolongée Résection ganglionnaire étendue Dysfonction diaphragmatique Manipulations digestives Incisions chirurgicales abdominale et thoracique 35

36
PEP lors de la Ventilation monopulmonaire
Cohen E J Cardiothorac Vasc Anesth 1996;10: 36

37
37

38
Antibio-prophylaxie et pneumonies ?

39
L’antibioprophylaxie est axée sur les infections de paroi
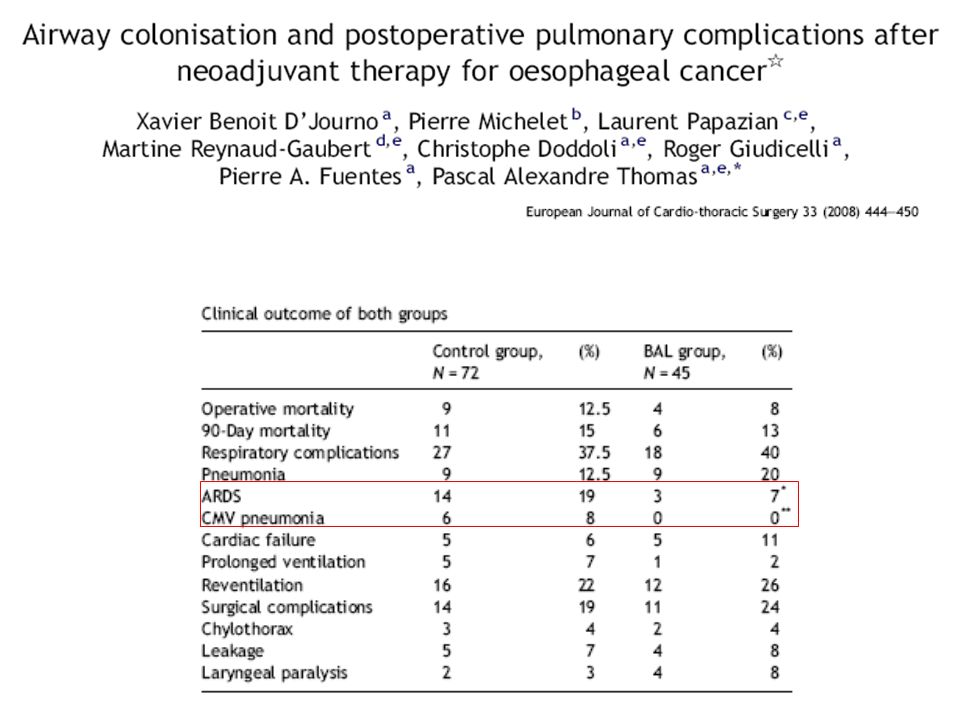
2 périodes : 6 mois C2G, 12 mois Augmentin Baisse de 45 % des pneumopathies dans seconde période Confirmation nécessaire par RCT

40
45 LBA pré-op, 72 contrôles 7 patients traités en pré-op (germes jugés pathogènes):
:")
42
Analgésie

43
Après cholecystectomie ou chez le sujet âgé

44
Après chir cardiaque ou abdominale

45
Population : lobectomie
PCA ± Kétamine PCA Baisse conso morphine

46
915 patients avec comorbidités et chirurgie abdominale

47
Chirurgie Abdominale Majeure

48
Risque de pneumonie post-operatoire
This meta-analysis reviews the impact of epidural versus systemic analgesia during 24 h or longer in the postoperative period of major surgery. Epidural analgesia reduced the need for prolonged mechanical ventilation or reintubation.

49
Diminution du bénéfice dans les études
Risque de pneumonie post-operatoire Diminution du bénéfice dans les études les plus récentes This meta-analysis reviews the impact of epidural versus systemic analgesia during 24 h or longer in the postoperative period of major surgery. Epidural analgesia reduced the need for prolonged mechanical ventilation or reintubation.

50
15 études randomisées // 1179 patients
AG vs AG + APD Thoracique

52
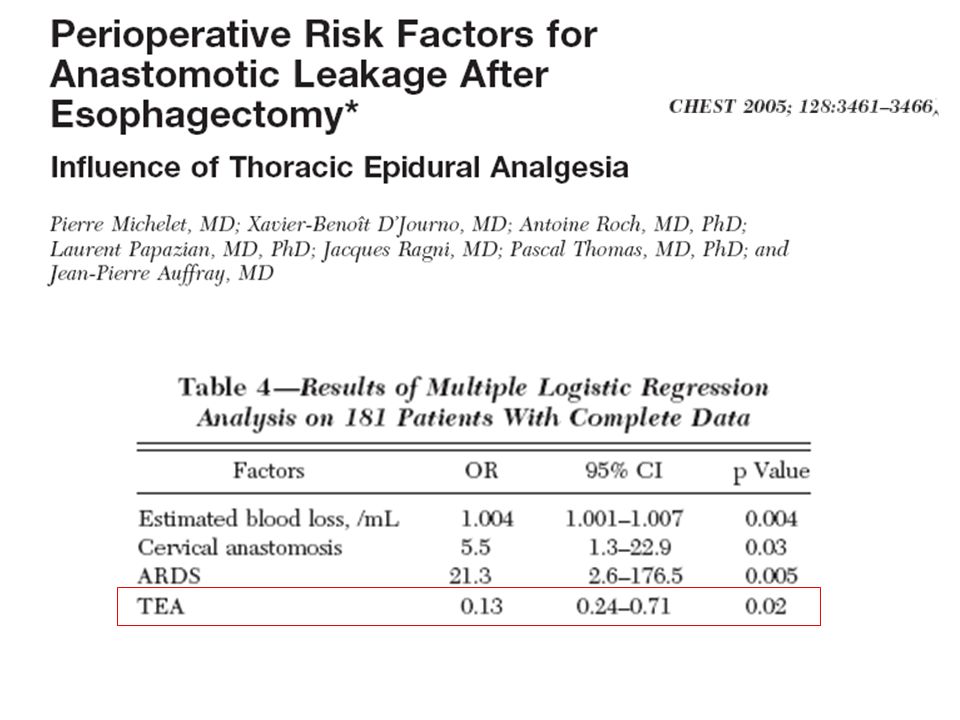
La Péridurale Thoracique
[92] Meilleur respect de la structure du sommeil Promotion de l’extubation précoce [83, 84, 90] Amélioration de la perfusion anastomotique Qualité de l’analgésie au repos et à l’effort Amélioration de la kinésithérapie postopératoire Réduction des atélectasies Réduction des complications respiratoires Amélioration des rapports ventilation / perfusion [85] Amélioration de la cinétique diaphragmatique [87, 91] Amélioration de la fonction digestive

53
Intrications des Facteurs Médicaux et Chirurgicaux
L’Hypoxémie L’Ischémie L’Inflammation 53

54
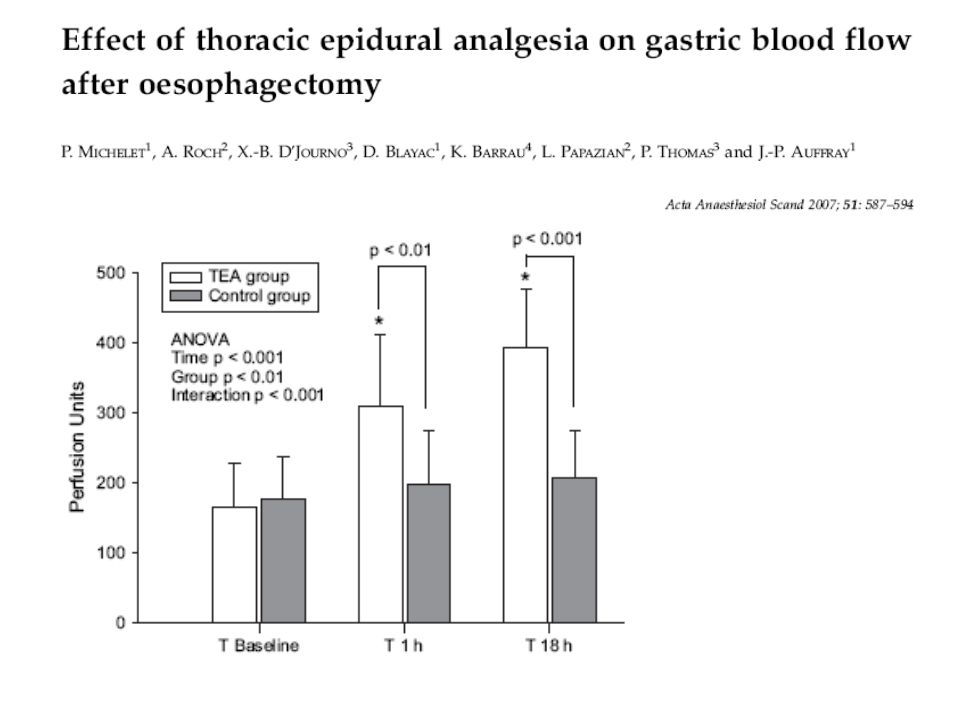
Péridurale Thoracique et Perfusion du transplant gastrique
Étude par laser doppler Évolution de la perfusion Muqueuse avant et après 1 et 18 H De perfusion de péridurale Michelet P. et al Acta Anesthesiologica Scandinavica 2007 54

56
Spiromètre incitative: pas d’évidence en faveur
Cochrane Database Syst Rev Jul 18;3 Incentive spirometry for preventing pulmonary complications after coronary artery bypass graft. Freitas ER, Soares BG, Cardoso JR, Atallah AN.

57
CPAP- VNI Bénéfices attendus
Diminuer le travail respiratoire et compenser la perte respiratoire post-op Améliorer le recrutement alvéolaire et les échanges gazeux (atélectasies) Diminuer la post charge cardiaque nCPAP delivers constant positive airway pressure during both inspiration and expiration, either by use of a flow generator with a high-pressure gas source or by use of a portable compressor. nCPAP exerts its effects by increasing intrathoracic pressure to prevent atelectasis and increasing functional residual capacity; by reducing the work of breathing; by increasing oxygenation and CO2 washout; and by improving the left ventricular afterload and hemodynamics. Different from nCPAP, nPPV allows a better respiratory systemmuscle unloading, alveolar recruitment, oxygenation and CO2 washout, and dyspnea relief.
 Diminuer la post charge cardiaque. nCPAP delivers constant positive airway pressure during. both inspiration and expiration, either by use of a flow. generator with a high-pressure gas source or by use of a. portable compressor. nCPAP exerts its effects by increasing. intrathoracic pressure to prevent atelectasis and. increasing functional residual capacity; by reducing the. work of breathing; by increasing oxygenation and CO2. washout; and by improving the left ventricular afterload. and hemodynamics. Different from nCPAP, nPPV allows a better. respiratory systemmuscle unloading, alveolar recruitment, oxygenation and CO2 washout, and dyspnea relief.")
58
CPAP 10 pendant > 6h / j VS trt standard
Zarbock et al. [34] reported that, in a large prospective randomized study, prophylactic nCPAP of 10cmH2O (study) for at least 6 h per day following surgery in comparison with standard treatment including 10 min of intermittent nCPAP at 10cmH2O every 4 h improved arterial oxygenation, reduced the incidence of pulmonary complications including pneumonia and reintubation rate, and reduced the readmission rate to ICU or an intermediate care unit.
 for at least 6 h per day following. surgery in comparison with standard treatment including. 10 min of intermittent nCPAP at 10cmH2O every 4 h. improved arterial oxygenation, reduced the incidence of. pulmonary complications including pneumonia and reintubation. rate, and reduced the readmission rate to ICU or. an intermediate care unit.")
59
La CPAP en (quasi) préventif ?
Squadrone V et al JAMA 2005 Fréquence d’intubation en postopératoire N=209 Chir abdominale lourde Inclusion si PAFI < 300 dans première h postextub CPAP 7,5 cm H2O pdt au moins 6h vs O2 Patients scheduled for elective abdominal surgery and general anesthesia were eligible to participate in the study if they met the following criteria: abdominal surgery requiring laparotomy and time of viscera exposure longer than 90 minutes. At the end of the surgical procedure, patients were extubated and underwent a 1-hour screening test breathing oxygen through a Venturi mask at an inspiratory fraction of 0.3. Patients were included in the study if they developed an arterial oxygen tension to inspiratory oxygen fraction ratio (PaO2/FiO2) of 300 or less Squadrone et al. [70], in a multicenter RCT, evaluated the effect of CPAP in patients with early hypoxemia after major abdominal surgery. The authors randomized 209 patients who developed an arterial oxygen tension to inspiratory oxygen fraction ( pO2/FiO2) less than 300mmHg to receive oxygen or oxygen along with CPAP of 7.5 cm H2O for at least 6 h continuously. Patients with cardiac or pulmonary comorbidities were excluded from the study. Pneumonia, intubation rate, and sepsis were reduced in the CPAP group, and a trend of shorter ICU length of stay was reported. Three patients died in hospital among the group of patients who received oxygen alone but none in the treatment group. The trial was concluded before the expected sample size was reached due to the clinical benefits particularly in the primary outcome, endotracheal intubation (1 versus 10%, P¼0.005) [70]. This study demonstrates that CPAP should be implemented as an early therapy for at least 6 consecutive hours when the lung is still highly compliant. La CPAP en (quasi) préventif ? 59
 of 300 or less. Squadrone et al. [70], in a multicenter. RCT, evaluated the effect of CPAP in patients. with early hypoxemia after major abdominal surgery. The. authors randomized 209 patients who developed an. arterial oxygen tension to inspiratory oxygen fraction. ( pO2/FiO2) less than 300mmHg to receive oxygen or. oxygen along with CPAP of 7.5 cm H2O for at least 6 h. continuously. Patients with cardiac or pulmonary comorbidities. were excluded from the study. Pneumonia, intubation. rate, and sepsis were reduced in the CPAP group, and a trend of shorter ICU length of stay was reported. Three patients died in hospital among the group of. patients who received oxygen alone but none in the. treatment group. The trial was concluded before the. expected sample size was reached due to the clinical. benefits particularly in the primary outcome, endotracheal. intubation (1 versus 10%, P¼0.005) [70]. This. study demonstrates that CPAP should be implemented. as an early therapy for at least 6 consecutive hours when. the lung is still highly compliant. La CPAP en (quasi) préventif 59.")
60
La CPAP en (quasi) préventif ?
Squadrone V et al JAMA 2005 60

61
Groupe contrôle Groupe VNI p IOT et VM 12 (50%) 5 (20.8%) 0.035 Mortalité hospitalière 9 (37.5%) 3(12.5%) 0.045 Durée de séjour en USI (j) 14+/-11,1 16,65+/-23.6 0.52 Durée d’hospitalisation (j) 22.8+/-10.7 27.1+/-19.5 0.061 Mortalité à 120 jours
 3(12.5%) Durée de séjour en USI (j) 14+/-11,1. 16,65+/ Durée d’hospitalisation (j) 22.8+/ / Mortalité à 120 jours.")
62
Critères assez larges de détresse et hypoxémie
Jaber et al. [15] in an observational study demonstrated the feasibility, good tolerance and safety of nPPV for the treatment of ARF after digestive surgery.More severe initial hypoxemia and lower improvement in PaO2 after treatment were predictive of nPPV failure. FDR d’échec: Hypoxémie plus sévère Amélioration PaO2 plus faible

63
The beneficial effects of CPAP to prevent or treat respiratory
complications in patients undergoing abdominal surgery are well supported. However, although studies on the use of CPAP in postoperative cardiac surgery are promising, there are not enough data to support its application. Further studies are needed to confirm whether CPAP is applicable to a general population of patients during the early postoperative period in order to prevent the high mortality rate due to respiratory complications.

64
113/690 patients = 16% IOT évitée dans 85%
Lefebvre et al. [42] confirmed in an observational prospective survey the feasibility and efficacy of early nPPV in ARF following lung resection. During a 4-year period, among 690 patients at risk of severe complications following lung resection, 16% experienced ARF, which was initially managed by nPPV with a success rate of 85%.

65
Indications en pratique
Dyspnée modérée à sévère FR > 25 Tirage PaO2/FiO2 < 250 PaCO2 > 45, pH < 7.35 Rechercher la cause de la détresse respiratoire !

66
Réglages en pratique CPAP : 7-10 cmH2O VNI :
PEP : 2-5 cmH2O AI: augmentation jusqu’à 20 cmH2O pour obtenir un Vt de 6 à 10 ml/kg et selon confort Durée : min à intervalles de 2-4h Sevrage progressif

67
Conclusions CRPO fréquentes et avec lourde morbi-mortalité
La ventilation per-opératoire influence les CRPO L’APD est utile après chirurgie abdominale lourde et thoracique CPAP préventive : intérêt montré en chir cardiaque CPAP - VNI curative : surtout si précoce études nécessaires pour la généralisation

68
Merci de votre attention

69
This meta-analysis evaluated the benefits of postoperative CPAP for patients
undergoing abdominal surgery. The authors suggest that CPAP decreases the risk of respiratory complications and support its clinical use.

71
CRPO pneumonies atélectasies

Présentations similaires



>")
















