Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Cancer du col utérin et coelioscopie
Emile Daraï, Emmanuel Barranger, Roman Rouzier, Serge Uzan. Service de Gynécologie-Obstétrique Hôpital Tenon , CancerEst, Université Pierre et Marie Curie Paris 6, France First of all, I would like to thank the committee of organization for his invitation to speak on

2
Classification anatomique des cancers du col

3
Classification FIGO

4
Tumeur localisée du col stade Ib1

5
Tumeur du col stade Ib2 4 cm

6
Cancer du col stade Ib2

7
Atteinte vaginale stade IIa

8
Atteinte paramétriale stade IIb

9
Cancer du col stade III urinaire

10
Cancer du col stade IV: atteinte vésicale

11
Moyens thérapeutiques du cancer du col
Chirurgie exclusive. Radiothérapie exclusive. Association radio-chirurgicale. Association radio-chimiothérapie concomitante. A part traitement conservateur: - trachélectomie élargie, - ganglion sentinelle.

12
Indication chirurgicale pour les cancers du col de stade Ib1
Pas de standard: Options: - Chirurgie première; Piver II ou III et lymphadénectomie - Irradiation exclusive: radio et curiethérapie - Association radio-chirurgicale: curiethérapie, ± radiothérapie externe Piver II ou III et lymphadénectomie

13
Indication chirurgicale CancerEst pour les cancers du col de stade Ib1
Désir de grossesse et lésion < 2 cm: trachélectomie élargie (problème des adénocarcinomes) Lésion > 2 cm ou lésion < 2 cm sans désir de grossesse: colpohystérectomie élargie coelioscopie ou Amreich-Schauta
 Lésion > 2 cm ou lésion < 2 cm sans désir de grossesse: colpohystérectomie élargie coelioscopie ou Amreich-Schauta.")
14
Faisabilité de la colpo-hystérectomie élargie pour cancer du col
Since the first laparoscopic radical hysterectomy performed by Canis in 1989, several series have confirmed its feasibility. As for abdominal radical hysterectomy, the main indications are women with Stage IA or IB1 cervical or IIa with small tumour size cancer. However, Hertel and Malur reported for locally advanced cervical cancer a laparoscopic treatment. Although some authors performed laparoscopic radical hysterectomy for locally advanced stages, several prospective trials have underlined the relevance of first concomitant radiochemotherapy.

15
Complications de la colpo-hystérectomie élargie pour cancer du col
As in our experience, Spirtos and Pomel performed an exclusive laparoscopic radical hysterectomy whereas all others authors use a combined laparoscopic and vaginal technique. The mean operating time varied according to series between 205 and 380 minutes. The mean operating time was higher than 300 minutes for our first 20 cases but is now less than 200 minutes including the time for sentinel node procedure. Whatever the series, an acceptable intra-operative complication rate has been reported ranging from 2% to 13%.

16
Complications et survie après colpo-hystérectomie élargie pour cancer du col
The rate of post-operative complications is mainly related to urinary disorders including infection and dysuria. To our knowledge, no death subsequent to laparoscopic radical hysterectomy has been reported.

17
Complications de la colpo-hystérectomie élargie: coelio vs laparotomie
When comparing the morbidity of laparoscopic radical hysterectomy with those from the metaanalysis performed by Magrina including seven studies of abdominal radical hysterectomy, no difference in post-operative complications were found between the two routes. In our experience of 52 operations, 3 ureteral stenosis and 1 urinary fistula occurred but always in women with locally advanced stages carcer treated by first concomitant radiochemotherapy followed by Piver II operation. Hertel et al, Gynecol Oncol 2003

18
Survie globale de la colpo-hystérectomie élargie pour cancer du col
On a large series including 200 women, Hertel reported an overall survival rate about 80%. Hertel et al, Gynecol Oncol 2003

19
Survie après colpo-hystérectomie élargie pour cancer du col de stade Ia ou Ib1
For women with stage Ia or Ib1 cervical cancer, the overall survival reached 97%. Hertel et al, Gynecol Oncol 2003

20
Survie sans récidive après colpo-hystérectomie élargie pour cancer du col en fonction de l’envahissement lympho-vasculaire In addition to tumour stage, Lymphovascular space involvement appeared a major prognostic factor of survival. Disease-free survival was 35%for women with both lymphatic and vascular involvement and 85% for women without lymphovascular involvement. Hertel et al, Gynecol Oncol 2003

21
Survie sans récidive après colpo-hystérectomie élargie en fonction du statut ganglionnaire
After exclusion of women with no lymph node involvement, Hertel et al found a relation between the number of positive lymph nodes and survival. Hertel et al, Gynecol Oncol 2003

22
Colpo-hystérectomie élargie pour cancer du col: coelio vs laparotomie
Recently, in a case control study, Nam demonstrated that abdominal and laparoscopic radical hysterectomy had similar operating time, number of lymph nodes removed, blood loss and transfusion rate but hospital stay was shorter for women treated by laparoscopy. Nam et al Gynecol Oncol 2004

23
Colpo-hystérectomie élargie pour cancer du col: coelio vs laparotomie
Steed in a study comparing 71 women after laparoscopy and 205 women after laparotomy observed a higher operating time and intra-operative complication rate for laparoscopy but a lower blood loss. Steed et al, Gynecol Oncol 2004

24
Colpo-hystérectomie élargie pour cancer du col stade Ia-Ib: coelio vs laparotomie
In contrast, no difference in post-operative complications was found. As in our experience, a higher rate of dysuria was noted after laparoscopic radical hysterectomy. No clear explanation has been suggested. Steed et al, Gynecol Oncol 2004

25
Survie après colpo-hystérectomie élargie pour cancer du col stade Ia-Ib: coelio vs laparotomie
LARVH RAH For women with stage IA or IB, Steed found no difference in overall survival between women operated on by laparoscopy or laparotomy. Steed et al, Gynecol Oncol 2004

26
Survie après colpo-hystérectomie élargie pour cancer du col stade: coelio vs laparotomie
Nam noted that overall survival was poorer after laparoscopy for locally advanced stages of cervical cancer and suggested that laparoscopy should be restricted to early stages disease. Although laparoscopic management appears a safe option, this underlines the need for prospective trial comparing laparoscopy and laparotomy. Nam et al Gynecol Oncol 2004

27
CHE par voie laparoscopique pour cancer du col de stade IB1: Expérience de Tenon
52 patientes (50 ans; ans) opérées entre 2001 et 2006. Durée opératoire: 157 mn ( mn). 45 CHE, 4 Amreich-Schauta, 3 trachélectomies élargies 17% de métastases ganglionnaires. Complications per-opératoires: 7% (plaie vésicale, saignement per-opératoire et plaie des gros vaisseaux avec laparoconversion). Complications post-opératoires immédiates: 9%. Abcès essentiellement.
 opérées entre 2001 et Durée opératoire: 157 mn ( mn). 45 CHE, 4 Amreich-Schauta, 3 trachélectomies élargies. 17% de métastases ganglionnaires. Complications per-opératoires: 7% (plaie vésicale, saignement per-opératoire et plaie des gros vaisseaux avec laparoconversion). Complications post-opératoires immédiates: 9%. Abcès essentiellement.")
28
Etude randomisée comparant la stadification clinique et coelioscopique
Lai et al., Gynecol Oncol 2003

29
Risques de la coelioscopie
Challan-Belval & Daraï, Gynecol Oncol 2006

30
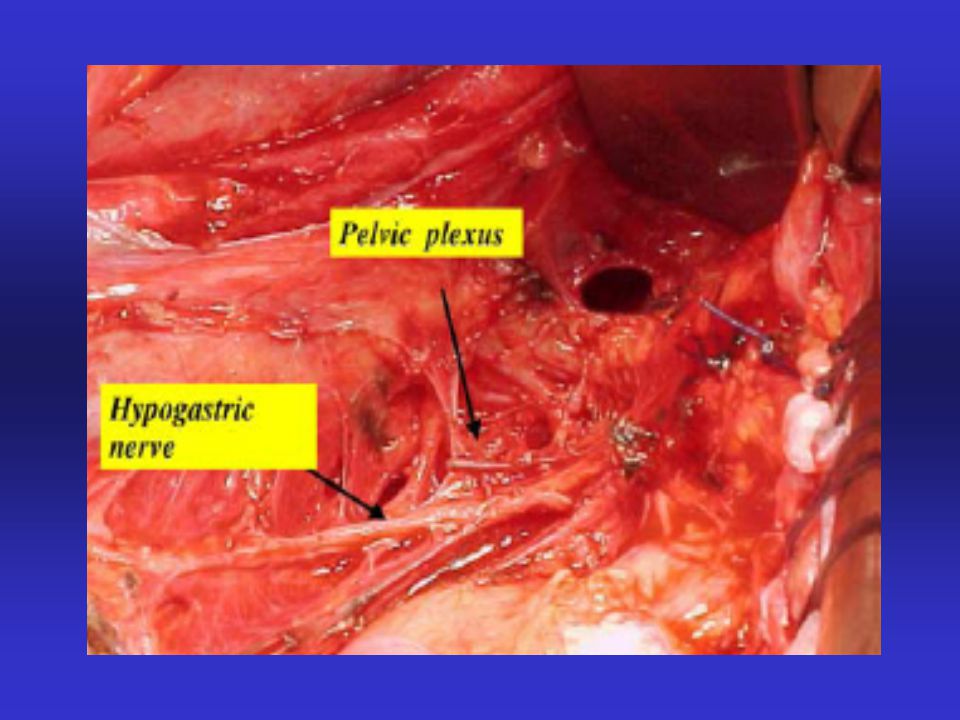
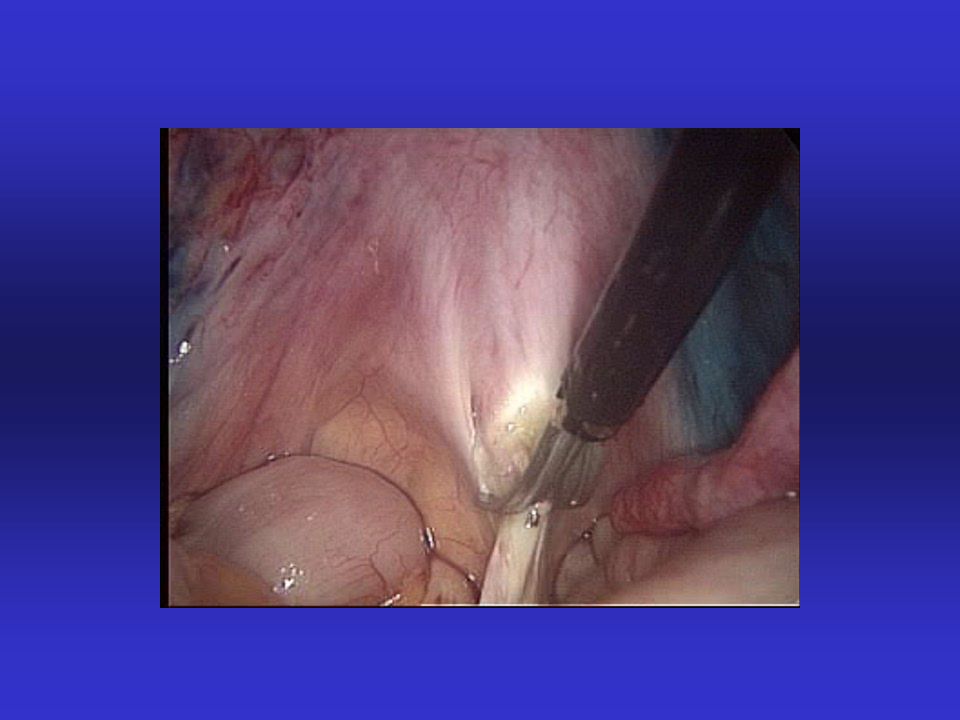
Artifices chirurgicaux pour diminuer la morbidité de la colpohystérectomie
Transposition ovarienne. Préservation du plexus hypogastrique inférieur. Réduire les indications des lymphadénectomies: Procédure du ganglion sentinelle. Clarifier les indications de paramétrectomie.

31
Incidence des métastases ovariennes associées au cancer du col utérin
Shimada et coll, Gynecol Oncol 2006

33
Procédure du ganglion sentinelle
Gil-Moreno et al, Gynecol Oncol, 2005

34
BJOG, 2005

35
Facteurs déterminants de l’envahissement paramétrial
Steed et al, Gynecol Oncol 2006

36
Indication chirurgicale CancerEst pour les cancers du col de stade Ib2 ou II
curage pelvien et lombo-aortique coelioscopique premier et radiochimiothérapie concomittante - chirurgie complémentaire si N(-) - radiochimiothérapie concomittante exclusive si N(+)
 - radiochimiothérapie concomittante exclusive si N(+)")
37
Curage pelvien et lombo-aortique premier pour stade Ib2 ou II: Expérience de Tenon
25 patientes (âge moyen 48 ans) entre 2001 et 2006. Durée opératoire: 204 mn ( mn). Aucune laparoconversion. Nb moyen de gg en lombo-aortique 13 et 14 en pelvien. Durée moyenne d’hospitalisation 3j (2 à 5j) 15/25 avec métastases ganglionnaires dont 2 pelvien et lombo-aortique aucun lombo-aortique isolé. Complications per-opératoires: saignement 3 cas. Complications post-opératoires immédiates: 1 ascite chyleuse,. 1 abcès traité par antibiotique.Complications tardives: 2 lymphocèles, 10 CHE secondaires: fistules urétérales (n=3) et fistule recto-vaginale (n=1).
 entre 2001 et Durée opératoire: 204 mn ( mn). Aucune laparoconversion. Nb moyen de gg en lombo-aortique 13 et 14 en pelvien. Durée moyenne d’hospitalisation 3j (2 à 5j) 15/25 avec métastases ganglionnaires dont 2 pelvien et lombo-aortique aucun lombo-aortique isolé. Complications per-opératoires: saignement 3 cas. Complications post-opératoires immédiates: 1 ascite chyleuse,. 1 abcès traité par antibiotique.Complications tardives: 2 lymphocèles, 10 CHE secondaires: fistules urétérales (n=3) et fistule recto-vaginale (n=1).")
38
Facteurs de risque de récidive
Rouzier et coll, Eur J Surg Oncol 2005

39
Résultats histologiques après radio-chimiothérapie concomitante néo-adjuvante
Houvenaeghel et coll, Gynecol Oncol 2006

41
Indications de la trachélectomie
Stage IA1 avec emboles vasculaires. Stage IA2 ou IB1 ≤ 2 cm. Pas d’envahissement de la partie haute du canal cervical. Pas d’atteinte ganglionnaire. Lésion exophytique pure < 3 cm Since the first report of radical trachelectomy by Dargent, the indications have been clarified. Only women with etc are good candidates for radical trachelectomy.

42
Caractéristiques des patientes ayant eu une trachélectomie
Recently, in a large series, Plante and Roy reported a renouncement to radical trachelectomy in 10 out of 82 women. The sole difference between the two groups was a higher rate of grade 3 tumours in women who underwent a renouncement to the radical trachelectomy. Plante et al, Gynecol Oncol 2004

43
Cause de renoncement à la trachélectomie
The reasons for renouncement, were a positive margins in 5 cases and pelvic positive nodes in 4 cases. In our experience, 3 women required a second operation after first radical trachelectomy for pelvic node metastases in 2 cases and for positive margins in 1 case not diagnosed by intra-operative histology. Plante et al, Gynecol Oncol 2004

44
Complications de la trachélectomie.
Five major intra-operative complications were reported during radical trachelectomy. Among them, 3 required a conversion to laparotomy. As for radical hysterectomy, the main post-operative complications of radical trachelectomy were related to bladder dysfunction. Plante et al, Gynecol Oncol 2004

45
Faisabilité, récidives et mortalité de la trachélectomie
In a review including 319 women who underwent a radical trachelectomy, recurrence and mortality rates appear acceptable ranging between 0 and 7.3%, and 0 and 4.2%, respectively. In addition, it is important to note that the rate of renouncement to radical trachelectomy was about 10%. Therefore, women have to be informed on this risk.

46
Sites de récidives après trachélectomie
Recurrence locations were mainly nodal and represented more than one third of all recurrences followed by parametrial recurrences. In our experience, one ovarian recurrence 18 months after first treatment occurred in a woman with stage IB1 adenocarcinoma of 11 mm of diameter with negative margins and pelvic lymph nodes raising the issue of trachelectomy for adenocarcinoma. However, in the review of Plante and Roy, adenocarcinoma did not appeared a risk factor for recurrence. histology of the tumour did not appeared a criterion to exclude women from conservative management.

47
Fertilité après trachélectomie
In addition to the recurrence rate, main end-points for radical trachelectomy are pregnancy rate and reproductive outcome. The mean conception rate reaches 45%. With a birth rate of 58% due a high rate of foetal losses during the second trimester of pregnancy.

48
Taux actuariel de conception après trachélectomie (95% CI)
Bernardini noted that 95% of pregnancies were obtained in the 36 months following radical trachelectomy. Bernardini et al, Am J Obstet Gynecol 2003

49
Gynecol Oncol, 2006

50
Conclusion Laparoscopic radical hysterectomy for cervical cancer offers similar DFS and OS than laparotomy. Indications for locally advanced stages remains controversial. Radical trachelectomy is a safe option to spare fertility with an acceptable recurrence rate.

51
Pelvic lymph node metastases in cervical cancers

52
Vaginal radical trachelectomy
Schlaerth et al, Am J Obstet Gynecol 2003

53
Vaginal radical trachelectomy
Schlaerth et al, Am J Obstet Gynecol 2003

54
Abdominal radical trachelectomy
Rodriguez et al, Am J Obstet Gynecol 2001

55
Abdominal radical trachelectomy
Rodriguez et al, Am J Obstet Gynecol 2001

56
Retroperitoneal drainage after paraaortic lymphadenectomy
Morice et al, Obstet Gynecol 2001

57
Disease-free survival after LARVH according to tumor stage
Hertel et al, Gynecol Oncol 2003

58
Risk factors for recurrence after radical hysterectomy

59
Survival after trachelectomy and renouncement for trachelectomy
Plante et al, Gynecol Oncol 2004

60
Radical trachelectomy
Whatever the series, the mean follow-up remains short. The rate of recurrence ranged between 0 to 8.3%.

61
Proposal for management of women with Stage IB2 / II
Abdomino-pelvic MRI or CT scan Suspicious PA nodes Absence of suspicious PA nodes Radioguided percutaneous puncture Positive PA nodes Negative PA nodes Initial Para-aortic lymphadenectomy Positive PA nodes Negative PA nodes External pelvic+ PA radiation therapy (45 Gy) with concomitant chemotherapy (cisplatin 40 + brachytherapy (15 Gy)
 with concomitant chemotherapy. (cisplatin 40 + brachytherapy (15 Gy)")
Présentations similaires