Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Journal Club 13-2-19 Constantin Filip C’est-tu mon cœur, docteur?
MCAS et angine stable en 2013… Dernières lignes directrices américaines (Nov. 2012) et algorithmes de prise en charge Constantin Filip
 et algorithmes de prise en charge. Constantin Filip.")
2
Paru le: 20 NOVEMBRE 2012 1. From: Diagnosis of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons 2. From: Management of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons Ann Intern Med. 2012;157(10): doi: /
: doi: /")
3
Abbréviations FHQ: forte recommendation, haute qualité des données probantes FMQ : forte recommendation, qualité moyenne des données probantes FQF : forte recommandation, qualité faible des données probantes Forte recommendation : -le bénéfice clairement excède de risque -le risque clairement excède le bénéfice

4
Angine

5
Angine Angine typique (définitive) Angine atypique (probable)
Douleur ou inconfort rétrosternal d’une qualité/durée charactéristiques (<30 min) Provoquée par l’effort ou le stress émotionnel Soulagée par le repos ou la NTG Angine atypique (probable) 2 critères sur 3 Douleur « non-cardiaque » 1 critère ou moins
 Provoquée par l’effort ou le stress émotionnel. Soulagée par le repos ou la NTG. Angine atypique (probable) 2 critères sur 3. Douleur « non-cardiaque » 1 critère ou moins.")
6
Angine La caractérisation OPQRST clinique de la douleur thoracique devrait toujours être associée au questionnaire sur les facteurs de risque pour la maladie ischémique coronarienne Classifier stable versus instable Instable si au repos, classe fonctionnelle III ou IV de novo, classe III ou IV crescendo

7
Un ‘petit’ mot sur l’angine instable

8
Facteurs de risque Non modifiables Âge Sexe (homme>femme)
ATCD familiaux

9
Facteurs de risque Modifiables Tabagisme Dyslipidémie Sédentarité
Excès de poids Hypertension Diabète

10
Angine Classes fonctionnelles :
Société Canadienne de Cardiologie Classe I : symptômes lors d’efforts importants, rapides ou prolongés (>7mets) Classe II : limitation légère, marche rapide >2 pâtés de maison, monter >1 palier d’escalier (5-7 mets) Classe III : limitation marquée, marcher 1-2 pâtés plat, monter un palier d’escalier (2-5 mets) Classe IV : incapacité ± symptômes aux repos (<2 mets)
 Classe II : limitation légère, marche rapide >2 pâtés de maison, monter >1 palier d’escalier (5-7 mets) Classe III : limitation marquée, marcher 1-2 pâtés plat, monter un palier d’escalier (2-5 mets) Classe IV : incapacité ± symptômes aux repos (<2 mets)")
11
Le diagnostic différentiel

12
Objectifs… Première question : Comment doit-on évaluer un patient avec DRS qui suggère une maladie cardiaque ischémique? Deuxième question : Comment faire pour évaluer le risque de décès ou d’infarctus du myocarde si le diagnostic est positif? Troisième question : Quelle devrait être l’approche pour combattre les facteurs de risque qui contribuent à la morbidité et la mortalité de la maladie coronaire ischémique? Quatrième question : Quel est le rôle de la revascularisation dans la réduction de morbidité et de mortalité associée à la maladie coronaire ischémique? (pas couvert dans cette présentation) Cinquième question : Comment les symptômes cliniques d’angine devraient-ils être « managés » avec la pharmacothérapie?
 Cinquième question : Comment les symptômes cliniques d’angine devraient-ils être « managés » avec la pharmacothérapie")
13
Les recommendations Ann Intern Med. 2012;157(10): doi: /

14
À noter Noter que les études inclues dans la revue de la littérature sont publiées avant Novembre le temps de rédiger/éditer/publier les articles. R1-28 pour Diagnostic R1-48 pour Management

15
Diagnostic (R1) Faire l’histoire et l’examen physique pour établir la probabilité PRÉ-test de maladie coronarienne ischémique stable FQF

16
Probabilité pré-test Probabilité intermédiaire est définie comme étant de 10-90%.

17
Probabilité pré-test

18
(R4) Faire un ECG de repos, sauf si la douleur thoracique a une cause non-cardiaque évidente FMQ
 Faire un ECG de repos, sauf si la douleur thoracique a une cause non-cardiaque évidente FMQ")
19
(R5) Faire un ECG à l’effort si l’ECG de base est interprétable et un fonctionnement physique au moins modéré ou sans comorbidité invalidante FQF

20
ECG non-interpretable
BBG complet Pacemaker pré-excitation (Wolff-Parkinson-White) >1mm dépression onde ST au repos Hypertrophie VG
 >1mm dépression onde ST au repos. Hypertrophie VG.")
21
(R6) Faire un stress test avec échocardiographe / perfusion de radionucléide si l’ECG est non- interprétable FMQ

22
(R9) Faire un stress test pharmacologique nucléaire ou avec écho cardiaque si incapable d’atteindre un niveau de fonctionnement physique modéré ou présence de comorbidité incapacitante FMQ
 Faire un stress test pharmacologique nucléaire ou avec écho cardiaque si incapable d’atteindre un niveau de fonctionnement physique modéré ou présence de comorbidité incapacitante FMQ")
23
(R11) Faire un écho cardiaque en plus si histoire d’infarctus, ondes Q pathologiques, signes ou symptômes d’insuffisance cardiaque, arythmies ventriculaires complexes, ou souffle cardiaque non diagnostiqué. FMQ

24
Copyright © The American College of Physicians.
From: Diagnosis of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons Ann Intern Med. 2012;157(10): doi: / Figure Legend: † CCTA is reasonable only for patients with intermediate probability of IHD. Date of download: 2/16/2013 Copyright © The American College of Physicians. All rights reserved.
: doi: / Figure Legend: † CCTA is reasonable only for patients with intermediate probability of IHD. Date of download: 2/16/2013. Copyright © The American College of Physicians. All rights reserved.")
25
Figure 1. Le diagnostic chez les patients à risque de maladie cardio-ischémie
Figure 1. Diagnosis of patients suspected of having ischemic heart disease. CCTA computed coronary tomography angiography; CMR cardiac magnetic resonance; ECG electrocardiogram; echo echocardiography; IHD ischemic heart disease; MPI myocardial perfusion imaging; UA unstable angina; UA/NSTEMI unstable angina/non–ST-segment elevation myocardial infarction. * See Table 2 of reference 2 for short-term risk of death or nonfatal myocardial infarction in patients with UA/NSTEMI. † CCTA is reasonable only for patients with intermediate probability of IHD.

26
Le score Duke (avec protocole Bruce) L’angiographie
Deuxième question : Comment faire pour évaluer le risque de décès ou d’infarctus du myocarde si le diagnostic d’MCAS est entretenu? Le score Duke (avec protocole Bruce) L’angiographie Duke score (exercise time in minutes minus (5 × ST-segment deviation, during or after exercise, in millimeters) minus (0 if there is no angina, 4 if angina occurs, and 8 if angina is the reason for stopping the test) Patients are classified as low, moderate, or high risk according to the score: Low-risk – score ≥+5 Moderate-risk — score from – 10 to +4 High-risk – score ≤-11
 L’angiographie. Duke score (exercise time in minutes minus (5 × ST-segment deviation, during or after exercise, in millimeters) minus (0 if there is no angina, 4 if angina occurs, and 8 if angina is the reason for stopping the test) Patients are classified as low, moderate, or high risk according to the score: Low-risk – score ≥+5. Moderate-risk — score from – 10 to +4. High-risk – score ≤-11.")
27
Cavéat : ECG à l’effort NB. Les B-bloqueurs ne devraient pas être données 2 jours avant le test (sevrés si possible pour éviter rebond) (idéalement). La sensibilité du test est relativement faible (autour de 50%) alors si la suspicion clinique est forte, ne pas choisir l’épreuve d’effort par ECG, mais par une méthode par imagerie.
 (idéalement). La sensibilité du test est relativement faible (autour de 50%) alors si la suspicion clinique est forte, ne pas choisir l’épreuve d’effort par ECG, mais par une méthode par imagerie.")
28
Indications d’angiographie
(R21) … pour les survivants d’un ‘sudden cardiac death’ ou V-tach/fib. FMQ (R22)… pour l’insuffisant cardiaque de novo (chez pt auparavant stable) (R23)… pour angine stable sévère FQF (R24)… pour angine stable dont les tests révèlent un risque grave FQF
 … pour les survivants d’un ‘sudden cardiac death’ ou V-tach/fib. FMQ. (R22)… pour l’insuffisant cardiaque de novo (chez pt auparavant stable) (R23)… pour angine stable sévère FQF. (R24)… pour angine stable dont les tests révèlent un risque grave FQF.")
29
Copyright © The American College of Physicians.
From: Diagnosis of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons Ann Intern Med. 2012;157(10): doi: / Numerous factors influence prognosis, including sociodemographic characteristics (age, sex, socioeconomic status), cardiovascular risk factors (smoking, hypertension, dyslipidemia, family history of premature IHD, obesity, sedentary lifestyle), coexisting medical conditions (diabetes; chronic kidney disease; chronic obstructive pulmonary disease; and inflammatory conditions, such as rheumatoid arthritis and systemic lupus erythematosus), coexisting cardiovascular conditions (heart failure, peripheral arterial or cerebrovascular disease), psychosocial characteristics (depression, poor social support), symptoms (especially anginal frequency), functional capacity, and severity of cardiac disease (degree and distribution of stenoses, findings on exercise testing and stress imaging, LV function). Figure Legend: CCTA = coronary computed tomography angiography; CMR = cardiac magnetic resonance; ECG = electrocardiogram; echo = electrocardiography; LBBB = left bundle branch block; MPI = myocardial perfusion imaging. Date of download: 2/16/2013 Copyright © The American College of Physicians. All rights reserved.
: doi: / Numerous factors influence prognosis, including sociodemographic characteristics (age, sex, socioeconomic status), cardiovascular risk factors (smoking, hypertension, dyslipidemia, family history of premature IHD, obesity, sedentary lifestyle), coexisting medical conditions (diabetes; chronic kidney disease; chronic obstructive pulmonary disease; and inflammatory conditions, such as rheumatoid arthritis and systemic lupus erythematosus), coexisting cardiovascular conditions (heart failure, peripheral arterial or cerebrovascular disease), psychosocial characteristics (depression, poor social support), symptoms (especially anginal frequency), functional capacity, and severity of cardiac disease (degree and distribution of stenoses, findings on exercise testing and stress imaging, LV function). Figure Legend: CCTA = coronary computed tomography angiography; CMR = cardiac magnetic resonance; ECG = electrocardiogram; echo = electrocardiography; LBBB = left bundle branch block; MPI = myocardial perfusion imaging. Date of download: 2/16/2013. Copyright © The American College of Physicians. All rights reserved.")
30
Figure 2. L’évaluation du risque des patients avec maladie cardio-ischémique stable.

31
Troisième question : Quelle devrait être l’approche pour combattre (les facteurs de risque qui contribuent à) la morbidité et la mortalité de la maladie coronaire ischémique?
 la morbidité et la mortalité de la maladie coronaire ischémique")
32
Diète (R4) Gras saturés <7% des calories totales
R1 à 3 : sans grand intérêt (R4) Gras saturés <7% des calories totales Gras trans <1% des calories totales Cholesterol <200mg par jour FMQ
 Gras saturés <7% des calories totales. Gras trans <1% des calories totales. Cholesterol <200mg par jour. FMQ.")
33
Dyslipidémie R5 Statines (si non contre-indiqué, et toléré). FHQ
evidence has established the efficacy of statins in the primary and secondary prevention of coronary events (15–17, 31, 78–83). Each 40-mg/dL (1mmol/L) reduction in LDL cholesterol was associated with a 12% reduction in all cause mortality and 19% reduction in coronary mortality, with corresponding reductions in MI, need for coronary revascularization, and fatal or nonfatal strokes (48). …Si traitement sous-optimal avec statines (forte dose), consiérer séquestrant (cholestyramine) ou niacin, qui ont été démontré efficaces à réduire la mortalité comparés au placébo. Moins de données probantes sur les dérivés d’acid fibrique. Études observationnelles et études de traitement montre un bénéfice des acides oméga-3 à réduire le risque cardiovasculaire. L’Ezetimibe décroit le cholestérol, mais n’a pas été démontré à améliorer les résultats cliniques.
. Each 40-mg/dL (1mmol/L) reduction in LDL cholesterol was associated with a 12% reduction in all cause mortality and 19% reduction in coronary mortality, with corresponding reductions in MI, need for coronary revascularization, and fatal or nonfatal strokes (48). …Si traitement sous-optimal avec statines (forte dose), consiérer séquestrant (cholestyramine) ou niacin, qui ont été démontré efficaces à réduire la mortalité comparés au placébo. Moins de données probantes sur les dérivés d’acid fibrique. Études observationnelles et études de traitement montre un bénéfice des acides oméga-3 à réduire le risque cardiovasculaire. L’Ezetimibe décroit le cholestérol, mais n’a pas été démontré à améliorer les résultats cliniques.")
34
Activité physique R9 Encourager à faire min d’activité aérobique en intensité modérée, (e.g. marche rapide), ≥5x/sem (préférablement die) FMQ Faire un programme médical supervisé (‘réhab’ cardiaque) si haut risque. FHQ high risk for cardiac complications : a history of multiple MIs cardiac arrest, New York Heart Association functional class 3 or 4 exercise capacity less than 6 METs [metabolic equivalents], or significant exercise-induced ischemia on treadmill testing)
, ≥5x/sem (préférablement die). FMQ. Faire un programme médical supervisé (‘réhab’ cardiaque) si haut risque. FHQ. high risk for cardiac complications : a history of multiple MIs. cardiac arrest, New York Heart. Association functional class 3 or 4. exercise capacity less than 6 METs [metabolic equivalents], or. significant exercise-induced ischemia on treadmill testing)")
35
Surveillance du poids R10 IMC ou tour de taille qvisite
IMC 18.5 à 24.9 (kg/m2) tour de taille <40 po (hommes) <35 po (femmes) (Caucasien) FQF
 tour de taille <40 po (hommes) <35 po (femmes) (Caucasien) FQF.")
36
Interventions non suggérées* (e.g. sans ou peu de bénéfices)
Estrogène pour femmes ménopausées FHQ Vitamine C, E, B-carotene FHQ Folate/B6/B12 avec ou sans homocystéinémie FHQ Chélation (EDTA) FQF Ail, sélénium, chromium FQF (*Pas pour cette indication (MCAS)… en connaissez-vous d’autres)
 FQF. Ail, sélénium, chromium FQF. (*Pas pour cette indication (MCAS)… en connaissez-vous d’autres)")
37
Pharmacothérapie pour prévention de l’infarctus (IM) et/ou de mort
 et/ou de mort")
38
Rx… prévention (IM)/mort
En absence de C-I, l’AAS mg est à continuer indéfiniment chez le patient atteint de maladie ischémique coronarienne. FHQ

39
Rx… prévention (IM)/mort
Contre-indications à l’AAS: Relatives Allergies aux AINS Syndrome asthme / rhinite /polypes nasaux

40
Rx… prévention (IM)/mort
Le Clopidogrel (Plavix) est une alternative raisonable si l’AAS n’est pas indiqué. FMQ
 est une alternative raisonable si l’AAS n’est pas indiqué. FMQ.")
41
Rx… prévention (IM)/mort
Thérapie avec un Beta-bloqueur devrait être initiée et continuée pour 3 ans chez tous les patients post-IM ou -SCA si FVG normale. FMQ

42
Rx… prévention (IM)/mort
Métoprolol, carvedilol ou bisoprolol devraient être utilisés si FVG<40% avec insuffisance cardiaque ou IM antérieur sauf si contre- indiqué. FHQ

43
Rx… prévention (IM)/mort
Contre-indications aux beta-bloqueurs: Absolues Bradycardie sévère Bloc atrioventriculaire haut degré sick sinus syndrome Insuffisance cardiaque réfractoire Relatives Bronchospasme, MAP active (vasodilatation)
")
44
Rx… prévention (IM)/mort
Beta-bloqueurs: Attention chez diabétiques type I Cessation abrupte dangereuse Viser 1-3 semaines de ‘sevrage’ Risque d’infarctus, ‘sudden death’ rebond

45
Rx… prévention (IM)/mort
Un IECA est recommandé si HTA avec DB/FE<40% et/ou IRC si pas contre-indiqué FHQ

46
Rx… prévention (IM)/mort
IECA Contreindications Angioedème/allergie Sténose rénale artérielle Sténose aortique sévère

47
Rx… prévention (IM)/mort
ARA, si IECA indiqué et non-toléré. FHQ

48
Rx… prévention (IM)/mort
Vaccin annuel influenza! FMQ Démontré que l’influenza cause l’hospitalisation et entraîne la mortalité. Organisation mondiale de la santé se rajoute à ces recommendations!

49
Pharmacothérapie pour symptomatologie
Les beta-bloqueurs sont le premier choix. FMQ

50
Pharmacothérapie pour symptomatologie
Les ICC ou nitrates avec action-prolongée lorsque beta-bloqueurs sont contre-indiqués ou non-tolérés. FMQ

51
Pharmacothérapie pour symptomatologie
Effets secondaires des beta-bloqueurs : Nausée, diarrhée, bronchospasme, fatigue étourdissement (*hypotension/orthostatique), dyspepsie, céphalée, intolérence au froid/↑Raynaud, dysfonction érectile. hypoglycémies
, dyspepsie, céphalée, intolérence au froid/↑Raynaud, dysfonction érectile. hypoglycémies.")
52
Pharmacothérapie pour symptomatologie
Les ICC ou nitrates action-prolongée, en combinaison avec beta-bloqueurs si échec aux beta-bloqueurs seuls. FMQ

53
Pharmacothérapie pour symptomatologie
La nitroglycérine SL ou spray devrait être utilisée pour le soulagement immédiat. FMQ

54
Pharmacothérapie pour symptomatologie
L’acupuncture n’est pas recommandé comme alternative. FQF

55
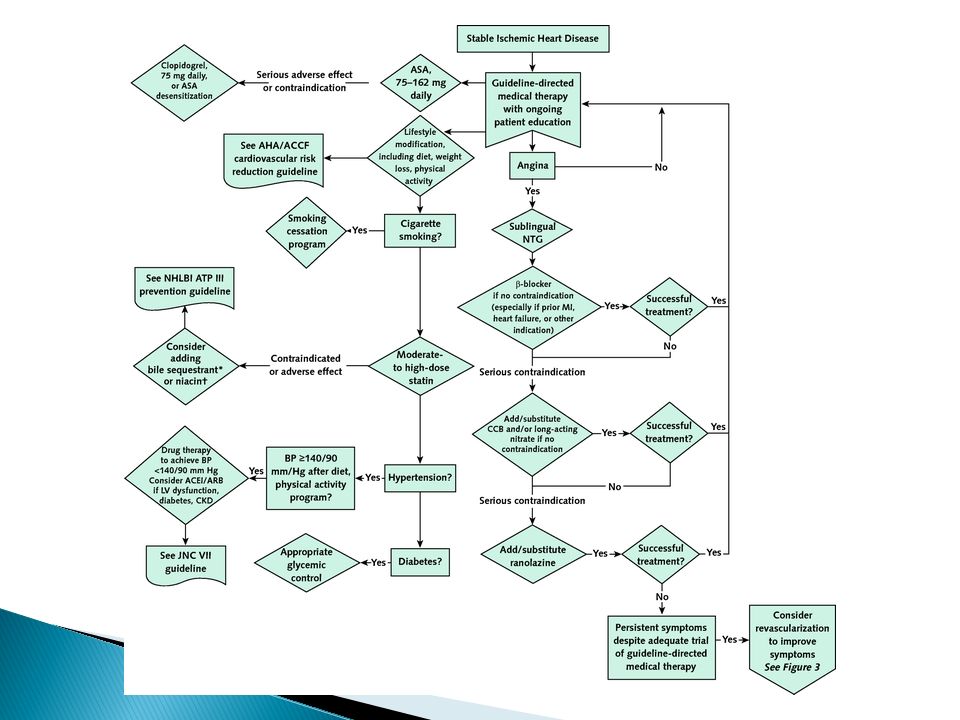
Copyright © The American College of Physicians.
From: Management of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons Ann Intern Med. 2012;157(10): doi: / Figure Legend: † Dietary supplement niacin must not be used as a substitute for prescription niacin. Copyright © The American College of Physicians. All rights reserved.
: doi: / Figure Legend: † Dietary supplement niacin must not be used as a substitute for prescription niacin. Copyright © The American College of Physicians. All rights reserved.")
57
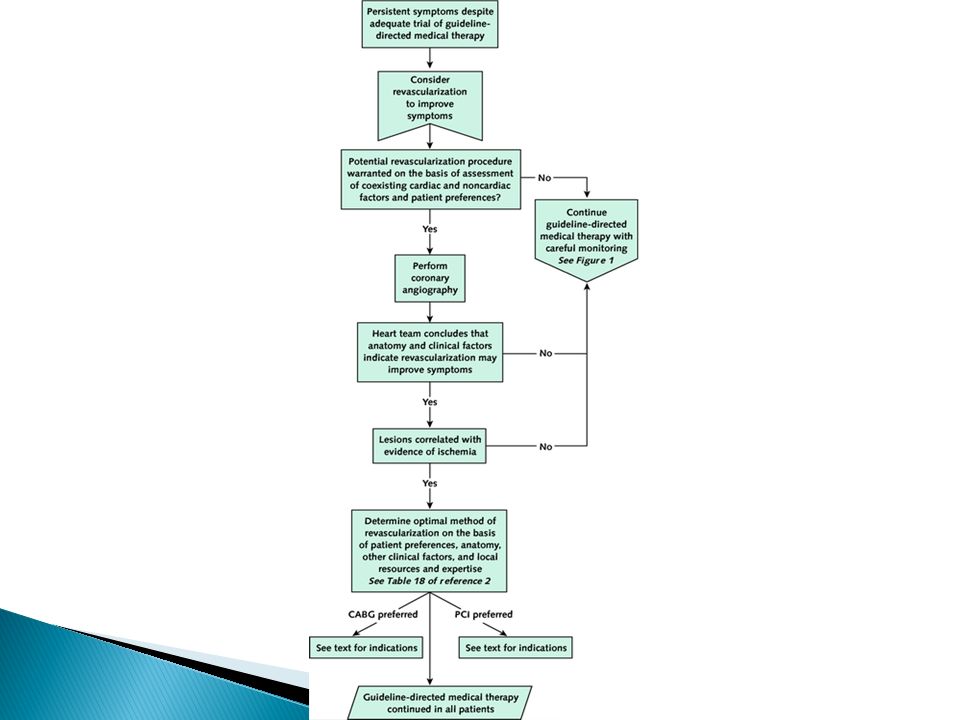
Copyright © The American College of Physicians.
From: Management of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons Ann Intern Med. 2012;157(10): doi: / Figure Legend: Revascularization to improve survival of patients with stable ischemic heart disease. Date of download: 2/16/2013 Copyright © The American College of Physicians. All rights reserved.
: doi: / Figure Legend: Revascularization to improve survival of patients with stable ischemic heart disease. Date of download: 2/16/2013. Copyright © The American College of Physicians. All rights reserved.")
59
Copyright © The American College of Physicians.
From: Management of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons Ann Intern Med. 2012;157(10): doi: / Figure Legend: CABG = coronary artery bypass grafting; PCI = percutaneous coronary intervention. Date of download: 2/16/2013 Copyright © The American College of Physicians. All rights reserved.
: doi: / Figure Legend: CABG = coronary artery bypass grafting; PCI = percutaneous coronary intervention. Date of download: 2/16/2013. Copyright © The American College of Physicians. All rights reserved.")
61
References Articles en question (1,2) UpToDate.com (3)
Amir Qaseem, Stephan D. Fihn, Sankey Williams, Paul Dallas, Douglas K. Owens, Paul Shekelle, ; Diagnosis of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons. Annals of Internal Medicine Nov;157(10): Amir Qaseem, Stephan D. Fihn, Paul Dallas, Sankey Williams, Douglas K. Owens, Paul Shekelle, ; Management of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons. Annals of Internal Medicine Nov;157(10): UpToDate.com (3) DCC 26 (Ulaval) (4)
: Amir Qaseem, Stephan D. Fihn, Paul Dallas, Sankey Williams, Douglas K. Owens, Paul Shekelle, ; Management of Stable Ischemic Heart Disease: Summary of a Clinical Practice Guideline From the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons. Annals of Internal Medicine Nov;157(10): UpToDate.com (3) DCC 26 (Ulaval) (4)")
Présentations similaires



















 % de la.>")
