Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Cas clinique d’infection sur prothèse articulaire
Aurélien Dinh Maladies Infectieuses, Hôpitaux Universitaires Paris Ile de France Ouest Centre de référence des infections ostéo articulaires Université Versailles Saint Quentin

2
Cas clinique Monsieur X, 79 ans
Consulte pour douleur de hanche droite évoluant depuis 3 semaines avec fistulisation et écoulement à la peau depuis 2j. ATCD : Diabète + PTH droite (il y a 3 ans) Examen clinique : Apyrétique, douleur de hanche à la mobilisation. Bilan biologique : CRP = 55mg/l ; VS 100 ml/h Vous suspectez une infection sur prothèse ostéo articulaire
 Examen clinique : Apyrétique, douleur de hanche à la mobilisation. Bilan biologique : CRP = 55mg/l ; VS 100 ml/h. Vous suspectez une infection sur prothèse ostéo articulaire.")
3
Q1 : Quels examens complémentaires demandez vous pour étayer le diagnostic?
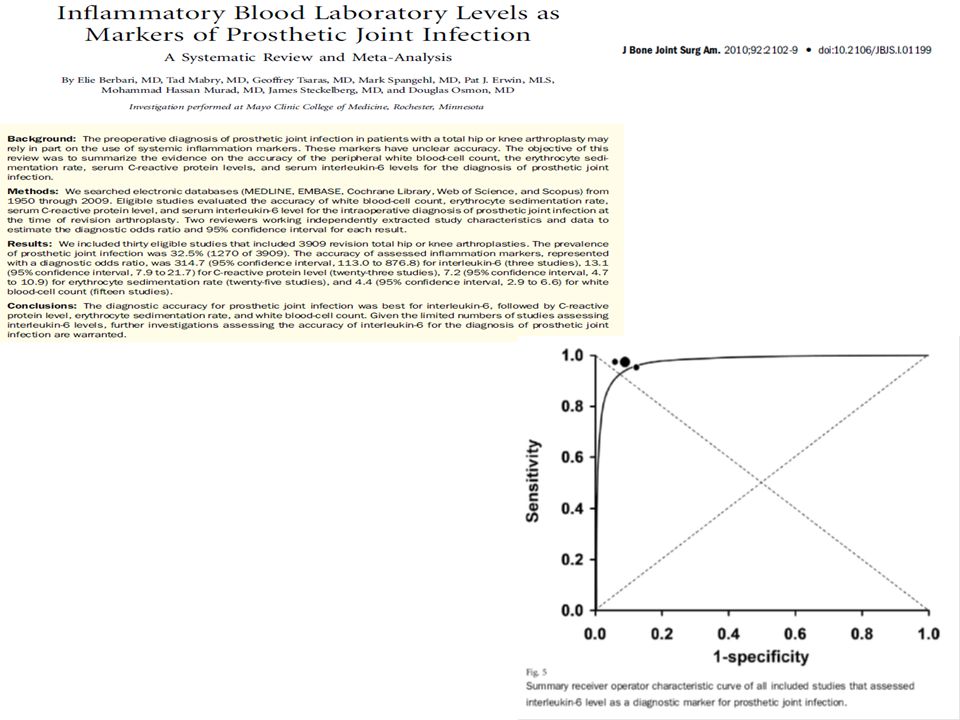
VS CRP Radio Alb IL6 ? Faisceau d’argument Pas d’ATB sans confirmation diagnostique dans la mesure du possible Diagnostic certains d’après la clinique VS peu spécifique IRm excellente VPN

4
Q1 : Quels examens complémentaires demandez vous pour étayer le diagnostic?
VS CRP Radio Alb IL6 ? Faisceau d’argument Pas d’ATB sans confirmation diagnostique dans la mesure du possible Diagnostic certains d’après la clinique VS peu spécifique IRm excellente VPN

5
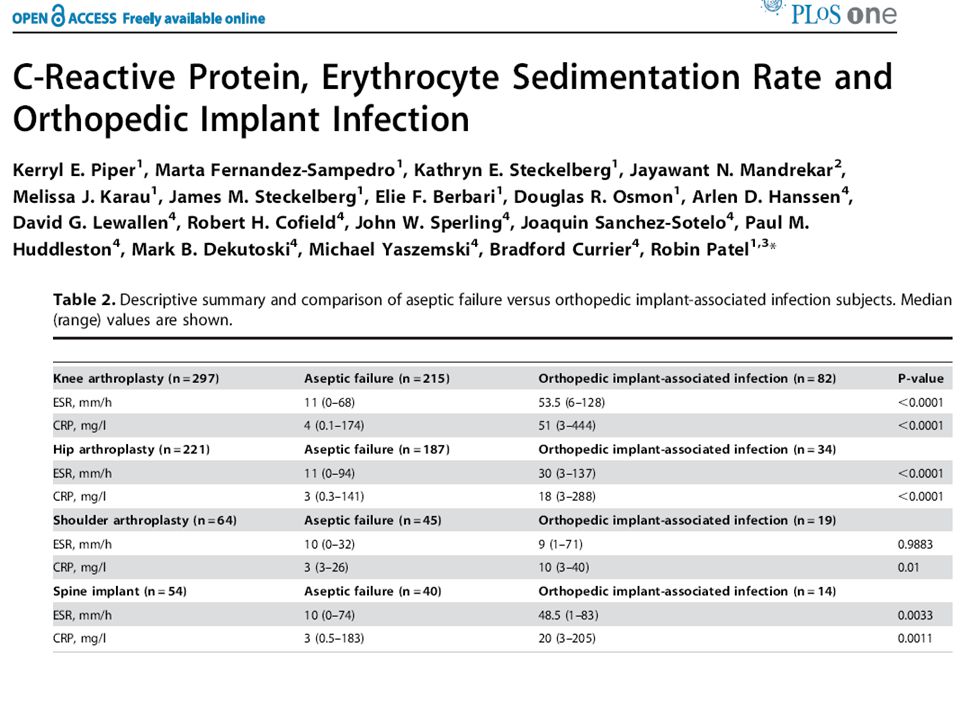
Examens complémentaires pour confirmer le diagnostic ?
Aucun n’est sensible ni spécifique !!! VS ou CRP normales >>n’élimine pas l’infection. Dans le mois qui suit l’implantation, la courbe d’évolution de la CRP a une valeur diagnostique mais pas la VS Biologiquement, à 3 mois de l’implantation une VS > 22-30 mm : sensibilité 82 -93 % spécificité 84 %, une CRP > 10 à 13,5 mg/l sensibilité % spécificité entre 86-92 % SPILF RCP Infections ostéoarticulaires sur matériel 2009

8
Q2 : Que proposez vous pour tenter d’obtenir un diagnostic microbiologique?
Ponction articulaire (conditions stériles) Cathétérisme de la fistule Écouvillon de surface Intervention chirurgicale avec prélèvements per op Aucun : antibiothérapie probabiliste
 Cathétérisme de la fistule. Écouvillon de surface. Intervention chirurgicale avec prélèvements per op. Aucun : antibiothérapie probabiliste.")
9
Q2 : Que proposez vous pour tenter d’obtenir un diagnostic microbiologique?
Ponction articulaire (conditions stériles) Cathétérisme de la fistule Écouvillon de surface Intervention chirurgicale avec prélèvements per op Aucun : antibiothérapie probabiliste
 Cathétérisme de la fistule. Écouvillon de surface. Intervention chirurgicale avec prélèvements per op. Aucun : antibiothérapie probabiliste.")
10
Intérêt de la ponction pré opératoitre
Phillips, Clin Orthop Related Res PPV = 24%, VPN>90% Barrack, JBJS PPV = 6% (58% SCN) Duff, Clin Orthop Related Res 1996 : PPV = 100% ; VPN>90% Spangehl, JBJS 1999 : PPV = 67% (77% si répétée) Somme, JBS 2003 : PPV = 100% ; VPN = 85% Previous antibiotherapy reduces sensitivity A free antibiotherapy of at least 15 days Eric Senneville (Tourcoing)
 Duff, Clin Orthop Related Res 1996 : PPV = 100% ; VPN>90% Spangehl, JBJS 1999 : PPV = 67% (77% si répétée) Somme, JBS 2003 : PPV = 100% ; VPN = 85% Previous antibiotherapy reduces sensitivity. A free antibiotherapy of at least 15 days. Eric Senneville (Tourcoing)")
11
Ponction articulaire Se 56-75% ; Spe 95-100% Passage en peau saine
Nécessité Asepsie chirurgicale Pas d’ATB préalable (fenêtre >15j) Intérêt d’ensemencement flacon d’hémoculture ? A répéter en cas d’identification de germe potentiellement contaminant ? Difficult in hips and shoulder High risk contaminant or incomplete documentation Trampuz NEJM 2007 ; Fink JBJS ; Virolainen Scand J Surg 2002 ; Hugues JCM 2001
 Intérêt d’ensemencement flacon d’hémoculture A répéter en cas d’identification de germe potentiellement contaminant Difficult in hips and shoulder. High risk contaminant or incomplete documentation. Trampuz NEJM 2007 ; Fink JBJS 2008 ; Virolainen Scand J Surg 2002 ; Hugues JCM")
12
Expérience CRIOA V. Zeller et al. JNI 2012

13
Q3 : Quelles techniques microbiologiques permettent d’optimiser le diagnostic ?
Nombreux prélèvements Sonication PCR Cultures prolongées Nouveaux prélèvements

14
Q3 : Quelles techniques microbiologiques permettent d’optimiser le diagnostic ?
Nombreux prélèvements Sonication PCR Cultures prolongées Nouveaux prélèvements

15
«Fenêtre» antibiotique avant biopsie osseuse (infection chronique)
Witso et al. Acta Orthop Scand, 1999

16
Nombre de prélèvements positifs
N positive Histology PPV (%)* specimens + - ³ ,4** *** ,2 ,6 Study based on mathematical model 5 to 6 specimens submitted for culture 2 or 3 culture positive samples should be considered for diagnosis depending of the micro organism Relire méthodo papier We can say that for diagnosis strategy we need numerous and different specimens during intervention To try to identify the micro organism involve and to avoid the potential contaminant Indication of pre operative punction ? * : compared with histology (> 5 PMN/HPF) ** : whatever the microorganism *** : for CNS Atkins et al.JCM 1998
* specimens + - ³ ,4** *** , ,6. Study based on mathematical model. 5 to 6 specimens submitted for culture. 2 or 3 culture positive samples should be considered for diagnosis depending of the micro organism. Relire méthodo papier. We can say that for diagnosis strategy we need numerous and different specimens during intervention. To try to identify the micro organism involve and to avoid the potential contaminant. Indication of pre operative punction * : compared with histology (> 5 PMN/HPF) ** : whatever the microorganism. *** : for CNS. Atkins et al.JCM")
17
Culture prolongée nécessaire
Could be interesting but it take time The risk of isolating a contaminnat rise with the time of culture Schäfer et al CID 2008

18
Sonication de matériel
Mais : non applicable en pré opératoire pas applicable en cas de maintient de l’implant 1 seul résultat >> problème des contaminants Only available in highly specialized centers Trampuz, NEJM 2007

19
Clinical significance

20
Problem high rate of potential contaminant identification
What is the clinical significance of the results No antibiogram available And it take time and ressources 20

21
Stratégies thérapeutiques chirurgicales
Lavage débridement Changement en 1 temps Changement en deux temps Arthrodèse Résection Organisation en fistule chronique

22
Stratégies thérapeutiques chirurgicales
Lavage débridement Changement en 1 temps Changement en deux temps Arthrodèse Résection Organisation en fistule chronique

23
Efficacité lavage débridement fonction de l’âge de la prothèse et de la durée des symptômes
Bactério. Age de la PT Ref Efficacité Durée des symptômes Délai d’inclusion Nombre de cas Strepto. peniS 2 mois-5ans 1 89.5% <10j (1-10) Mediane 4j 29 ans 19 cas Staph (75%) 1.5 à 3ans 21/34 cas 2 100% 0% 5 j 16 ans 13/34 cas 54 j 3 > 2j 100% 0% Staph (93%) < 2j < 1mois: 40% >1 mois: 60% 11 ans 12/34 21/34 13 < 1an 23 > 1an Staph (86%) > 1 mois 19/36 cas 4 86.% * NS < 1mois 6 ans 17/36 cas 27% 61% > 4 s 22/33 cas 5 Staph (?%) Variable 14j < 4 s 8 ans 11/33 cas 1: Meehan, CID 2003(36: 845-9) 2: Tattevin, CID 1999 (29:292-5) 3: Brandt, CID, 1997(24:914-9) 4: RAO, Clin Ortho Rel Research, 2003(414: 55-60) 5: Hartman, Clin Ortho Rel Research, 1991(273: 113-8)
 Mediane 4j. 29 ans. 19 cas. Staph (75%) 1.5 à 3ans. 21/34 cas % 0% 5 j. 16 ans. 13/34 cas. 54 j. 3. > 2j. 100% 0% Staph (93%) < 2j. < 1mois: 40% >1 mois: 60% 11 ans. 12/34. 21/ < 1an. 23 > 1an. Staph (86%) > 1 mois. 19/36 cas % * NS. < 1mois. 6 ans. 17/36 cas. 27% 61% > 4 s. 22/33 cas. 5. Staph ( %) Variable 14j. < 4 s. 8 ans. 11/33 cas. 1: Meehan, CID 2003(36: 845-9) 2: Tattevin, CID 1999 (29:292-5) 3: Brandt, CID, 1997(24:914-9) 4: RAO, Clin Ortho Rel Research, 2003(414: 55-60) 5: Hartman, Clin Ortho Rel Research, 1991(273: 113-8)")
24
Thérapeutique D’un point de vue microbiologique il convient de privilégier un changement en 2 temps (long ?) Nécessité d’un projet global pour les patients âgés avec en objectif principal la préservation du statut fonctionnel et de l’autonomie. Rétention 1 temps Risque septique Perte fonctionnelle Qualité de vie 2 temps court 2 temps long Young MH. Drugs aging 2008

25
Peser les arguments Maintient du matériel Matériel récent
Sujet âgé, comorbidités sévères Apparition récente des symptômes Peu d’expression clinique de l’infection Staphylocoque coagulase négatif en cause Ablation du matériel Pose ancienne du matériel Sujet jeune, peu d’ATCD Durée d’évolution des symptômes État septique sévère Staphylocoque doré responsable Résistance à un traitement médical bien conduit

28
Efficacité globale La comparaison des différentes études : difficile.
Mais en globalité pour hanche et genou on obtient : Changement en 1 temps : efficacité entre 85 et 90 % Changement en 2 temps : 85 et 95 % Bengtson S. Acta Orthop Scand 1991 ; Mont MA. J Bone Joint Surg Am 2000 Hsieh PH. J Bone Joint Surg Am 2004 Mulcahy DM. Ir J Med Sci 1996 Souillac V. Rev Chir Orthop Reparatrice Appar Mot 2006 Hanssen AD. Clin Orthop Relat Res 1994

29
Efficacité du 2 temps Changement en 2 temps, + espaceur contenant ou non des antibiotiques, + antibiothérapie systémique, >> taux d’éradication de l’infection Au niveau de la hanche : 85 et 100 % (généralement supérieur à 95 %) Au niveau du genou : généralement entre 85 et 90 % Quelle que soit la sensibilité des bactéries aux antibiotiques Brandt CM. Clin Infect Dis 1997 Souillac V. Rev Chir Orthop Reparatrice Appar Mot 2006 Hanssen AD. Clin Orthop Relat Res 1994 Volin SJ. Clin Orthop Relat Res 2004 Lecuire F. Rev Chir Orthop Reparatrice Appar Mot Hirakawa K. J Arthroplasty 1998 Windsor RE. J Bone Joint Surg Am 1990 Nazarian DG. J Arthroplasty 2003 Hsieh PH. J Bone Joint Surg Br Hsieh PH. J Trauma 2004
 Au niveau du genou : généralement entre 85 et 90 % Quelle que soit la sensibilité des bactéries aux antibiotiques Brandt CM. Clin Infect Dis 1997 Souillac V. Rev Chir Orthop Reparatrice Appar Mot Hanssen AD. Clin Orthop Relat Res 1994 Volin SJ. Clin Orthop Relat Res 2004 Lecuire F. Rev Chir Orthop Reparatrice Appar Mot 1999 Hirakawa K. J Arthroplasty Windsor RE. J Bone Joint Surg Am 1990 Nazarian DG. J Arthroplasty 2003 Hsieh PH. J Bone Joint Surg Br 2005 Hsieh PH. J Trauma 2004")
30
Q4 : Quelle antibiothérapie post opératoire précoce prescrivez vous ?
Daptomycine Daptomycine + C3G ou tazocilline Vancomycine Vancomycine + C3G ou tazocilline FQ+ RFP

31
Q4 : Quelle antibiothérapie post opératoire précoce prescrivez vous ?
Daptomycine Daptomycine + C3G ou tazocilline Vancomycine Vancomycine + C3G ou tazocilline FQ+ RFP

32
Principe de l’ATB post op
Après le geste chirurgical : but de l’antibiothérapie initiale : diminuer le plus rapidement l’inoculum bactérien résiduel. Antibiothérapie forte dose, IV pour des raisons de tolérance et de biodisponibilité Antibiothérapie initiale : probabiliste ou guidée par les prélèvements préopératoires, adaptée après quelques jours. Antibiothérapie probabiliste la plus fréquente : glycopeptides +/- ? Mais baisse de l’incidence des SARM à l’hôpital et toxicité de la vancomycine ! Hétérogénéité des pratiques selon les centres

33
Pronostic identique pour MRSA et MSSA
E. Senneville CID 2012

34
Résultats per opératoire
Les prélèvements per opératoires retrouvent 5/5 Staphylococcus aureus R : Peni G, Péni M, gentamicine, kanamycine, tobramycine, cycline, ofloxacine, érythromycine triméthoprime-sulfaméthoxazole, acide fusidique S : vancomycine, teicoplanine, rifampicine, daptomycine, fosfomycine, linezolide

35
Q5 : Quelle antibiothérapie adaptée ?
Daptomycine Daptomycine rifampicine Rifampicine linezolide Vancomycine seule Vancomycine rifampicine

36
Q5 : Quelle antibiothérapie adaptée ?
Daptomycine Daptomycine rifampicine Rifampicine linezolide Vancomycine seule Vancomycine rifampicine

38
What is the management of MRSA Bone and Joint Infections
What is the management of MRSA Bone and Joint Infections ? IDSA Clinical Practice Guidelines for the treatment of MRSA infections Debride and drain associated soft tissue abscesses (AII) Some experts recommend adding rifampin BID (BIII) Animal models, small human trials of MSSA osteo Retrospective studies : cure rates of up to 80%; no benefit if debridement Adults Children Vancomycin (BII) Daptomycin (BII) Linezolid (BII) Clindamycin (BIII) TMP-SMX + Rifampin (BII) Vancomycin (AII) Clindamycin (AII) Daptomycin (CIII) Linezolid (CIII) Crompton J Chemotherapy 2009; Rayner Infection 2004; Rao DMID 2007; Euba AAC 2009; Martinez-Aguilar PIDJ 2003, Pelroth Arch Int Med 2008; Van der Auwera AAC 1985, Nordern SMJ 1986; Priest SMJ 2005; Livorsi J Infect 2008 38
 Some experts recommend adding rifampin BID (BIII) Animal models, small human trials of MSSA osteo. Retrospective studies : cure rates of up to 80%; no benefit if debridement. Adults. Children. Vancomycin (BII) Daptomycin (BII) Linezolid (BII) Clindamycin (BIII) TMP-SMX + Rifampin (BII) Vancomycin (AII) Clindamycin (AII) Daptomycin (CIII) Linezolid (CIII) Crompton J Chemotherapy 2009; Rayner Infection 2004; Rao DMID 2007; Euba AAC 2009; Martinez-Aguilar PIDJ 2003, Pelroth Arch Int Med 2008; Van der Auwera AAC 1985, Nordern SMJ 1986; Priest SMJ 2005; Livorsi J Infect")
39
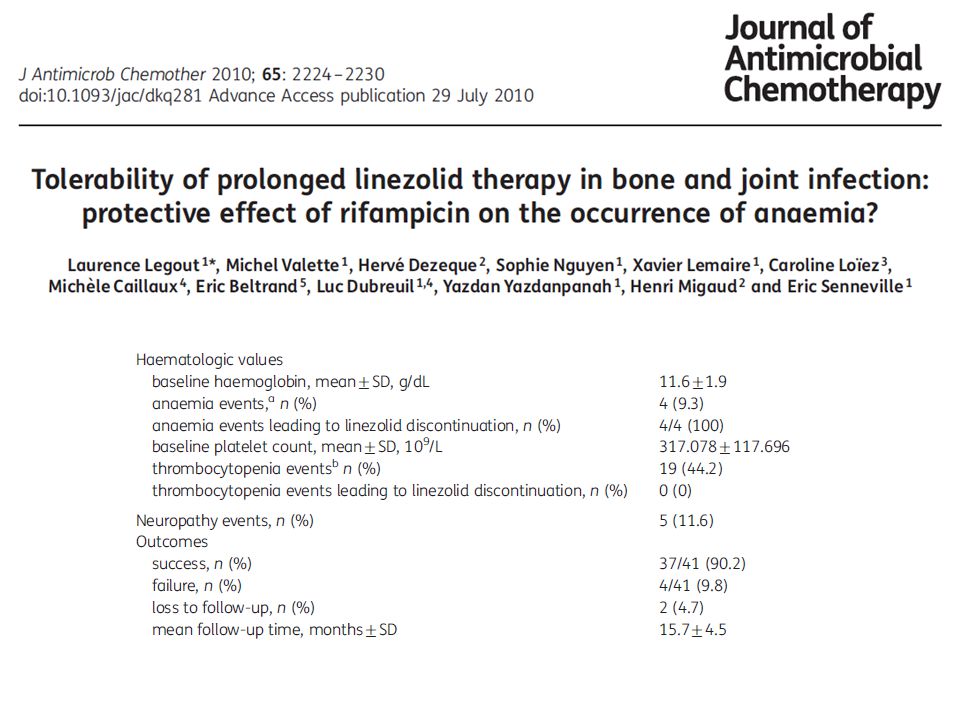
En pratique : la Rifampicine
Peu de molécules répondent à ces critères. La sensibilité à la rifampicine est un élément clé du pronostic MAIS : capacité importante à sélectionner des mutants résistants DONC utilisation obligatoire en bithérapie (+++FQ). 1 seule étude prospective randomisée double aveugle vs placebo : lavage débridement quand infection précoce sur prothèse puis 3 à 6 mois de traitement antibiotique : Antibiothérapie Succès Emergence de résistance à la CPF CPF + RFP 100% CPF + placebo 58% +++ Drancourt M. AAC 1993 Zimmerli JAMA 1998
. 1 seule étude prospective randomisée double aveugle vs placebo : lavage débridement quand infection précoce sur prothèse puis 3 à 6 mois de traitement antibiotique : Antibiothérapie. Succès. Emergence de résistance à la CPF. CPF + RFP. 100% CPF + placebo. 58% +++ Drancourt M. AAC 1993 Zimmerli JAMA")
40
Pronostic identique pour MRSA et MSSA

42
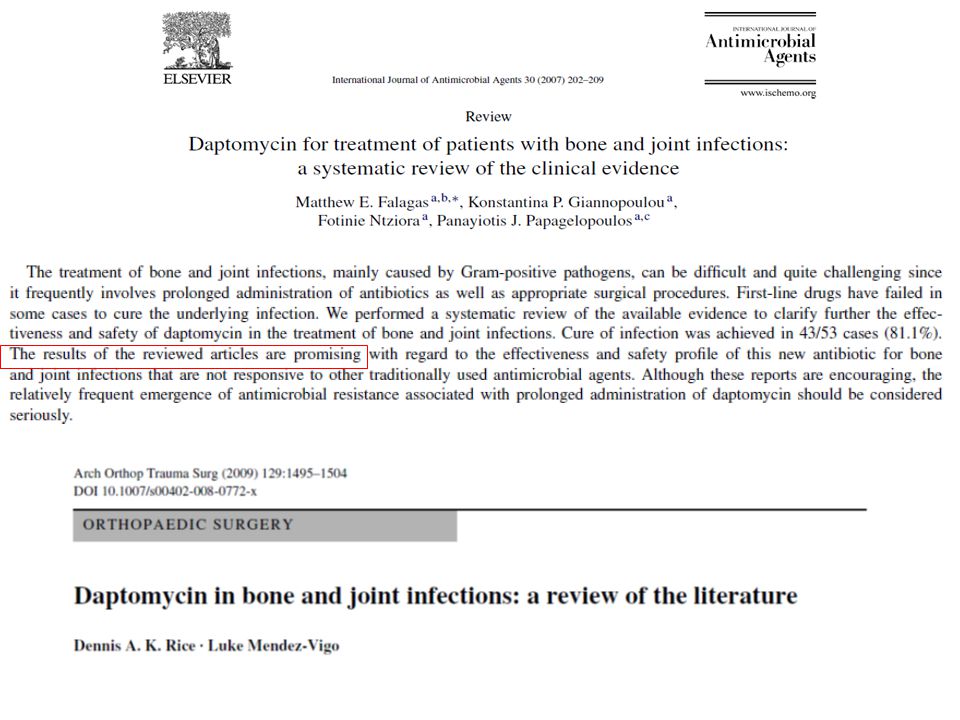
We studied the efficacy of daptomycin at high doses (equivalent to 10 mg/kg/day in humans) and
compared it to that of reference and alternative treatments in a model of foreign-body infection with methicillin (meticillin)-resistant Staphylococcus aureus. In vitro studies were conducted with bacteria in the log and stationary phases. For the in vivo model, therapy with daptomycin at 100 mg/kg/day, vancomycin at 50 mg/kg/12 h, rifampin (rifampicin) at 25 mg/kg/12 h, or linezolid at 35 mg/kg/12 h was administered for 7 days. Antibiotic efficacy was evaluated using either bacteria from tissue cage fluids or those attached to coverslips. We screened for the emergence of linezolid- and rifampin-resistant strains and analyzed the surviving population from the daptomycin-treated group. Only daptomycin was bactericidal in both the log- and stationary-phase studies. Daptomycin (decrease in the log number of CFU per milliliter of tissue cage fluid, 2.57) and rifampin (decrease, 2.6 log CFU/ml) were better (P < 0.05) than vancomycin (decrease, 1.1 log CFU/ml) and linezolid (decrease, 0.9 log CFU/ml) in the animal model. Rifampin-resistant strains appeared in 60% of cases, whereas no linezolid resistance emerged. No daptomycin-resistant subpopulations were detected at frequencies of 107 or higher. In conclusion, daptomycin at high doses proved to be as effective as rifampin, and the two were the most active therapies for this experimental foreign-body infection. These high doses ensured a profile of safety from the development of resistance.
-resistant Staphylococcus aureus. In vitro studies were conducted with bacteria in the log and. stationary phases. For the in vivo model, therapy with daptomycin at 100 mg/kg/day, vancomycin at 50 mg/kg/12. h, rifampin (rifampicin) at 25 mg/kg/12 h, or linezolid at 35 mg/kg/12 h was administered for 7 days. Antibiotic. efficacy was evaluated using either bacteria from tissue cage fluids or those attached to coverslips. We screened. for the emergence of linezolid- and rifampin-resistant strains and analyzed the surviving population from the. daptomycin-treated group. Only daptomycin was bactericidal in both the log- and stationary-phase studies. Daptomycin (decrease in the log number of CFU per milliliter of tissue cage fluid, 2.57) and rifampin (decrease, 2.6 log CFU/ml) were better (P < 0.05) than vancomycin (decrease, 1.1 log CFU/ml) and linezolid (decrease, 0.9 log CFU/ml) in the animal model. Rifampin-resistant strains appeared in 60% of cases, whereas no linezolid. resistance emerged. No daptomycin-resistant subpopulations were detected at frequencies of 107 or higher. In conclusion, daptomycin at high doses proved to be as effective as rifampin, and the two were the most active. therapies for this experimental foreign-body infection. These high doses ensured a profile of safety from the. development of resistance.")
43
Biofilm-associated cell survival of 12 meticillin-resistant Staphylococcus
aureus isolates treated with clindamycin, daptomycin, linezolid, tigecycline and vancomycin at 64g/mL. Each box plot represents the spread of cell survival across the different clinical isolates and the error bars represent the standard deviation between samples. ***P < ; **P <

44
Daptomycin is an attractive option for treating prosthetic joint infection, but the 6-mg/kg of body weight/day dose was linked to clinical failure and emergence of resistance. Using a methicillin-resistant Staphylococcus aureus (MRSA) knee prosthesis infection in rabbits, we studied the efficacies of high-dose daptomycin (22 mg/kg given intravenously [i.v.] once daily [o.d.]; equivalent to 8 mg/kg/day in humans) or vancomycin (60 mg/kg given intramuscularly [i.m.] twice daily [b.i.d.]), both either alone or with adjunctive rifampin (10 mg/kg i.m. b.i.d.). After partial knee replacement with a silicone implant, 107 MRSA CFU was injected into the knees. Treatment started 7 days postinoculation and lasted 7 days. Positive cultures were screened for the emergence of mutant strains, defined as having 3-fold-increased MICs. Although in vivo mean log10 CFU/g of daptomycintreated ( ; n 12) or vancomycin-treated ( ; n 12) crushed bone was significantly lower than that of controls ( ; n 9) (P < 0.01), neither treatment sterilized bone (2/12 and 0/12 rabbits with sterile bone, respectively). Daptomycin mutant strains were found in 6/12, 3/12, and 2/9 daptomycintreated, vancomycin-treated, and control rabbits, respectively; no resistant strains emerged (MIC was always <1 mg/liter). Adjunctive rifampin with daptomycin ( CFU/g of bone [detection threshold]; 11/11 sterile bones) or vancomycin ( CFU/g of bone; 6/8 sterile bones) was significantly more effective than monotherapy (P < 0.01) and prevented the emergence of daptomycin mutant strains. In this MRSA joint prosthesis infection model, combining rifampin with daptomycin was highly effective. Daptomycin mutant strains were isolated in vivo even without treatment, but adjunctive rifampin prevented this phenomenon, previously found after monotherapy in humans.
 knee prosthesis infection in rabbits, we studied the efficacies of high-dose daptomycin (22. mg/kg given intravenously [i.v.] once daily [o.d.]; equivalent to 8 mg/kg/day in humans) or vancomycin (60. mg/kg given intramuscularly [i.m.] twice daily [b.i.d.]), both either alone or with adjunctive rifampin (10 mg/kg. i.m. b.i.d.). After partial knee replacement with a silicone implant, 107 MRSA CFU was injected into the knees. Treatment started 7 days postinoculation and lasted 7 days. Positive cultures were screened for the emergence. of mutant strains, defined as having 3-fold-increased MICs. Although in vivo mean log10 CFU/g of daptomycintreated. ( ; n 12) or vancomycin-treated ( ; n 12) crushed bone was significantly lower. than that of controls ( ; n 9) (P < 0.01), neither treatment sterilized bone (2/12 and 0/12 rabbits. with sterile bone, respectively). Daptomycin mutant strains were found in 6/12, 3/12, and 2/9 daptomycintreated, vancomycin-treated, and control rabbits, respectively; no resistant strains emerged (MIC was always. <1 mg/liter). Adjunctive rifampin with daptomycin ( CFU/g of bone [detection threshold]; 11/11. sterile bones) or vancomycin ( CFU/g of bone; 6/8 sterile bones) was significantly more effective than. monotherapy (P < 0.01) and prevented the emergence of daptomycin mutant strains. In this MRSA joint. prosthesis infection model, combining rifampin with daptomycin was highly effective. Daptomycin mutant. strains were isolated in vivo even without treatment, but adjunctive rifampin prevented this phenomenon, previously found after monotherapy in humans.")
45
In conclusion, the daptomycin-cloxacillin combination improved
the in vitro bactericidal activity of daptomycin, especially against bacteria in the log phase of growth. Against foreign-body infection by MRSA, this combination modestly enhanced the in vivo efficacy of daptomycin alone and was less effective than daptomycin plus rifampin. In this setting, the potential benefits of adding cloxacillin to daptomycin should be especially evaluated against infections by rifampin-resistant MRSA. Further studies should compare the efficacy of this combination versus other those of alternative therapies. Despite the use of daptomycin alone at high doses (greater than 6 mg/kg of body weight/day) against difficult-to-treat infections, clinical failures and resistance appeared. Recently, the combination daptomycin-cloxacillin showed enhanced efficacy in clearing bacteremia caused by methicillin-resistant Staphylococcus aureus (MRSA). The aim of this study was to evaluate the efficacy of daptomycin at usual and high doses (equivalent to 6 and 10 mg/kg/day in humans, respectively) in combination with cloxacillin in a rat tissue cage infection model by MRSA and to compare its efficacy to that of daptomycin-rifampin. We used MRSA strain ATCC BAA-39. In the log- and stationary-phase kill curves, daptomycin-cloxacillin improved the bactericidal activity of daptomycin, especially in log phase. For in vivo studies, therapy was administered intraperitoneally for 7 days with daptomycin at 100 mg/kg/day and 45/mg/kg/day (daptomycin 100 and daptomycin 45), daptomycin 100-cloxacillin at 200 mg/kg/12 h, daptomycin 45-cloxacillin, and daptomycin 100-rifampin at 25 mg/kg/12 h. Daptomycin-rifampin was the best therapy (P<0.05). Daptomycin 45 was the least effective treatment and did not protect against the emergence of resistant strains. There were no differences between the two dosages of daptomycin plus cloxacillin in any situation, and both protected against resistance. The overall effect of the addition of cloxacillin to daptomycin was a significantly greater cure rate (against adhered bacteria) than that for daptomycin alone. In conclusion, daptomycin-cloxacillin enhanced modestly the in vivo efficacy of daptomycin alone against foreignbody infection by MRSA and was less effective than daptomycin plus rifampin. The benefits of adding cloxacillin to daptomycin should be especially evaluated against infections by rifampin-resistant MRSA and for protection against the emergence of daptomycin nonsusceptibility
 against difficult-to-treat infections, clinical failures and resistance appeared. Recently, the combination daptomycin-cloxacillin showed enhanced efficacy in clearing. bacteremia caused by methicillin-resistant Staphylococcus aureus (MRSA). The aim of this study was to evaluate the efficacy of. daptomycin at usual and high doses (equivalent to 6 and 10 mg/kg/day in humans, respectively) in combination with cloxacillin. in a rat tissue cage infection model by MRSA and to compare its efficacy to that of daptomycin-rifampin. We used MRSA strain. ATCC BAA-39. In the log- and stationary-phase kill curves, daptomycin-cloxacillin improved the bactericidal activity of daptomycin, especially in log phase. For in vivo studies, therapy was administered intraperitoneally for 7 days with daptomycin at 100. mg/kg/day and 45/mg/kg/day (daptomycin 100 and daptomycin 45), daptomycin 100-cloxacillin at 200 mg/kg/12 h, daptomycin. 45-cloxacillin, and daptomycin 100-rifampin at 25 mg/kg/12 h. Daptomycin-rifampin was the best therapy (P<0.05). Daptomycin. 45 was the least effective treatment and did not protect against the emergence of resistant strains. There were no differences. between the two dosages of daptomycin plus cloxacillin in any situation, and both protected against resistance. The overall effect. of the addition of cloxacillin to daptomycin was a significantly greater cure rate (against adhered bacteria) than that for daptomycin. alone. In conclusion, daptomycin-cloxacillin enhanced modestly the in vivo efficacy of daptomycin alone against foreignbody. infection by MRSA and was less effective than daptomycin plus rifampin. The benefits of adding cloxacillin to daptomycin. should be especially evaluated against infections by rifampin-resistant MRSA and for protection against the emergence of daptomycin. nonsusceptibility.")
46
Quelle durée de traitement antibiotique ?
2 semaines 6 semaines 3 mois 6 mois A vie

47
Quelle durée de traitement antibiotique ?
2 semaines 6 semaines 3 mois 6 mois A vie

48
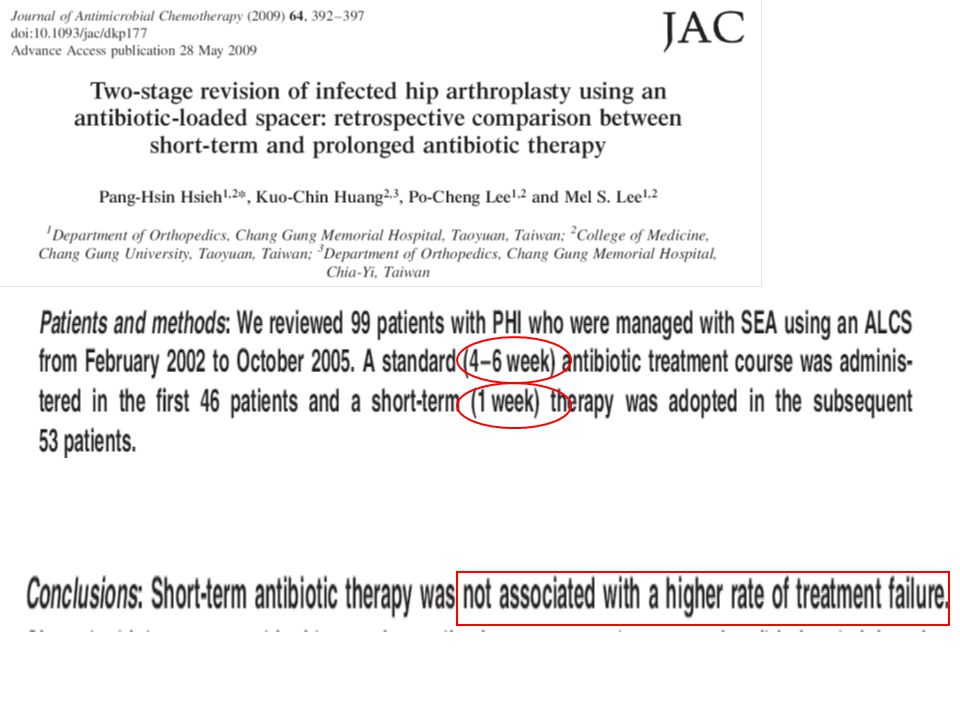
Quelle durée ? Durée du traitement antibiotique non standardisée.
Études récentes : possibilité d’une durée de traitement de 6 semaines après la dépose (PTH et PTG). En pratique courante : le plus souvent 6 à 12 semaines. Choutet P, Desplaces N, Evrard P et al. Traitement des infections ostéoarticulaires bactériennes en dehors des infections à mycobactéries. Med Mal Infect 1991 ; 21 : Bernard L, Hoffmeyer P, Assal M et al. Trends in the treatment of orthopaedic prosthetic infections. J Antimicrob Chemother 2004 ; 53 : Hoad-Reddick DA, Evans CR, Norman P, Stockley I. Is there a role for extended antibiotic therapy in a two-stage revision of the infected knee arthroplasty ? J Bone Joint Surg Br 2005 ; 87 (2) : Galpérine T, Bernard L. Antibiotic therapy of osteoarticular infections in the adult. Rev Prat 2007 ; 57 (9) :
. En pratique courante : le plus souvent 6 à 12 semaines. Choutet P, Desplaces N, Evrard P et al. Traitement des infections ostéoarticulaires bactériennes en dehors des infections à mycobactéries. Med Mal Infect 1991 ; 21 : Bernard L, Hoffmeyer P, Assal M et al. Trends in the treatment of orthopaedic prosthetic infections. J Antimicrob Chemother 2004 ; 53 : Hoad-Reddick DA, Evans CR, Norman P, Stockley I. Is there a role for extended antibiotic therapy in a two-stage revision of the infected knee arthroplasty J Bone Joint Surg Br 2005 ; 87 (2) : Galpérine T, Bernard L. Antibiotic therapy of osteoarticular infections in the adult. Rev Prat 2007 ; 57 (9) :")
50
Antibiotics for treating chronic osteomyelitis in adults (Review)
Conterno LO, da Silva Filho CR COCHRANE DATA BASE “No trials compared different durations of antibiotic treatment for chronic osteomyelitis” This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2009, Issue 3

51
Durée de traitement des IPOA : Revue de la littérature
20 Articles: - Aucune étude prospective de durée - de 15 à 186 patients par étude (total n= 1196) - 12 études avec durée 6s - 2 études avec durée 3 mois - 5 études avec durée variable 6s à 6 mois - 1 étude avec durée variable < à >6 mois
 - 12 études avec durée 6s. - 2 études avec durée 3 mois. - 5 études avec durée variable 6s à 6 mois. - 1 étude avec durée variable < à >6 mois.")
52
Durée de traitement des IPOA : Revue de la littérature
Efficacité: - entre 67% et 100% - majorité des études entre 85% et 95% - 1 étude : 67% malgré une durée 18 s mais multiples reprises - difficiles à interpréter car différentes stratégies chirurgicales

53
Recommandations USA : en cours
Suisse (Zimmerli) : PTH 3 mois, PTG 6 mois France : au moins 6 semaines ; justifier pour traitement >12 semaines si ostéo arthrite pas plus de 6 semaines Chez l’enfant : 3 semaines habituellement une étude récente validant 10 jours de traitement ATB
 : PTH 3 mois, PTG 6 mois. France : au moins 6 semaines ; justifier pour traitement >12 semaines si ostéo arthrite pas plus de 6 semaines. Chez l’enfant : 3 semaines habituellement une étude récente validant 10 jours de traitement ATB.")
56
Evolution

57
Conclusions Tendances : Nécessité de 1 temps, Durée Atb courte,
relai per os précoce Nécessité de réunion pluridisciplinaire, communication inter services et collégialité mettre en place des protocole et les évaluer

58
MERCI !

59
Merci

60
Repose et stérilité du site
Ponction-biopsie préopératoire avant réimplantation. Repose de la prothèse 15 j après l’arrêt des antibiotiques. Prélèvements profonds avant l’introduction du traitement antibiotique (comprenant l’antibioprophylaxie). Traitement antibiotique arrêté à la réception des cultures négatives des prélèvements peropératoires. En cas, exceptionnel, de positivité de ces cultures, une antibiothérapie adaptée sera poursuivie 6 à 12 semaines.
. Traitement antibiotique arrêté à la réception des cultures négatives des prélèvements peropératoires. En cas, exceptionnel, de positivité de ces cultures, une antibiothérapie adaptée sera poursuivie 6 à 12 semaines.")
Présentations similaires