Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Broncho-Pneumopathie Chronique Obstructive
GOLD : un GOLD standard ?

2
Broncho-Pneumopathie Chronique Obstructive
Combinaison variable chez un individu de lésions des voies aériennes (B) et du poumon (P) responsable d’une limitation chronique (C) (définitive en grande partie) des débits aériens Cette ou ces affection(s) se caractérise(nt) par un déficit ventilatoire obstructif (O) fixe ou peu réversible sous traitement Le tabagisme en est la cause principale
 et du poumon (P) responsable d’une limitation chronique (C) (définitive en grande partie) des débits aériens. Cette ou ces affection(s) se caractérise(nt) par un déficit ventilatoire obstructif (O) fixe ou peu réversible sous traitement. Le tabagisme en est la cause principale.")
3
Bronches : hyperproduction de mucus et dysfonction muco-ciliaire : bronchite chronique Alvéoles : destruction des parois alvéolaires, avec dilatation des espaces distaux : emphysème Bronchioles : inflammation et sténose des voies aériennes périphériques : bronchiolite

4
Phénomènes causant la réduction de calibre des voies aériennes
Inflammation et sténoses des voies aériennes périphériques Perte des attaches alvéolaires (collapsus) Contraction des muscles lisses (tonus cholinergique) Présence d’un exsudat inflammatoire et muqueux endo-luminal, œdème muqueux
 Contraction des muscles lisses (tonus cholinergique) Présence d’un exsudat inflammatoire et muqueux endo-luminal, œdème muqueux.")
5
GOLD guidelines :définition de la BPCO
Disease state characterized by airflow limitation that is not fully reversible The airflow limitation is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases GOLD guidelines 2006

6
Classification GOLD: très schématique
BPCO définie sur base d’un rapport VEMS/CVF de 70 %. Environ 30 % des non fumeurs de plus de 70 ans ont une valeur inférieure à 70 % Hardie JA et al. Eur Respir J 2002;20: Les catégories de sévérité sont ensuite uniquement basées sur la valeur en % du VEMS post-bronchodilateur (80, 50, 30 %)
")
7
Classification de la BPCO (GOLD )
Stade Caractéristiques 0 : à risque Symptômes chroniques : toux, expectoration VEMS/CV 70% I : BPCO légère VEMS/CV < 70% VEMS 80% de la valeur prédite avec ou sans symptômes chroniques (toux, expectoration) II : BPCO modérée III : BPCO sévère 50% VEMS < 80% de la valeur prédite 30% VEMS < 50% de la valeur prédite avec ou sans symptômes chroniques (toux, expectoration, dyspnée) IV : BPCO très sévère VEMS < 30% de la valeur prédite ou VEMS < 50% de la valeur prédite en présence d ’insuffisance respiratoire (PaO2 < 60 mmHg) ou de signes cliniques d'insuffisance cardiaque droite
 II : BPCO modérée. III : BPCO sévère. 50% VEMS < 80% de la valeur prédite. 30% VEMS < 50% de la valeur prédite avec ou sans symptômes chroniques (toux, expectoration, dyspnée) IV : BPCO très sévère. VEMS < 30% de la valeur prédite ou VEMS < 50% de la valeur prédite en présence d ’insuffisance respiratoire (PaO2 < 60 mmHg) ou de signes cliniques d insuffisance cardiaque droite.")
8
GOLD: critère d’obstruction
Comparaison entre % de sujets obstructifs définis selon GOLD (VEMS/CVF < 70 %) ou selon la limite inférieure des valeurs prédites (88 % H et 89 F; ERS/ATS) Surestimation diagnostic obstruction dans 58 % des cas après 50 ans Sous-estimation de 29 % avant 50 ans Le critère GOLD surestime la prévalence de la BPCO chez les personnes âgées et la sous-estime chez les personnes jeunes Hnizdo E et al. COPD 2006;3:95-100
 ou selon la limite inférieure des valeurs prédites (88 % H et 89 F; ERS/ATS) Surestimation diagnostic obstruction dans 58 % des cas après 50 ans. Sous-estimation de 29 % avant 50 ans. Le critère GOLD surestime la prévalence de la BPCO chez les personnes âgées et la sous-estime chez les personnes jeunes. Hnizdo E et al. COPD 2006;3:")
9
BPCO Maladie complexe, hétérogène, à composantes multiples
Divers phénotypes: réversibilité importante ou non, présence d’un emphysème ou non, exacerbations fréquentes ou non.. Une seule ou plusieurs maladies ?

10
Classification GOLD: très schématique
Des patients de la même catégorie de sévérité selon le VEMS peuvent avoir des maladies très différentes, mais bénéficient (?) du même traitement La notion de réversibilité est très floue La valeur pronostique des symptômes au stade 0 n’est pas démontrée. (BPCO après 15 ans chez 20,5% des fumeurs symptomatiques et 18,5% des fumeurs asymptomatiques) Vestbo J & Lange P. Am J Respir Crit Care Med 2002;166:329-32
 du même traitement. La notion de réversibilité est très floue. La valeur pronostique des symptômes au stade 0 n’est pas démontrée. (BPCO après 15 ans chez 20,5% des fumeurs symptomatiques et 18,5% des fumeurs asymptomatiques) Vestbo J & Lange P. Am J Respir Crit Care Med 2002;166:")
11
Evaluation du patient La mesure du VEMS et du rapport VEMS/CV reste centrale dans le diagnostic et dans le pronostic vital Le VEMS est cependant peu corrélé avec les symptômes, la capacité d’effort ou la qualité de vie

12
Autres critères d’évaluation
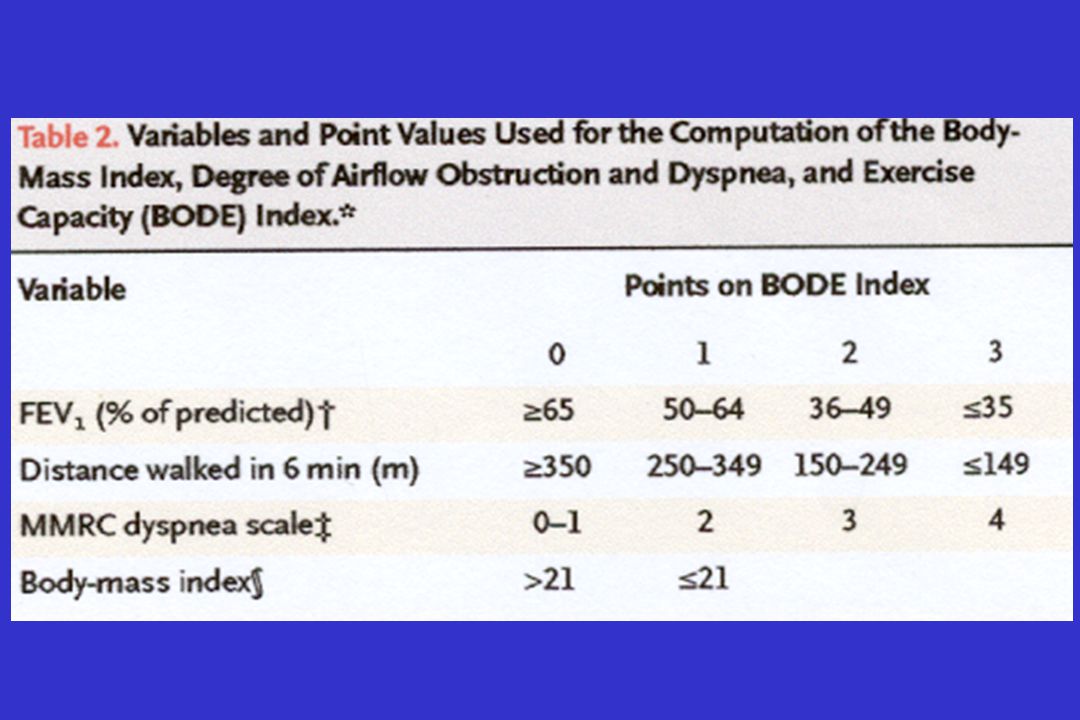
Nombre d’exacerbations Test marche 6 minutes HRQL BODE index : score composite utilisant body mass index (B), degré d’obstruction (O), dyspnée (D) et capacité d’effort (E) Celli BR et al. NEJM 2004;350:
, degré d’obstruction (O), dyspnée (D) et capacité d’effort (E) Celli BR et al. NEJM 2004;350:")
15
BPCO : « maladie systémique »
Les processus inflammatoires impliqués dans la BPCO peuvent « déborder » du poumon (cytokines pro-inflammatoires) Cette inflammation systémique pourrait jouer un rôle dans les complications extra-pulmonaires de la BPCO
 Cette inflammation systémique pourrait jouer un rôle dans les complications extra-pulmonaires de la BPCO.")
16
BPCO : « maladie systémique »
Des co-morbidités sont fréquemment associées à la BPCO et contribuent à la sévérité de la maladie et à sa mortalité Hormis un étiologie commune ou un effet du traitement , l’inflammation systémique associée à la BPCO joue-t-elle un rôle causal dans ces co-morbidités ?

17
BPCO : « maladie systémique »
Si l’inflammation systémique joue un rôle dans les co-morbidités associées et si un traitement anti-inflammatoire efficace est disponible dans la BPCO, il pourrait avoir un effet sur ces co-morbidités aussi

18
Biomarqueurs dans la BPCO
Locaux invasifs : sputum induit, (IL 6, TNF alpha, TGF beta, profil cytologique), LBA, biopsies Locaux non-invasifs: NO, condensats air exhalé (LTB4, peroxynitrile, isoprostanes). « Electronic nose » dans le futur Systémiques : sang (CRP,TNF …)
, LBA, biopsies. Locaux non-invasifs: NO, condensats air exhalé (LTB4, peroxynitrile, isoprostanes). « Electronic nose » dans le futur. Systémiques : sang (CRP,TNF …)")
19
Systemic Inflammation in COPD: C-reactive Protein
Dentener Eid Mannino Mendall Yasuda Speaker notes A systematic review identified 14 studies which reported on the relationship between COPD, FEV1 or FVC, and levels of systemic inflammatory markers: C-reactive protein (CRP), fibrinogen, leucocytes, TNF-a, and IL-6 and -8. Overall, the standardized mean difference in the CRP level between COPD and control subjects was 0.53 units (95% CI 0.34 to 0.72). The finding of elevated CRP is consistent with the presence of systemic inflammation in patients with stable COPD, and may explain, at least in part, the high prevalence of systemic complications such as cachexia, osteoporosis, and cardiovascular diseases among patients with COPD. Reference Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: Pooled summary -0.2 0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0 Standardized mean difference of CRP Greater in controls Greater in COPD Gan et al. Thorax 2004; 59: Copyright © 2004 BMJ Publishing Group Limited. All rights reserved.
, fibrinogen, leucocytes, TNF-a, and IL-6 and -8. Overall, the standardized mean difference in the CRP level between COPD and control subjects was 0.53 units (95% CI 0.34 to 0.72). The finding of elevated CRP is consistent with the presence of systemic inflammation in patients with stable COPD, and may explain, at least in part, the high prevalence of systemic complications such as cachexia, osteoporosis, and cardiovascular diseases among patients with COPD. Reference. Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: Pooled summary Standardized mean difference of CRP. Greater. in controls. Greater in COPD. Gan et al. Thorax 2004; 59: Copyright © 2004 BMJ Publishing Group Limited. All rights reserved.")
20
CRP is Elevated in Patients with COPD versus Smokers and Nonsmokers
* Speaker notes Patients with chronic obstructive pulmonary disease (COPD) have elevated serum levels of C reactive protein (CRP). This may be related directly to COPD and its associated systemic inflammation or secondary to other factors such as concomitant ischemic heart disease (IHD) or smoking status. Cross-sectional analyses comparing cohorts of 88 patients with COPD, 33 smokers, and 38 non-smoker controls were performed to evaluate these relationships. Serum CRP levels were significantly higher in patients with COPD than in controls, but were similar in the two control groups (smokers and nonsmokers). These results indicate that CRP levels are raised in COPD patients independent of cigarette smoking. Reference Pinto-Plata VM, Mullerova H, Toso JF, et al. C-reactive protein in patients with COPD, control smokers and non-smokers. Thorax. 2006;61:23-28. * P < .05 versus other groups Pinto-Plata et al. Thorax 2006; 61: 23-28
 have elevated serum levels of C reactive protein (CRP). This may be related directly to COPD and its associated systemic inflammation or secondary to other factors such as concomitant ischemic heart disease (IHD) or smoking status. Cross-sectional analyses comparing cohorts of 88 patients with COPD, 33 smokers, and 38 non-smoker controls were performed to evaluate these relationships. Serum CRP levels were significantly higher in patients with COPD than in controls, but were similar in the two control groups (smokers and nonsmokers). These results indicate that CRP levels are raised in COPD patients independent of cigarette smoking. Reference. Pinto-Plata VM, Mullerova H, Toso JF, et al. C-reactive protein in patients with COPD, control smokers and non-smokers. Thorax. 2006;61: * P < .05 versus other groups. Pinto-Plata et al. Thorax 2006; 61:")
21
Systemic Inflammation in COPD: TNF-a
de Godoy Di Francia Takabatake Yasuda Speaker notes A systematic review identified 14 studies which reported on the relationship between COPD, FEV1 or FVC, and levels of systemic inflammatory markers: C-reactive protein (CRP), fibrinogen, leucocytes, TNF-a, and IL-6 and -8. Serum TNF-a levels were higher in patients with COPD than in control subjects: standardized mean difference of 0.59 units (95% CI 0.29 to 0.89). The finding of elevated TNF-a is consistent with the presence of systemic inflammation in patients with stable COPD, and may explain, at least in part, the high prevalence of systemic complications such as cachexia, osteoporosis, and cardiovascular diseases among patients with COPD. Reference Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: Pooled summary -0.4 -0. 2 0.0 0.2 0.4 .06 .08 1.0 1.2 1.4 Standardized mean difference of TNF-alpha Greater in controls Greater in COPD Gan et al. Thorax 2004; 59: Copyright © 2004 BMJ Publishing Group Limited. All rights reserved.
, fibrinogen, leucocytes, TNF-a, and IL-6 and -8. Serum TNF-a levels were higher in patients with COPD than in control subjects: standardized mean difference of 0.59 units (95% CI 0.29 to 0.89). The finding of elevated TNF-a is consistent with the presence of systemic inflammation in patients with stable COPD, and may explain, at least in part, the high prevalence of systemic complications such as cachexia, osteoporosis, and cardiovascular diseases among patients with COPD. Reference. Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: Pooled summary Standardized mean difference of TNF-alpha. Greater. in controls. Greater in COPD. Gan et al. Thorax 2004; 59: Copyright © 2004 BMJ Publishing Group Limited. All rights reserved.")
22
Systemic Inflammation in COPD: Fibrinogen
Alessandri Engstrom (smokers) Mannino Pooled summary Standardized mean difference of TNF-alpha Greater in controls Greater in COPD 1.6 -0. 2 0.0 0.2 0.4 .06 .08 1.0 1.2 1.4 Dahl (smokers) Speaker notes A systematic review identified 14 studies which reported on the relationship between COPD, FEV1 or FVC, and levels of systemic inflammatory markers: C-reactive protein (CRP), fibrinogen, leucocytes, TNF-a, and IL-6 and -8. The standardized mean difference for patients with COPD versus control subjects in the fibrinogen level was 0.47 units (95% CI 0.29 to 0.65). The finding of elevated fibrinogen is consistent with the presence of systemic inflammation in patients with stable COPD, and may explain, at least in part, the high prevalence of systemic complications such as cachexia, osteoporosis, and cardiovascular diseases among patients with COPD. Reference Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: Gan et al. Thorax 2004; 59: Copyright © 2004 BMJ Publishing Group Limited. All rights reserved.
 Mannino. Pooled summary. Standardized mean difference of TNF-alpha. Greater. in controls. Greater in COPD Dahl (smokers) Speaker notes. A systematic review identified 14 studies which reported on the relationship between COPD, FEV1 or FVC, and levels of systemic inflammatory markers: C-reactive protein (CRP), fibrinogen, leucocytes, TNF-a, and IL-6 and -8. The standardized mean difference for patients with COPD versus control subjects in the fibrinogen level was 0.47 units (95% CI 0.29 to 0.65). The finding of elevated fibrinogen is consistent with the presence of systemic inflammation in patients with stable COPD, and may explain, at least in part, the high prevalence of systemic complications such as cachexia, osteoporosis, and cardiovascular diseases among patients with COPD. Reference. Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: Gan et al. Thorax 2004; 59: Copyright © 2004 BMJ Publishing Group Limited. All rights reserved.")
23
Marqueurs de sévérité dans la BPCO
Méta-analyse (146,255 patients) Marqueurs montrant une tendance à discriminer les différents stades de BPCO - PaO2 - Neutrophiles et IL8 dans le sputum - Taux sériques de TNF alpha et CRP Franciosi LG et al. Pulm Pharmacol Ther 2006; 19:
 Marqueurs montrant une tendance à discriminer les différents stades de BPCO. - PaO2. - Neutrophiles et IL8 dans le sputum. - Taux sériques de TNF alpha et CRP. Franciosi LG et al. Pulm Pharmacol Ther 2006; 19:")
24
Franciosi LG et al. Pulm Pharmacol Ther 2006; 19: 189-199

25
Systemic Inflammation Rises with COPD Severity
CRP TNF-a Severe COPD Severe COPD Moderate COPD Moderate COPD Speaker notes Review of clinical study databases was conducted to determine how existing clinical and laboratory measures change with COPD severity and to identify disease markers that can serve as better endpoints for diagnosis and assessment of COPD progression and treatment effect. A meta-analysis of 652 studies comprising 146,255 enrollees showed trends in serum TNF-a and CRP toward separation between COPD stages. Serum concentrations of CRP showed no statistical differences between the healthy subjects and those for individuals at each of the COPD stages but showed an upward trend with increasing disease severity. For serum TNF-a, there was a similar trend for increasing level with increasing level of COPD severity, but there were no statistically significant differences between the healthy subjects and any of the COPD stages. Reference Franciosi LG, Page CP, Celli BR, et al. Markers of disease severity in chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2006;19: Mild COPD Mild COPD Healthy Healthy 10 20 30 40 50 60 70 20 40 60 80 100 Serum C-Reactive Protein (mg/L) Serum TNF-Alpha (pg/mL) Franciosi et al. Pulm Pharmacol Ther 2006; 19: 5.25
 Serum TNF-Alpha (pg/mL) Franciosi et al. Pulm Pharmacol Ther 2006; 19:")
26
CRP et BPCO Protéine de la phase aiguë, activatrice du complément, produite par le foie (et localement) en réponse à l’IL 6. Cellules épithéliales et macrophages produisent IL6, activant lymphocytes T et B, PNN et macrophages CRP plasmatique peut donc refléter inflammation pulmonaire médiée par IL 6 conduisant à progression de la BPCO Dahl M et al. Am J Respir Crit Care Med 2007; 175:

27
Valeur pronostique de la CRP dans la BPCO
Suivi médian de 8 ans de 1,302 BPCO Risque d’hospitalisations et de mortalité augmente si CRP supérieure à 3 mg/L Une CRP sup. à 3 mg/l augmente le risque d’hospitalisation et de décès respectivement de 54% et 57% chez BPCO fumeurs de plus de 70 ans avec un VEMS sous 50% Dahl M et al. Am J Respir Crit Care Med 2007; 175:

28
Dosage de la CRP au départ
Hospitalisation pour BPCO Décès dû à la BPCO Incidence cumulée Log-rank: Test logarithmique par rang mg/L mg/l Âge Dahl M et al. Am j Respir Crit Care Med 2007; 175:

29
Valeur pronostique de la CRP dans la BPCO
Taux sériques de CRP chez 4,803 BPCO Mortalité (toutes causes confondues) : 4 x plus élevée dans quintile avec CRP la plus élevée (moy mg/L) que dans quintile avec CRP la plus basse (moy mg/L) CRP est un facteur pronostique pouvant aider à détecter les patients à haut risque de mortalité Man SF et al. Thorax 2006; 61:
 : 4 x plus élevée dans quintile avec CRP la plus élevée (moy mg/L) que dans quintile avec CRP la plus basse (moy mg/L) CRP est un facteur pronostique pouvant aider à détecter les patients à haut risque de mortalité. Man SF et al. Thorax 2006; 61:")
30
Conclusion La protéine C réactive (CRP) est un marqueur de détérioration plus rapide, d’hospitalisations plus fréquentes et de mortalité chez les patients BPCO
 est un marqueur de détérioration plus rapide, d’hospitalisations plus fréquentes et de mortalité chez les patients BPCO.")
31
Valeur pronostique de la CRP dans la BPCO
Facteurs génétiques pourraient intervenir dans la concentration sérique de CRP La CRP pourrait être un marqueur d’une sensibilité accrue à une baisse de la fonction respiratoire, éventuellement "boostée" par le tabagisme La BPCO surviendrait donc préférentiellement chez des sujets à CRP élevée Hersh CP et al. Eur Respir J 2006; 28:

32
Relation inverse entre fonction pulmonaire et CRP
1131 sujets sans maladie respiratoire 8.5 % EFR « anormales » (VEMS moins de 80 % VP) Relation inverse et linéaire entre taux de CRP et mesures des volumes pulmonaires y compris chez non fumeurs Aronson D et al. AJRCCM 2006
 Relation inverse et linéaire entre taux de CRP et mesures des volumes pulmonaires y compris chez non fumeurs. Aronson D et al. AJRCCM")
33
Comorbidities in COPD Cardiovascular Metabolic Orthopedic
Angina CHF Arrhythmias Hypertension Metabolic Diabetes Obesity Orthopedic Osteoporosis Locomotive Gastrointestinal Ulcer Disease Hematologic Malignancies Anemia Psychiatric Depression Insomnia Ophthalmologic Cataracts Speaker notes Assessment of patients with COPD has revealed that they are at increased risk, relative to the general population, for a wide range of systemic comorbidities.1,2 These include cardiovascular conditions, such as angina, congestive heart failure (CHF), arrhythmias, and hypertension; metabolic diseases, such as diabetes and obesity; osteoporosis; increased risk for ulcers; malignancies; depression and insomnia; and cataracts.1-3 References 1. Agusti AG, Noguera A, Sauleda J, Sala E, Pons J, Busquets X. Systemic effects of chronic obstructive pulmonary disease. Eur Respir J. 2003;21: 2. Sevenoaks MJ, Stockley RA. Chronic Obstructive Pulmonary Disease, inflammation and co-morbidity--a common inflammatory phenotype? Respir Res. 2006;7:70-78. 3. Gartlehner G, Hansen RA, Carson SS, Lohr KN. Efficacy and safety of inhaled corticosteroids in patients with COPD: a systematic review and meta-analysis of health outcomes. Ann Fam Med. 2006;4: Agusti et al. Eur Respir J 2003; 21: ; Sevenoaks, Stockley. Respir Res 2006; 7: 70-78
, arrhythmias, and hypertension; metabolic diseases, such as diabetes and obesity; osteoporosis; increased risk for ulcers; malignancies; depression and insomnia; and cataracts.1-3. References. 1. Agusti AG, Noguera A, Sauleda J, Sala E, Pons J, Busquets X. Systemic effects of chronic obstructive pulmonary disease. Eur Respir J. 2003;21: Sevenoaks MJ, Stockley RA. Chronic Obstructive Pulmonary Disease, inflammation and co-morbidity--a common inflammatory phenotype Respir Res. 2006;7: Gartlehner G, Hansen RA, Carson SS, Lohr KN. Efficacy and safety of inhaled corticosteroids in patients with COPD: a systematic review and meta-analysis of health outcomes. Ann Fam Med. 2006;4: Agusti et al. Eur Respir J 2003; 21: ; Sevenoaks, Stockley. Respir Res 2006; 7:")
34
Comorbidités et BPCO Facteurs causaux communs (tabagisme)
Mécanismes divers possibles: mécaniques (remplissage cardiaque, fractures ostéoporotiques), hypoxémie tissulaire Interférences traitements (CST et ostéoporose, moins de bloquants prescrits si BPCO) Versus (ou en plus) Facteurs inflammatoires communs
, hypoxémie tissulaire. Interférences traitements (CST et ostéoporose, moins de bloquants prescrits si BPCO) Versus (ou en plus) Facteurs inflammatoires communs.")
35
BPCO : co-morbidités Maladies cardiovasculaires Ostéoporose
Dysfonction musculaire Diabète Anémie Maladies digestives

36
COPD and risk of CVD 6629 sujets
Corrélation entre obstruction et taux CRP En présence d’une CRP élevée : Cardiac Infarction Injury Score (CIIS) multiplié par 2.7 si BPCO modérée et 5.9 si BPCO sévère Sin and Man. Circulation 2003
 multiplié par 2.7 si BPCO modérée et 5.9 si BPCO sévère. Sin and Man. Circulation")
37
Risk for Ischemic Heart Disease and Pulmonary Function
1.56 1.48 1.55 1.15 1 1.88 1.5 1.22 1.01 0.2 0.4 0.6 0.8 1.2 1.4 1.6 1.8 2 First Second Third Fourth Fifth Relative Hazard Ratio Men Women P < 0.05 for trend in both men and women Speaker notes A prospective general population study in 7,058 men and 8,353 women assessed the relation between FEV1 and subsequent mortality over 15 years of follow-up. Significant trends of increasing risk with diminishing FEV1 were apparent for both sexes for all the causes of death examined after adjustment for age, cigarette smoking, diastolic blood pressure, cholesterol concentration, BMI, and social class. Results plotted in this slide document elevated hazard ratios for ischemic heart disease in men and women across successive quintiles of impaired lung function. The relative hazard ratios for all cause mortality for subjects in the lowest fifth of the FEV1 distribution were 1.92 (95% CI 1.68 to 2.20) for men and 1.89 (95% CI 1.63 to 2.20) for women. Reference Hole DJ, Watt GC, Davey-Smith G, Hart CL, Gillis CR, Hawthorne VM. Impaired lung function and mortality risk in men and women: findings from the Renfrew and Paisley prospective population study. BMJ. 1996;313: Increasing FEV1 FEV1 Quintile P < .001 for trend in both sexes Hole et al. BMJ 1996; 313: (15400 patients)
 for men and 1.89 (95% CI 1.63 to 2.20) for women. Reference. Hole DJ, Watt GC, Davey-Smith G, Hart CL, Gillis CR, Hawthorne VM. Impaired lung function and mortality risk in men and women: findings from the Renfrew and Paisley prospective population study. BMJ. 1996;313: Increasing FEV1. FEV1 Quintile. P < .001 for trend in both sexes. Hole et al. BMJ 1996; 313: (15400 patients)")
38
Athérosclérose et BPCO
Aspects communs de physiopathologie : médiateurs (MMP, LTB4), TGF beta (fibrose PVA et hyperplasie intima), inflammation, rétrécissement lumière organe, rupture (plaque/emphysème)
, TGF beta (fibrose PVA et hyperplasie intima), inflammation, rétrécissement lumière organe, rupture (plaque/emphysème)")
39
Maladie périodontale Inflammation chronique et fibrose gingivale
Facteur de risque d’infarctus et d’athérosclérose Modèle d’inflammation locale avec effets systémiques Production locale de leucotriènes (LTB4) retrouvés dans les « lavages » gingivaux Corrélation avec plaques athéroscléreuses carotidiennes Bäck et al Atherosclerosis 2007
 retrouvés dans les « lavages » gingivaux. Corrélation avec plaques athéroscléreuses carotidiennes. Bäck et al Atherosclerosis")
40
BPCO : co-morbidités Ostéoporose Maladies cardiovasculaires
Dysfonction musculaire Diabète et anomalies métaboliques Anémie Maladies digestives

41
Airflow Obstruction and Osteoporosis in COPD
1.9 3.9 6.8 11 7.6 10.3 20.9 26 5 10 15 20 25 30 None Mild Moderate Severe Severity of Airflow Obstruction (GOLD) Percent of Subjects with Osteoporosis (BMD) Men Women Speaker notes Data from subjects (N = 9,502) in the Third National Health and Nutrition Examination Survey, conducted in the US between 1988 and 1994, were used along with total bone mineral density (BMD) measurements to determine whether osteoporosis (defined as total BMD values 2.5 SD below the corresponding mean values from young, healthy participants) was associated with COPD. Airflow obstruction was classified as none (FEV1/FCV 0.7), versus mild (FEV1 80% predicted), moderate (FEV1 50% to 80% predicted), and severe (FEV1 <50% predicted). Overall, airflow obstruction was associated with increased odds of osteoporosis compared with without airflow obstruction (Odds Ratio [OR] 1.9; 95% CI 1.4 to 2.5). Participants with severe airflow obstruction were at especially increased risk (OR 2.4; 95% CI 1.3 to 4.4). Moderate, but not mild, airflow obstruction was also associated with osteoporosis. For women and men evaluated separately, the trends for increased prevalence of osteoporosis with increased severity of airflow obstruction were statistically significant (P<0.005 for both). Reference Sin DD, Man JP, Man SF. The risk of osteoporosis in Caucasian men and women with obstructive airways disease. Am J Med. 2003;114:10-14. Sin et al. Am J Med 2003; 114:
 Percent of Subjects with. Osteoporosis (BMD) Men. Women. Speaker notes. Data from subjects (N = 9,502) in the Third National Health and Nutrition Examination Survey, conducted in the US between 1988 and 1994, were used along with total bone mineral density (BMD) measurements to determine whether osteoporosis (defined as total BMD values 2.5 SD below the corresponding mean values from young, healthy participants) was associated with COPD. Airflow obstruction was classified as none (FEV1/FCV 0.7), versus mild (FEV1 80% predicted), moderate (FEV1 50% to 80% predicted), and severe (FEV1 <50% predicted). Overall, airflow obstruction was associated with increased odds of osteoporosis compared with without airflow obstruction (Odds Ratio [OR] 1.9; 95% CI 1.4 to 2.5). Participants with severe airflow obstruction were at especially increased risk (OR 2.4; 95% CI 1.3 to 4.4). Moderate, but not mild, airflow obstruction was also associated with osteoporosis. For women and men evaluated separately, the trends for increased prevalence of osteoporosis with increased severity of airflow obstruction were statistically significant (P<0.005 for both). Reference. Sin DD, Man JP, Man SF. The risk of osteoporosis in Caucasian men and women with obstructive airways disease. Am J Med. 2003;114: Sin et al. Am J Med 2003; 114:")
42
Ostéoporose: « emphysème de l’os »
Remodelling permanent (résorption et reconstruction) de l’os par ostéoclastes et ostéoblastes Inflammation dans l’ostéoporose: TNF,IL 1 et Ginaldi et al. Immunity and Aging 2005; 2: 14-18 Rôle des Receptor Activator of NFB (RANK) et de l’Ostéoprotégérine (superfamille des récepteurs du TNF) Vega et al J Clin Endocrinol Metab 2007 Ostéoprotégérine (OPG) contrôle les ostéoclastes
 de l’os par ostéoclastes et ostéoblastes. Inflammation dans l’ostéoporose: TNF,IL 1 et 6 Ginaldi et al. Immunity and Aging 2005; 2: Rôle des Receptor Activator of NFB (RANK) et de l’Ostéoprotégérine (superfamille des récepteurs du TNF) Vega et al J Clin Endocrinol Metab Ostéoprotégérine (OPG) contrôle les ostéoclastes.")
43
Ostéoprotégérine et BPCO
OPG mesurée dans le sputum induit Augmentée dans les expectorations des patients BPCO OPG corrélée avec le VEMS et avec l’hyperinflation chez les patients BPCO Austin P et al. D11: A646 ATS 2007

44
Lésions de la matrice extracellulaire
L’OPG est probablement un médiateur impliqué dans le remaniement de la matrice extracellulaire dans la BPCO L’OPG la production de MMP-9 par les macrophages Osteoprotégérine MMP-9 Lésions de la matrice extracellulaire

45
BPCO : co-morbidités Dysfonction musculaire Maladies cardiovasculaires
Ostéoporose Dysfonction musculaire Diabète et anomalies métaboliques Anémie Maladies digestives

46
Skeletal Muscle Apoptosis in COPD
Healthy Subject COPD Patient Speaker Notes Patients with COPD often lose weight during the course of their disease and this may be due to skeletal muscle apoptosis. Quadriceps femoris biopsies in 15 patients with COPD (8 with normal body mass index [BMI] and 7with low [<20 kg/m2] BMI), 8 healthy volunteers, and 6 sedentary subjects undergoing orthopedic surgery (both groups with normal BMI) indicated that skeletal muscle apoptosis (as demonstrated by TUNEL staining) was increased in patients with COPD and low BMI as compared with the other three groups (P=0.005). Reference Agusti AG, Sauleda J, Miralles C, et al. Skeletal muscle apoptosis and weight loss in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166: Nucleus of apoptotic muscle fiber Agusti et al. Am J Resp Crit Care Med 2002; 166:
, 8 healthy volunteers, and 6 sedentary subjects undergoing orthopedic surgery (both groups with normal BMI) indicated that skeletal muscle apoptosis (as demonstrated by TUNEL staining) was increased in patients with COPD and low BMI as compared with the other three groups (P=0.005). Reference. Agusti AG, Sauleda J, Miralles C, et al. Skeletal muscle apoptosis and weight loss in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166: Nucleus of apoptotic muscle fiber. Agusti et al. Am J Resp Crit Care Med 2002; 166:")
47
Fat-free Mass is Reduced in COPD
* Speaker notes Eighty-six males (40 stable COPD and 46 healthy subjects) over 65 years old were studied. Fat-free mass and appendicular skeletal muscle mass were measured by dual energy X-ray absorptiometry. COPD patients had a lower FFM both expressed in kilograms and after correction for height squared. Reference Sergi G, Coin A, Marin S, et al. Body composition and resting energy expenditure in elderly male patients with chronic obstructive pulmonary disease. Respir Med. 2006;100: * P < 0.05 Sergi et al. Respir Med 2006; 100:
 over 65 years old were studied. Fat-free mass and appendicular skeletal muscle mass were measured by dual energy X-ray absorptiometry. COPD patients had a lower FFM both expressed in kilograms and after correction for height squared. Reference. Sergi G, Coin A, Marin S, et al. Body composition and resting energy expenditure in elderly male patients with chronic obstructive pulmonary disease. Respir Med. 2006;100: * P < Sergi et al. Respir Med 2006; 100:")
48
Relationship between Skeletal Muscle Mass and Inflammatory Markers in COPD
* * Speaker notes Eighty patients with clinically stable COPD were studied in order to assess the association between body composition and the inflammatory response. Body composition was determined anthropometrically, and skeletal muscle mass was determined as the creatinine-height index (CHI). Additional assessments included nitrogen balance, and circulating concentrations of IL-6, TNF-, and their soluble receptors (SR). Body mass index was normal (>20 kg/m2) in 55 patients, of whom 17 (31%) had a low CHI (<80% predicted). A reduced CHI was associated with significantly increased circulating levels of IL-6 (P=0.001), TNF- (P =0.032) and their respective SRs (P=0.002 for IL-6 SR, P=0.03 for TNF- SR1, and P=0.001 TNF- SR2). Serum levels of CRP were also increased with low CHI but not significantly. Patients with a normal BMI and low CHI showed levels of inflammatory mediators similar to those in patients with a low BMI and CHI; both were significantly greater than in those with a normal BMI and CHI. Additional Information Skeletal muscle loss in COPD is probably multifactorial in origin, but these data suggest a link with systemic inflammation, even without weight loss. Reference Eid AA, Ionescu AA, Nixon LS, et al. Inflammatory response and body composition in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164: CHI = creatinine height index, a measure of skeletal muscle mass. Normal CHI 80% predicted, Low CHI < 80% predicted.* P < .05 for between-group difference Eid et al. Am J Respir Crit Care Med 2001; 164:
. Additional assessments included nitrogen balance, and circulating concentrations of IL-6, TNF-, and their soluble receptors (SR). Body mass index was normal (>20 kg/m2) in 55 patients, of whom 17 (31%) had a low CHI (<80% predicted). A reduced CHI was associated with significantly increased circulating levels of IL-6 (P=0.001), TNF- (P =0.032) and their respective SRs (P=0.002 for IL-6 SR, P=0.03 for TNF- SR1, and P=0.001 TNF- SR2). Serum levels of CRP were also increased with low CHI but not significantly. Patients with a normal BMI and low CHI showed levels of inflammatory mediators similar to those in patients with a low BMI and CHI; both were significantly greater than in those with a normal BMI and CHI. Additional Information. Skeletal muscle loss in COPD is probably multifactorial in origin, but these data suggest a link with systemic inflammation, even without weight loss. Reference. Eid AA, Ionescu AA, Nixon LS, et al. Inflammatory response and body composition in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164: CHI = creatinine height index, a measure of skeletal muscle mass. Normal CHI 80% predicted, Low CHI < 80% predicted.* P < .05 for between-group difference. Eid et al. Am J Respir Crit Care Med 2001; 164:")
49
BPCO : co-morbidités Diabète et anomalies métaboliques
Maladies cardiovasculaires Ostéoporose Dysfonction musculaire Diabète et anomalies métaboliques Anémie Maladies digestives

50
Prevalence of Metabolic Syndrome in COPD
Speaker notes Thirty-eight COPD patients in a cardiopulmonary rehabilitation program (mean FEV1 = 43 16% predicted) and 34 control participants matched for age and gender were studied to evaluate the presence of metabolic syndrome in COPD patients. The criteria for the identification of the metabolic syndrome included 3 or more of the following features: abdominal obesity (waist circumference: >102 cm in men, >88 cm in women), triglycerides level (1.69 mmol/L), high-density lipoprotein cholesterol level (<1.0 mmol/L in men, <1.3 mmol/L in women), blood pressure (130/85 mm Hg), and fasting glucose level (6.1 mmol/L). Three or more determinants of the metabolic syndrome were present in 47% of COPD patients versus 21% of control participants. Reference Marquis K, Maltais F, Duguay V, et al. The metabolic syndrome in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2005;25: * Metabolic syndrome 3 of the following: abdominal obesity, elevated triglycerides, reduced HDL-C, hypertension, hyperglycemia Marquis et al. J Cardiopulm Rehabil 2005; 25:
 and 34 control participants matched for age and gender were studied to evaluate the presence of metabolic syndrome in COPD patients. The criteria for the identification of the metabolic syndrome included 3 or more of the following features: abdominal obesity (waist circumference: >102 cm in men, >88 cm in women), triglycerides level (1.69 mmol/L), high-density lipoprotein cholesterol level (<1.0 mmol/L in men, <1.3 mmol/L in women), blood pressure (130/85 mm Hg), and fasting glucose level (6.1 mmol/L). Three or more determinants of the metabolic syndrome were present in 47% of COPD patients versus 21% of control participants. Reference. Marquis K, Maltais F, Duguay V, et al. The metabolic syndrome in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2005;25: * Metabolic syndrome 3 of the following: abdominal obesity, elevated triglycerides, reduced HDL-C, hypertension, hyperglycemia. Marquis et al. J Cardiopulm Rehabil 2005; 25:")
51
Effets Corticoïdes Patients BPCO legers à modérés. Effets des CST inhalés (fluticasone 2 x 500 µg) et per os sur taux de CRP Chute des taux de CRP de 50 % (inh.) et de 63 % (p.o.) Sin DD et al. AJRCCM 2004 Dans TORCH, on diminue la mortalité cardio-vasculaire par le traitement combiné ( ! ) CST/LABA très loin du site de dépôt
 et de 63 % (p.o.) Sin DD et al. AJRCCM Dans TORCH, on diminue la mortalité cardio-vasculaire par le traitement combiné ( ! ) CST/LABA très loin du site de dépôt.")
52
Rôle potentiel des statines dans la BPCO
Les statines exercent des effets anti-inflammatoires 185 patients atteints de BPCO 90 sous statines 95 ne prenant pas de statines Pas de statine Statine p < 0,001 1,59 (nombre moyen par an) Exacerbations 0,41 L’utilisation de statines est associée à une plus faible incidence d’exacerbations dans la BPCO Blamoun A et al. ATS 2007; poster A53:A135
 Exacerbations. 0,41. L’utilisation de statines est associée à une plus faible incidence d’exacerbations dans la BPCO. Blamoun A et al. ATS 2007; poster A53:A135.")
53
Conclusion et perspectives
Champ d’investigation clinique majeur Modification de la dénomination ? Devons-nous (re)devenir des internistes ?
devenir des internistes")
57
Diagnostic components of « chronic systemic inflammatory syndrome »
Age older than 40 years Smoking for more than 10 pack-years Symptoms and abnormal lung function compatible with COPD Chronic heart failure Metabolic syndrome Increased C-reactive protein At least three components are needed for diagnosis

Présentations similaires












 artérielle(s) pulmonaire(s)>")








